8. Amoebiasis / Entamoeba histolytica - Morphology, life cycle, pathogenesis, lab diagnosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, rich content from multiple authoritative sources. Let me compile the complete answer:
Amoebiasis / Entamoeba histolytica
Classification
Entamoeba histolytica is a protozoan parasite (Kingdom Protista, phylum Amoebozoa). It is the causative agent of amoebiasis - defined by WHO as "harbouring E. histolytica with or without clinical manifestations." Symptomatic disease occurs in less than 10% of infected individuals.
Important distinction: What was once called "E. histolytica" morphologically actually encompasses four species: pathogenic E. histolytica and non-pathogenic E. dispar, E. moshkovskii, and E. bangladeshi - all morphologically indistinguishable; differentiation requires molecular methods.
1. Morphology
E. histolytica exists in two stages:
A. Trophozoite (Vegetative form)
- Size: 12-50 µm (invasive forms typically >20 µm; non-pathogenic forms 15-20 µm)
- Motility: Actively motile by unidirectional pseudopodial movement - a hyaline pseudopod is extended, then the rest of the cell is drawn forward ("snail-like")
- Cytoplasm: Two zones:
- Ectoplasm (outer): Clear, hyaline
- Endoplasm (inner): Granular; may contain ingested red blood cells (pathognomonic - seen only in E. histolytica, never in E. coli or other commensals)
- Nucleus: Single; nuclear membrane lined by fine, regularly distributed chromatin granules (uniform peripheral chromatin); karyosome (endosome) is small and central
- Key feature: Erythrophagocytosis (RBCs in cytoplasm) is the only pathognomonic feature in stool specimens
B. Cyst (Infective form)
- Size: 10-20 µm
- Shape: Spherical, with a refractile wall
- Nuclei: 1 (uninucleate, immature) → 2 → 4 nuclei (mature, quadrinucleate - infective stage). Each nucleus has the same fine peripheral chromatin and central karyosome as the trophozoite
- Chromatoid bars: Cigar-shaped masses of ribonucleoprotein with smooth, rounded ends (this distinguishes from E. coli cysts, which have splintered/frayed chromatoid bars)
- Glycogen vacuole: Present in early cysts; disappears as maturation progresses
- Found only in lumen of colon and mushy/formed feces
Comparison: E. histolytica vs. E. coli
| Feature | E. histolytica | E. coli |
|---|---|---|
| Trophozoite size | 12-50 µm | 20-30 µm |
| Cyst size | 10-20 µm | 10-30 µm |
| Peripheral nuclear chromatin | Fine, evenly dispersed ring | Coarse, clumped |
| Karyosome | Central, sharp | Eccentric, coarse |
| Ingested RBCs | Present (pathognomonic) | Absent |
