Teach me various changes in chest xray from basic to clinical with attached x ray and differentiating points in different conditions
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
chest X-ray systematic interpretation changes consolidation pneumothorax effusion cardiomegaly collapse with X-ray images
Loading Image
Loading Image
Loading Image
Reading Web Page
https://radiologyassistant.nl/chest/chest-x-ray/basic-interp…
Reading File
Finding Sources
Loading Image
Searching the Web
chest X-ray pneumonia consolidation air bronchogram lobar collapse cardiomegaly pulmonary edema images radiology
Loading Image
Loading Image
Searching the Web
chest xray cardiomegaly CTR measurement pulmonary edema interstitial pattern Kerley B lines images
Searching the Web
chest xray pneumothorax deep sulcus sign tension pneumothorax tracheal deviation images
Loading Image
Loading Image
Loading Image
I now have comprehensive material from Grainger & Allison's Diagnostic Radiology (the definitive radiology textbook), multiple real X-ray images, and supporting references. Let me compile the complete teaching guide.
Chest X-Ray: From Basic Interpretation to Clinical Findings
Source: Grainger & Allison's Diagnostic Radiology; Pfenninger & Fowler's Procedures for Primary Care; Tintinalli's Emergency Medicine; Radiology Masterclass; LearningRadiology.com
PART 1: BASICS - HOW TO READ A CXR SYSTEMATICALLY
Technical Assessment First (ALWAYS)
Before looking at pathology, verify:
| Parameter | Normal | Abnormal Clue |
|---|---|---|
| Patient identity & date | Labeled clearly | Missing = invalid film |
| Projection | PA (posteroanterior preferred) | AP films magnify heart |
| Rotation | Spinous process midway between clavicular heads | Rotation mimics mediastinal shift |
| Inspiration | 5-6 anterior ribs visible | <5 = poor inspiration, mimics cardiomegaly/basal disease |
| Exposure | Vertebral bodies visible through heart, but ribs clear | Under = too white; Over = too dark |
Systematic Approach: Inside-Out (ABCDE)
A - Airway (trachea midline, carina at T4-6, angle <70°)
B - Bones & soft tissues (ribs, clavicles, scapulae, soft tissue)
C - Cardiac silhouette (size, shape, borders)
D - Diaphragm (levels, costophrenic angles, subdiaphragmatic)
E - Everything else: lungs, hila, mediastinum, pleura
PART 2: KEY ANATOMICAL LANDMARKS ON A NORMAL CXR
Cardiac Borders (Silhouette Principle)
Structures touching each other produce a shared border. Loss of that border = pathology in the adjacent structure.
| Border | Structure Forming It |
|---|---|
| Right upper heart border | SVC / ascending aorta |
| Right lower heart border | Right atrium |
| Left upper border | Aortic knuckle |
| Left mid border | Pulmonary trunk / left atrial appendage |
| Left lower border | Left ventricle |
Cardiothoracic Ratio (CTR)
- Normal CTR < 0.5 on PA film (heart width < half thoracic width)
- CTR > 0.5 = cardiomegaly
- AP films falsely increase CTR (portable films are AP - note this caveat)
Diaphragm
- Right hemidiaphragm at level of 5th-6th anterior rib interspace
- Right is higher than left in >90% of people (by ~15 mm, up to 30 mm)
- Left has gas bubble underneath (stomach)
PART 3: THE FIVE CARDINAL OPACITIES (DENSITIES)
From whitest to blackest on CXR:
- Metal (clips, pacemakers) - densest white
- Bone (ribs, vertebrae)
- Fluid/soft tissue (heart, consolidation, effusion)
- Fat (slightly darker than soft tissue)
- Air (lung, trachea) - blackest
Key principle: Two structures of the SAME density touching each other = their border disappears (Silhouette Sign).
