Hemorrhage explain for 6 Mark answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete, structured 6-mark answer on Hemorrhage based on Robbins & Kumar Basic Pathology:
Hemorrhage
Definition
Hemorrhage is defined as the extravasation (escape) of blood from blood vessels into the surrounding tissues or body cavities. It results from damage to blood vessel walls and may be exacerbated by defects in blood clotting.
Causes
- Trauma - physical injury to vessel walls
- Atherosclerosis - weakening of vessel walls by disease
- Inflammatory or neoplastic erosion of a vessel wall
- Chronic congestion - allows capillary bleeding
- Hemorrhagic diatheses - inherited or acquired defects in vessel walls, platelets, or coagulation factors (e.g., thrombocytopenia, haemophilia, vitamin C deficiency/scurvy)
Morphological Forms / Types
| Type | Size | Description |
|---|---|---|
| Petechiae | 1-2 mm | Minute hemorrhages in skin, mucous membranes, or serosal surfaces. Caused by thrombocytopenia, defective platelet function, or loss of vascular wall support (e.g., scurvy) |
| Purpura | 3-5 mm | Slightly larger hemorrhages. Caused by same disorders as petechiae, plus trauma, vasculitis, or increased vascular fragility |
| Ecchymoses | 1-2 cm | Subcutaneous hematomas ("bruises"). Color changes occur: red-blue (hemoglobin) → blue-green (bilirubin) → golden-brown (hemosiderin) |
| Hematoma | Variable | Accumulation of blood within a tissue (e.g., retroperitoneal hematoma from ruptured aortic aneurysm) |
| Cavity bleeds | Large | Named by location - hemothorax, hemopericardium, hemoperitoneum, hemarthrosis |
Clinical Significance
The clinical impact depends on four factors:
- Volume of blood lost - Rapid loss of >20% blood volume causes hemorrhagic (hypovolemic) shock; up to 20% may be tolerated in healthy adults
- Rate of bleeding - Rapid bleeding is less tolerated than slow, chronic bleeding
- Location of bleed - A trivial bleed in the brain can be fatal; the same volume in subcutaneous tissue is insignificant
- Health of the individual - Patients with underlying cardiac or lung disease decompensate at lower blood loss
Additional consequences:
- Large hemorrhages can cause jaundice as red cells are broken down by macrophages
- Chronic external blood loss (e.g., peptic ulcer, menstrual) leads to iron deficiency anemia (iron in hemoglobin is lost)
- Internal bleeding (hematoma) does NOT cause iron deficiency because iron is efficiently recycled from phagocytosed red cells
Summary Mnemonic: "HEMORR"
- Hematoma / Hemothorax / Hemopericardium
- Ecchymoses (1-2 cm bruises)
- Microvascular (capillary) bleeding in congestion
- Output compromised - hypovolemic shock if >20% lost
- Risk factors - diatheses, trauma, vasculitis
- Recycling - internal bleeds don't cause iron deficiency
Source: Robbins & Kumar Basic Pathology, Chapter 3 - Hemodynamic Disorders, Thromboembolism, and Shock
Explain thrombosis as essay for 10marks
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the complete 10-mark essay on Thrombosis, based on Robbins & Kumar Basic Pathology:
THROMBOSIS - Essay (10 Marks)
Introduction / Definition
Thrombosis is defined as the pathological formation of a solid mass (thrombus) from blood constituents within the vascular system in a living person. It is distinct from normal hemostasis (physiological clot after injury) - thrombosis occurs due to disease processes within intact or minimally damaged vessels. It underlies the most serious and common forms of cardiovascular disease, including myocardial infarction, stroke, and pulmonary embolism.