| Cyst nuclei | 1-4 | 1-8 |
| Chromatoid bars | Rounded ends | Splintered, frayed ends |
(Medical Microbiology 9e, Table 72.1)
Microscopy - trichrome stain (1000x):
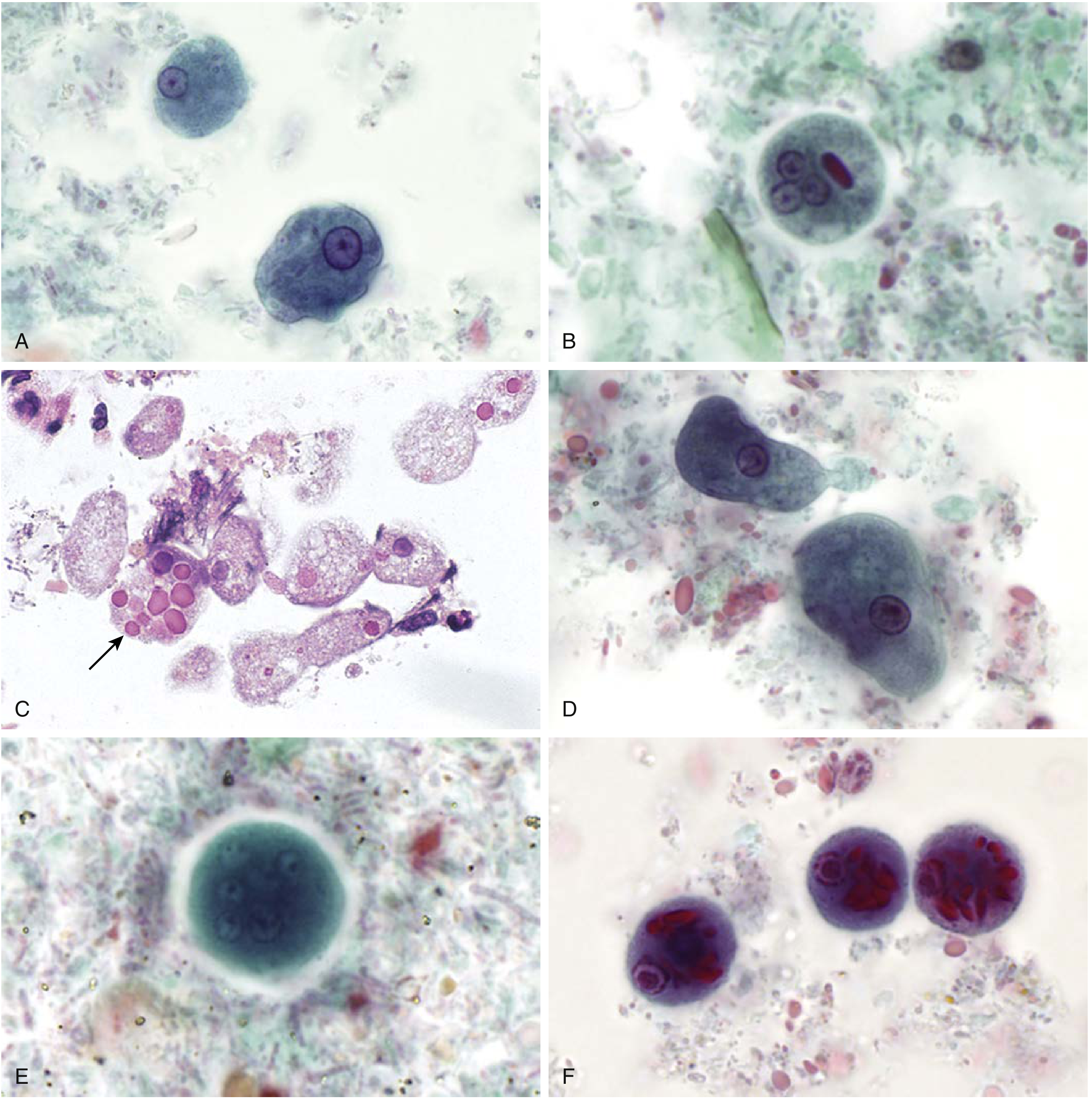
(Henry's Clinical Diagnosis, Fig. 65.10 - A: E. histolytica/dispar trophozoites; B: Cyst with 3 of 4 nuclei and rounded chromatoid bar; C: Trophozoites with ingested RBCs - arrow; D-E: E. coli forms; F: C. polecki cyst)
2. Life Cycle
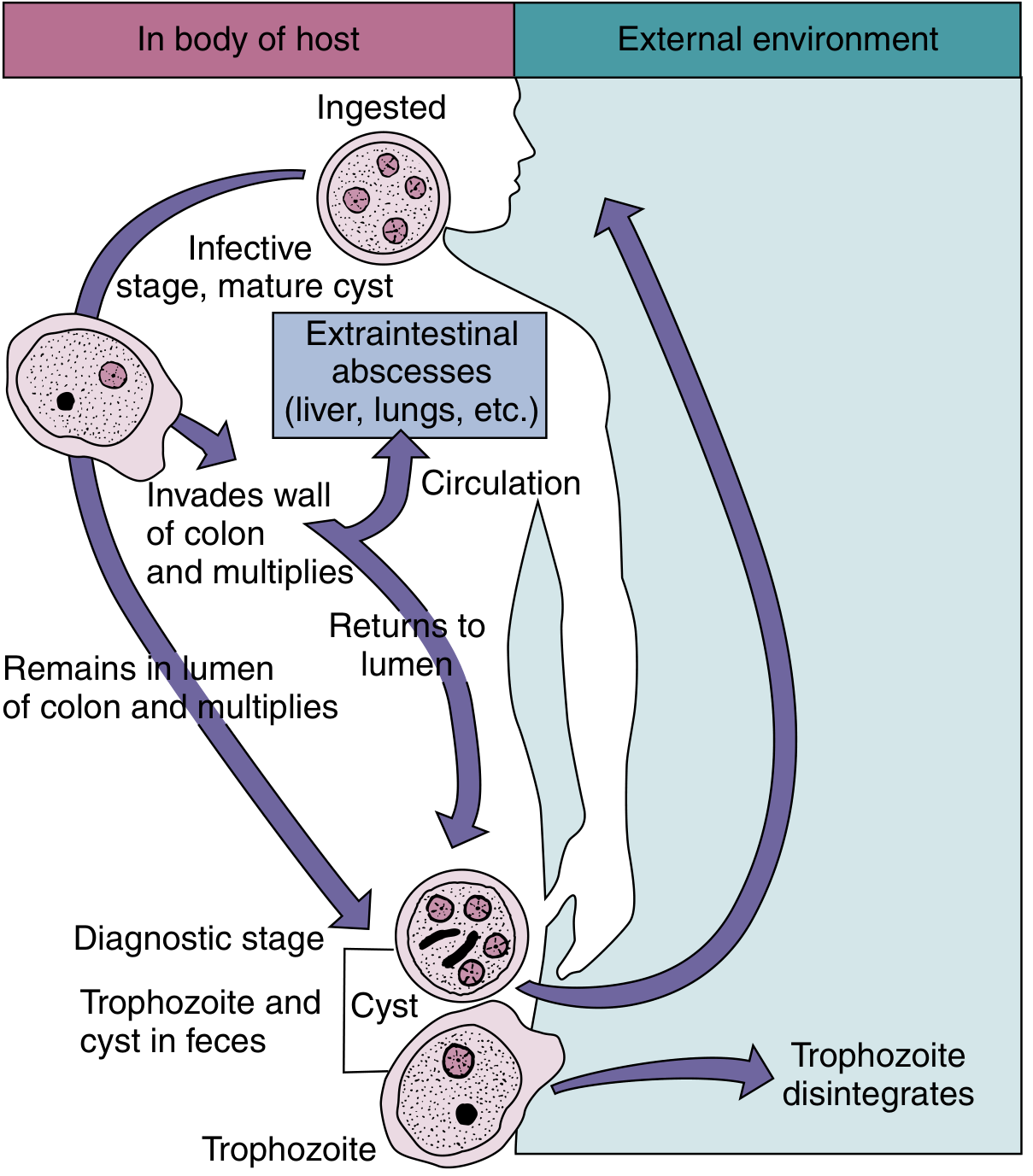
(Medical Microbiology 9e, Fig. 72.1 - Life cycle of E. histolytica)
The life cycle involves two stages: trophozoite and cyst. Humans are the only reservoir of infection.
Step-by-step:
-
Ingestion of mature quadrinucleate cysts - via contaminated food/water (fecal-oral route). Trophozoites cannot survive in the external environment or gastric acid, so cysts are the infective stage.
-
Excystation - Cysts pass through the stomach; exposure to gastric acid stimulates release of the pathogenic trophozoite in the duodenum. Each quadrinucleate cyst produces 8 trophozoites (4 nuclei → 8 cells by binary fission).
-
Colonization of large intestine - Trophozoites descend to the large intestine (primarily caecum and ascending colon, then rectosigmoid). They dwell in the colon, multiply by binary fission.