PART 4: MAJOR PATHOLOGICAL FINDINGS
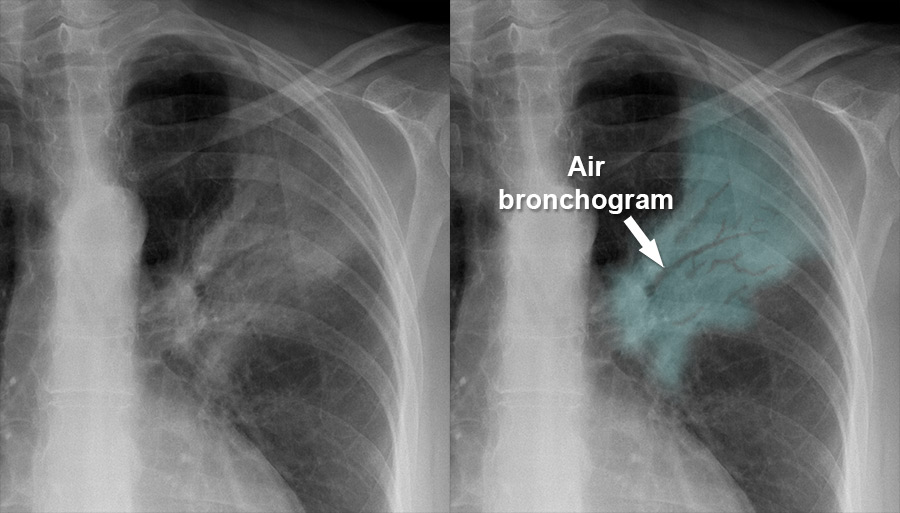
1. CONSOLIDATION (Air-Space Opacification)
Definition: Alveolar air replaced by fluid/pus/blood/cells, making the lung appear white/opaque.
X-ray features:
- Homogeneous or patchy opacity
- Air bronchogram - the hallmark: air-filled bronchi visible as dark branching lines against the white consolidated lung (only seen when the bronchi remain patent but surrounding alveoli are filled)
- Ill-defined borders (unless bounded by a fissure)
- No volume loss
- Lobar or segmental distribution
Air Bronchogram - Classic Example:
Causes of consolidation and differentiating features:
| Cause | Distinctive CXR Feature |
|---|---|