Pathogenesis - Virchow's Triad
The three primary abnormalities that lead to thrombosis are collectively called Virchow's Triad:
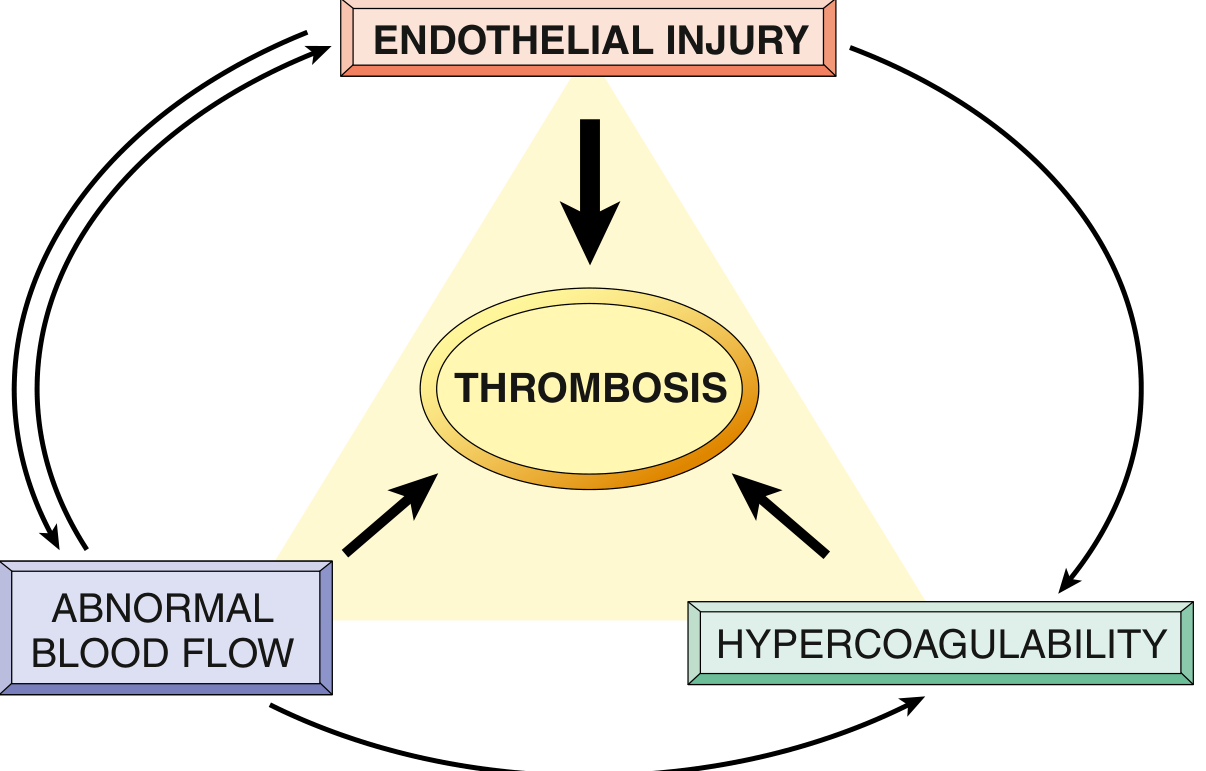
1. Endothelial Injury (Most Important Factor)
Endothelial injury is the dominant factor in thrombus formation in the heart and arteries, where high blood flow rates would otherwise prevent clot formation. Arterial and cardiac thrombi are therefore platelet-rich (white thrombi), as platelet adherence under high shear stress is a necessary prerequisite.
Mechanisms of prothrombotic endothelial changes:
- Procoagulant changes: Activated endothelium downregulates expression of coagulation inhibitors (thrombomodulin, endothelial protein C receptor, tissue factor pathway inhibitor) and increases expression of tissue factor, which activates the extrinsic coagulation cascade
- Antifibrinolytic effects: Secretion of plasminogen activator inhibitors (PAI) is increased, blocking t-PA and urokinase - limiting fibrinolysis
Causes of endothelial injury/dysfunction:
- Physical injury (trauma, surgery)
- Infectious agents (bacteria, viruses)
- Abnormal blood flow (turbulence)
- Inflammatory cytokines
- Metabolic abnormalities: hypercholesterolemia, homocystinemia
- Toxins from cigarette smoke
- Atherosclerosis (most common cause of arterial thrombosis)
2. Abnormal Blood Flow (Stasis and Turbulence)
Under normal laminar flow, platelets flow centrally in the vessel lumen, separated from the endothelium. Stasis and turbulence disrupt this by:
- Allowing platelets and clotting factors to contact the endothelium
- Preventing dilution of activated clotting factors by fresh blood flow
- Retarding inflow of clotting factor inhibitors
- Promoting endothelial cell activation and dysfunction
Turbulence contributes to arterial and cardiac thrombosis (e.g., at atherosclerotic plaques, vessel bifurcations, aneurysms).