-
Two possible outcomes:
- Non-invasive: Trophozoites remain in the lumen → encyst → cysts passed in formed stool → environmental contamination → transmission
- Invasive: Trophozoites invade the bowel wall → ulceration → may enter portal circulation → liver (most common extraintestinal site), then lungs, brain, heart, skin
-
Encystment - When conditions become unfavorable (temperature drop, desiccation), trophozoites retract pseudopodia, become spherical, and encyst (uninucleate → quadrinucleate cyst)
-
Excretion - Cysts excreted in stool; carriers can shed up to 1.5 × 10⁷ cysts/day. Cysts survive in feces, water, and soil for several days at low temperature/moisture.
Cyst survival: Survive in moist conditions for days to weeks; resistant to chlorination at standard water treatment doses; killed by drying, heating to ~55°C, or freezing. Sand filtration and boiling are effective.
3. Pathogenesis
Mechanisms of tissue invasion
After excystation, invasive trophozoites use multiple mechanisms to destroy tissue:
-
Galactose-inhibitable adherence protein (lectin) - Trophozoites attach to colonic epithelial cells via a Gal/GalNAc-specific lectin on their surface. This attachment is required for cytolysis to occur.
-
Cytotoxin production - After attachment, trophozoites secrete toxins that cause lytic necrosis (not inflammatory necrosis initially). This causes a lethal alteration in host cell membrane permeability → irreversible rise in intracellular calcium → cell death.
-
Lysing of immune cells - Trophozoites lyse colonic epithelial cells, neutrophils, lymphocytes, and monocytes. Release of toxic neutrophil constituents after neutrophil lysis amplifies tissue destruction.
-
Anaerobic preference - Amebae are killed by ambient oxygen concentrations; they thrive in low-oxygen environments (colonic lumen, abscess cavities).
Pathological lesions
Intestinal (colonic) lesions:
- Initial lesion: Pinhead-sized ulcer with raised edges in the mucosa; mucus, necrotic cells, and amebae exude
- Trophozoites multiply above the muscularis mucosae, spreading laterally → undermine mucosa
- Classic "flask-shaped" (collar-button) ulcer: Narrow neck through mucosa leading to an expanded necrotic area in the submucosa - small point of entry, large necrotic base. This is the hallmark lesion of amoebiasis.
- Bacterial superinfection occurs in larger, established ulcers
- Coalescence of ulcers → large denuded mucosal areas
- Ameboma (amoebic granuloma): Granulomatous tumorlike mass on intestinal wall, can obstruct the lumen and mimic carcinoma - produces "napkin ring lesion"
- Perforation into peritoneal cavity is possible
Extraintestinal spread:
- Trophozoites penetrate the muscularis, enter mesenteric venules → portal blood → liver
- Amebic liver abscess (ALA): Most common extraintestinal form (~5% of intestinal cases). Predominantly right lobe, usually single. Aspirate is classically "anchovy sauce" / chocolate-colored pus (liquefied hepatic parenchyma). Trophozoites found at the margin of abscess, not in the center.
- Hematogenous/contiguous spread → lungs (rupture across diaphragm), brain, pericardium, skin (perianal ulcers)
Factors determining invasion:
- Number of amebae ingested
- Pathogenic capacity of the strain (zymodeme)
- Host immunity and gut motility
- Enteric bacteria (enhance amebic growth)
4. Laboratory Diagnosis
A. Microscopy (Stool Examination)
- Gold standard for intestinal amoebiasis
- Examine at least 3 stool specimens on separate days (parasites not homogeneously distributed)
- Fresh liquid/semi-liquid stools → look for motile trophozoites (survive only a few hours outside body; must be examined immediately)
- Formed stools → cysts (more stable)
Wet mount: Direct or concentration methods
- Trophozoites show rapid, progressive, unidirectional motility via hyaline pseudopodia; sharp ectoplasm-endoplasm demarcation
Permanent stained smear (Trichrome or iron-hematoxylin stain):
- Best method for detailed morphologic identification
- Shows nuclear detail: uniform peripheral chromatin + central karyosome
- Ingested RBCs in trophozoites = pathognomonic for invasive E. histolytica
Concentration techniques (formalin-ethyl acetate): For cyst detection
PAS stain on tissue sections: Trophozoites stain prominently
Note: E. histolytica is morphologically indistinguishable from E. dispar, E. moshkovskii, and E. bangladeshi - RBC ingestion is the only microscopic pathognomonic feature.