| Pneumonia (lobar) | Lobar/segmental distribution; air bronchogram; may cross segments; fever |
| Pulmonary edema | Bilateral perihilar "bat-wing" pattern; Kerley B lines; upper lobe venous diversion; cardiomegaly |
| Pulmonary infarction (PE) | Peripheral, wedge-shaped opacity (Hampton's hump); unilateral; near costophrenic angle |
| Pulmonary hemorrhage | Bilateral, diffuse; clears rapidly (24-48h); no fever |
| Alveolar cell carcinoma | Persistent consolidation not responding to antibiotics |
| Aspiration | Dependent zones (posterior lower lobes, right > left) |
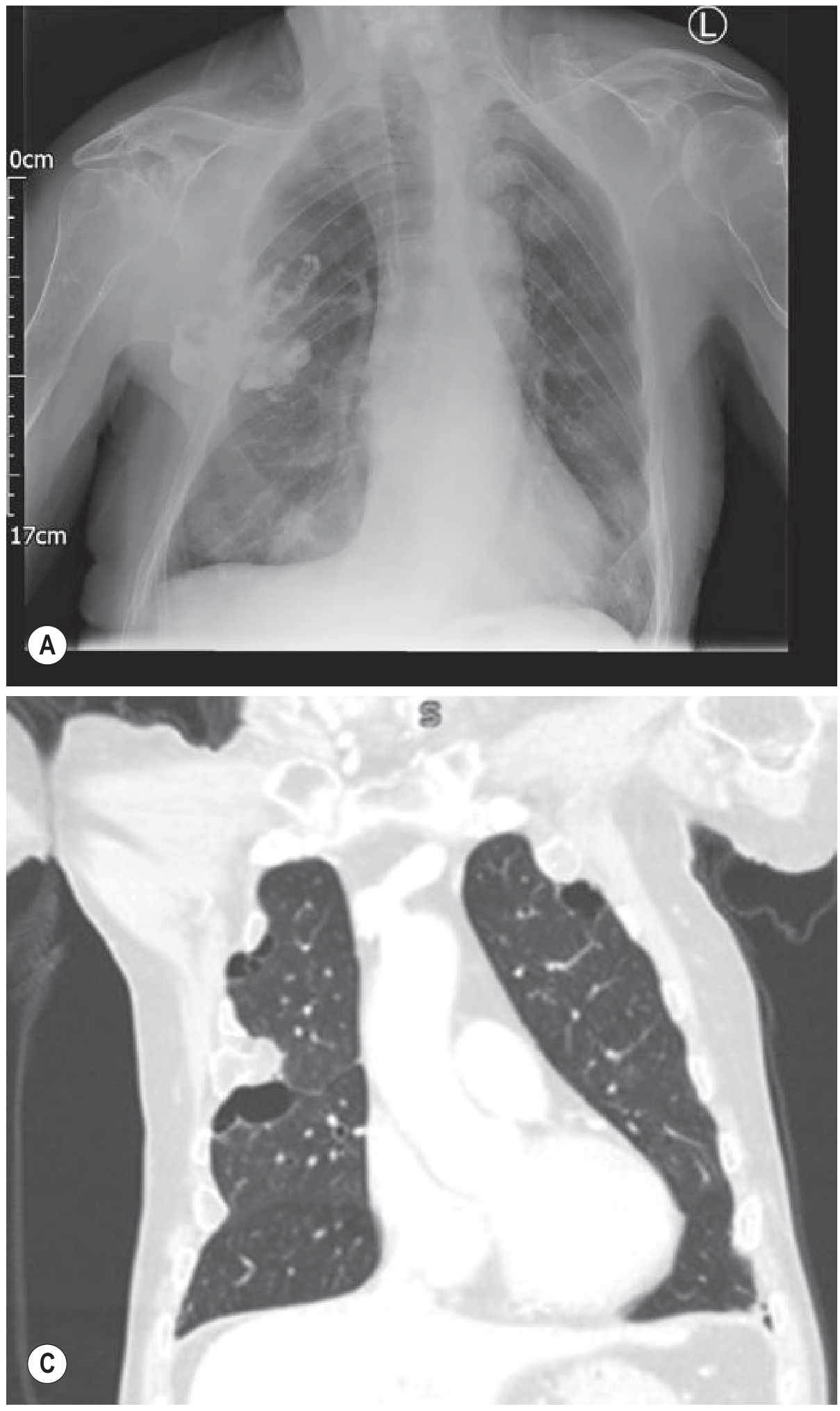
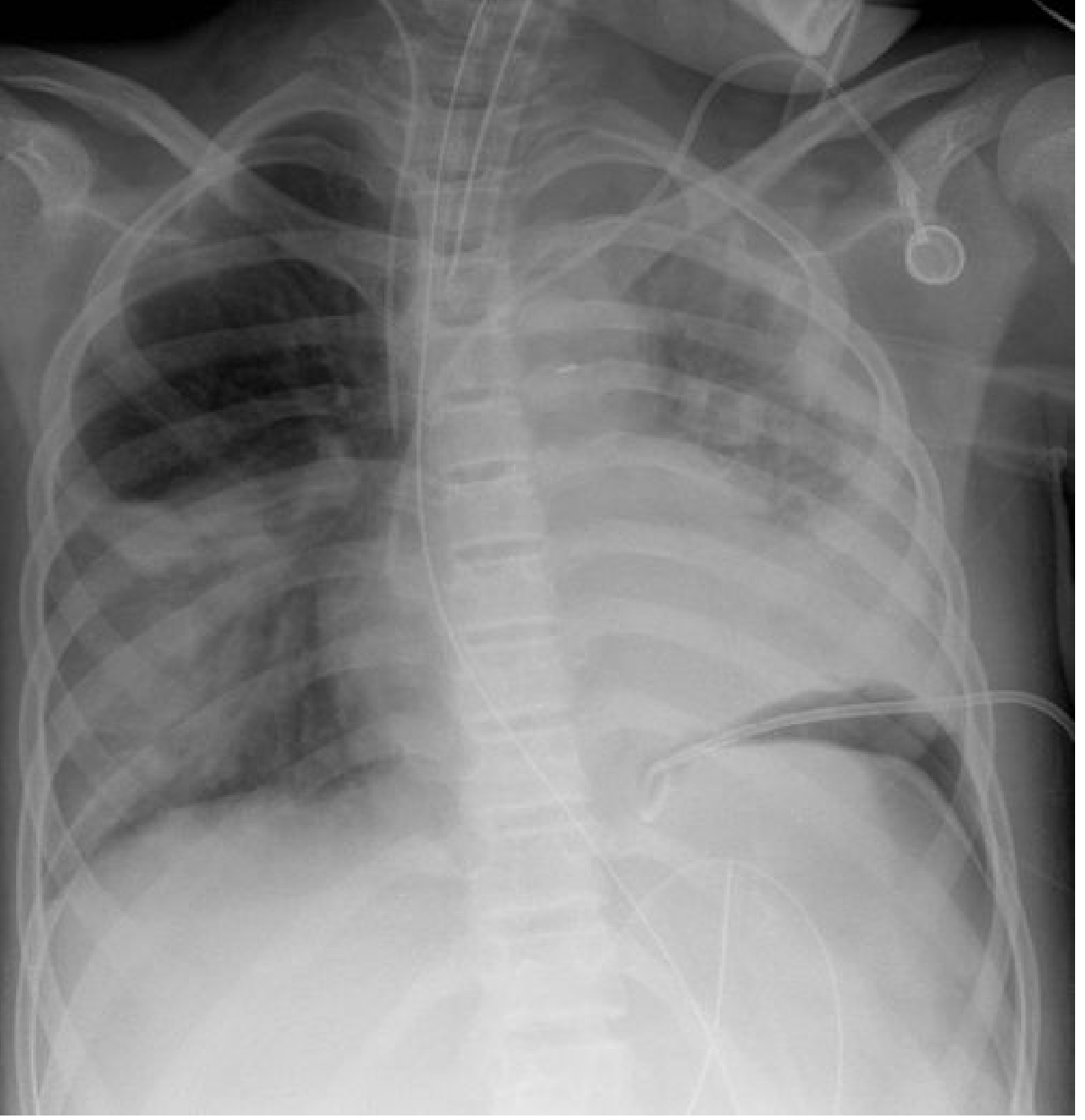
2. PLEURAL EFFUSION
Definition: Fluid accumulation in the pleural space.