Stasis is the major factor in venous thrombosis.
| Condition | Mechanism |
|---|---|
| Atherosclerotic plaques | Turbulence at irregular vessel surface |
| Aortic/arterial aneurysms | Local stasis in the sac |
| Acute myocardial infarction | Non-contractile myocardium → stasis |
| Atrial fibrillation | Atrial stasis → left atrial thrombus |
| Hyperviscosity syndromes | Sluggish flow → venous thrombosis |
| Varicose veins | Venous stasis → DVT |
| Prolonged immobility | Stasis in leg veins → DVT |
3. Hypercoagulability
Hypercoagulability is defined as any alteration of the coagulation pathways that predisposes to thrombosis. It is divided into:
Primary (Inherited) Hypercoagulable States:
- Factor V Leiden mutation - most common; mutated Factor V is resistant to inactivation by protein C
- Prothrombin gene mutation (G20210A) - elevated prothrombin levels
- Antithrombin III deficiency
- Protein C or Protein S deficiency - cannot inactivate Factors Va and VIIIa
- Homocystinemia - causes endothelial injury
Secondary (Acquired) Hypercoagulable States:
- High-risk: prolonged bed rest, MI, atrial fibrillation, cancer (Trousseau syndrome - migratory thrombophlebitis), prosthetic cardiac valves, DIC, heparin-induced thrombocytopenia (HIT)
- Lower-risk: oral contraceptive use, nephrotic syndrome, pregnancy, antiphospholipid antibody syndrome (lupus anticoagulant)
Morphology of Thrombi
A key gross feature of a true thrombus is that it is attached to the vessel wall at its point of origin and shows lines of Zahn - alternating pale (platelet-fibrin) and dark red (red cell-rich) layers, reflecting the sequential deposition during formation.
| Feature | Arterial Thrombus (White) | Venous Thrombus (Red) |
|---|---|---|
| Main trigger | Endothelial injury | Stasis |
| Composition | Platelet-rich, less fibrin | Red cell-rich, more fibrin |
| Location | Coronary, cerebral, femoral arteries | Deep leg veins (90%), pelvic veins |
| Effect | Occlusion → infarction | Occlusion + embolization |
| Direction of growth | Retrograde | Toward the heart (antegrade) |
Special types:
- Mural thrombi: Form in the heart chambers (over infarcted myocardium) or the aorta (over atherosclerotic plaques)
- Vegetations: Thrombi on heart valves - infective (infective endocarditis), sterile (non-bacterial thrombotic endocarditis, Libman-Sacks endocarditis in SLE)
Post-mortem clots are differentiated from true thrombi: they are gelatinous, with a red dependent layer and yellow "chicken-fat" upper layer, and are not attached to the vessel wall.
Fates of Thrombi
Once formed, a thrombus may undergo four possible outcomes:
-
Propagation - enlarges by accretion of more platelets and fibrin → increases risk of occlusion and embolization
-
Embolization - part or all of the thrombus detaches and travels through the circulation (most dangerous fate)
-
Dissolution - fibrinolytic system (plasmin) may dissolve new thrombi. Older thrombi with extensive fibrin polymerization are resistant to lysis - hence thrombolytic drugs (t-PA) must be given within a few hours of formation to be effective
-
Organization and Recanalization - ingrowth of endothelial cells, smooth muscle cells, and fibroblasts converts the thrombus into organized connective tissue. Capillary channels form within it (recanalization), partially restoring blood flow. Eventually incorporated into the vessel wall
Clinical Features and Consequences
The clinical significance of a thrombus depends primarily on where it forms:
Venous Thrombosis (Phlebothrombosis):
- Most common in deep veins of the leg (DVT) at or above the knee (popliteal, femoral, iliac veins)
- About 50% are asymptomatic - recognized only after pulmonary embolism
- Symptomatic DVT: unilateral leg pain, swelling, erythema, and warmth
- Greatest danger: pulmonary embolism (PE) - DVT is the source of >95% of PEs, which can cause sudden death
- Superficial venous thrombi (varicose veins) rarely embolize but cause local pain, congestion, and varicose ulcers
Arterial Thrombosis:
- Coronary artery → myocardial infarction
- Cerebral artery → ischemic stroke
- Mesenteric artery → intestinal infarction
- May also embolize (arterial embolism → ischemia of limbs, brain, kidneys)
Cardiac Thrombi:
- Mural thrombi over infarcted myocardium → systemic embolism
- Left atrial thrombus in AF → stroke
Summary
Thrombosis is a pathological process involving the interplay of endothelial injury, abnormal blood flow, and hypercoagulability (Virchow's Triad). Thrombi can be arterial (platelet-rich, cause occlusion/infarction) or venous (red cell-rich, cause embolism). The fate of a thrombus includes propagation, embolization, dissolution, or organization/recanalization. The major clinical consequences are myocardial infarction, stroke, and pulmonary embolism - making thrombosis one of the leading causes of death worldwide.
Source: Robbins & Kumar Basic Pathology, Chapter 3 - Hemodynamic Disorders, Thromboembolism, and Shock
This is a shared conversation. Sign in to Orris to start your own chat.