B. Culture
- Robinson's medium / Jones' medium / Boeck-Drbohlav medium
- Not widely used for diagnosis; mainly for research
- Useful for zymodeme analysis
C. Antigen Detection (EIA/ELISA)
- Enzyme immunoassay (EIA) on stool specimens
- Highly specific; can differentiate E. histolytica from E. dispar
- Commercially available (e.g., E. histolytica II ELISA, TechLab)
- Sensitivity ~85-90%, specificity ~99%
- Preferred over microscopy for species-level diagnosis
D. Serology (Antibody Detection)
- Detects host anti-amebic IgG antibodies
- Most useful for extraintestinal amoebiasis (ALA)
- ~95% of ALA patients are seropositive
- ~70% seropositive in active intestinal infection
- ~10% seropositive in asymptomatic carriers
- Tests: Indirect hemagglutination (IHA) - most sensitive; ELISA; counterimmunoelectrophoresis (CIE); indirect fluorescent antibody (IFA); latex agglutination
- Limitation: Titers persist months-to-years after treatment, so cannot distinguish current from past infection; less useful in endemic areas
E. Molecular Methods (PCR / DNA probes)
- Most sensitive and specific method
- Can definitively distinguish E. histolytica from E. dispar and other species
- FDA-approved multiplex panels: BioFire FilmArray GI Panel, BD MAX Enteric Parasite Panel, xTag GI Pathogen Panel
- Useful when serology/antigen tests are inconclusive
F. Aspiration of Liver Abscess
- Aspirate is chocolate-brown ("anchovy sauce") pus
- Trophozoites more likely in last aspirated material (at abscess wall margin)
- Direct microscopy or permanently stained slides
- PCR amplification of amebic 16S rRNA from aspirate is highly reliable
G. Imaging
- Ultrasound, CT scan, MRI of liver: Show abscess (usually single, right lobe)
- Cannot distinguish amebic from pyogenic abscess on imaging alone - requires serology
Summary Table: Lab Diagnosis
| Test | Best for | Notes |
|---|---|---|
| Stool microscopy (wet mount + trichrome) | Intestinal amoebiasis | 3 specimens; RBC phagocytosis = pathognomonic |
| Antigen EIA on stool | Intestinal amoebiasis | Differentiates E. histolytica vs E. dispar |
| Serology (IHA, ELISA) | ALA; extraintestinal disease | 95% positive in ALA; persists after cure |
| PCR / molecular | Species differentiation | Most specific; FDA-approved panels |
| Liver aspirate microscopy | ALA | Last aspirated material; margins of abscess |
| Culture | Research only | Zymodeme analysis |
Epidemiology (Quick Review)
- Worldwide distribution; highest in tropical/subtropical regions with poor sanitation
- Global: ~50 million infected; ~100,000 deaths/year
- India: ~15% prevalence (range 3.6-47.4%)
- Incubation period: 2-4 weeks (can be longer)
- Transmission: fecal-oral (contaminated water/food), oral-anal sexual contact, mechanical vectors (flies, cockroaches)
- Cysts resist standard chlorination; sand filtration and boiling are effective
Treatment (Brief)
- Invasive/systemic disease: Metronidazole or tinidazole (systemic penetration) → followed by luminal agent
- Luminal agents (to eradicate cysts/asymptomatic carriage): Diloxanide furoate, paromomycin, iodoquinol
- Treatment of asymptomatic carriers prevents environmental shedding
Sources: Medical Microbiology 9e (Murray); Henry's Clinical Diagnosis 23e; Park's Textbook of Preventive and Social Medicine; Jawetz Medical Microbiology 28e; Sleisenger & Fordtran's GI and Liver Disease; Robbins Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.