X-ray features (erect PA view):
- Small effusion (<200 mL): Blunting of lateral costophrenic angle (>200-500 mL needed to blunt the posterior CP angle on PA)
- Moderate effusion: Homogeneous lower zone opacity with meniscus sign - concave upper border, higher laterally than medially
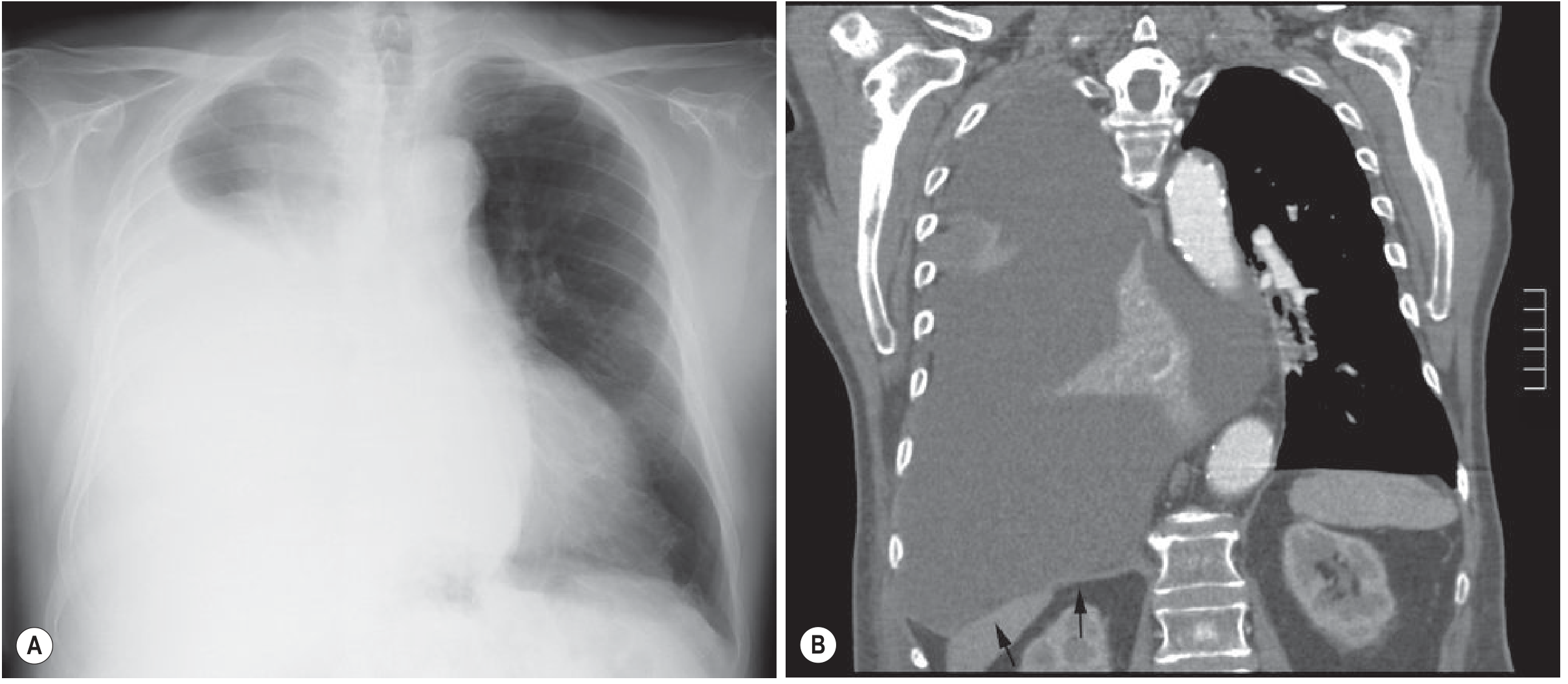
- Large/massive effusion: Dense hemithoracic opacification, mediastinal shift to opposite side
Classic Pleural Effusion - Meniscus Sign:
Massive Pleural Effusion With Mediastinal Shift:
Important differentiating clues:
| Finding | Effusion | Collapse | Consolidation |
|---|---|---|---|
| Mediastinal shift | Away from opacity | Towards opacity | None |
| Costophrenic angle | Blunted (meniscus) | May be blunted | Normal |
| Diaphragm | Elevated on side | Elevated | Normal |
| Air bronchogram | Absent | Absent (usually) | Present |
| Volume | Increased | Decreased | Normal/slight decrease |
Absence of mediastinal shift with massive effusion = suspect ipsilateral lobar collapse OR malignant pleural disease (e.g., mesothelioma, which tethers the mediastinum).
Empyema:
Supine effusion (ICU/portable films):
- No meniscus; fluid layers posteriorly
- "Veil-like" hazy opacity over the entire hemithorax
- Preserved vascular markings within the opacity
- No air bronchograms
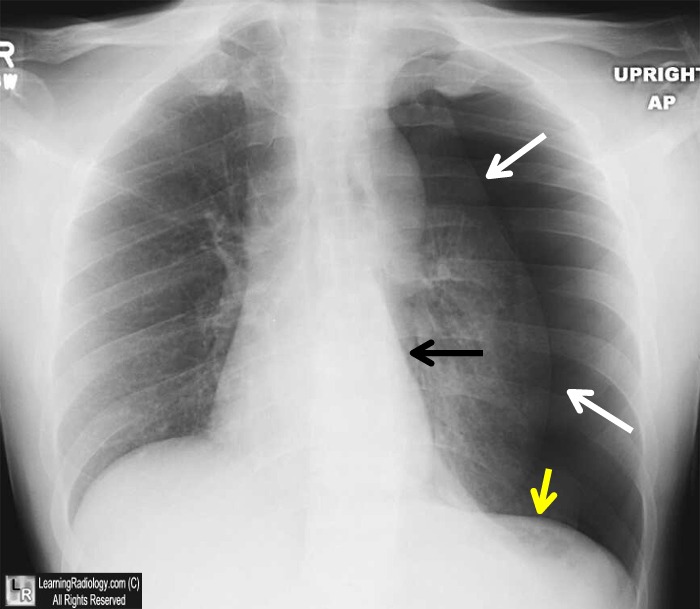
3. PNEUMOTHORAX
Definition: Air in the pleural space.
X-ray features (erect):
- Visceral pleural line - thin white line separated from chest wall
- Absent lung markings peripheral to that line
- Lung collapse varies from small apical to complete
Classic Left-Sided Pneumothorax:
Supine Pneumothorax - Deep Sulcus Sign:

Supine Pneumothorax (Bilateral Pneumonia Case):
Tension Pneumothorax (EMERGENCY):
- All above features PLUS:
- Mediastinal/tracheal deviation away from the side of pneumothorax
- Ipsilateral diaphragm depression / inversion
- Cardiovascular compromise - do NOT wait for X-ray to treat clinically!
Pneumothorax vs. Bulla/Skin fold - differentiating:
| Feature | Pneumothorax | Bulla | Skin Fold |
|---|---|---|---|
| Pleural line | Thin, convex towards chest wall | Concave | Wider margin, wrong orientation |
| Vascular markings | Absent beyond line | May be present | Present |
| Accentuated on expiration | Yes | No | No |
4. LOBAR COLLAPSE (ATELECTASIS)
Definition: Loss of air in a lobe or lung with volume reduction.
General CXR features of collapse:
- Increased opacity (white) of the affected area
- Volume loss: shift of fissures, trachea, hilum, mediastinum toward the collapse
- Elevated hemidiaphragm on affected side
- Crowding of ribs
- Compensatory hyperinflation of remaining lung
Lobe-by-lobe findings:
| Lobe | Key Sign on PA CXR | Other Features |
|---|---|---|
| Right upper lobe | Upward displacement of minor fissure; opacity in RUL | Tracheal deviation right; elevated right hilum |
| Right middle lobe | Loss of right heart border (silhouette sign); triangular density | Seen best on lateral view (narrow triangle) |
| Right lower lobe | Loss of right hemidiaphragm silhouette; opacity behind heart | Medial basal displacement; hilum depressed |
| Left upper lobe | "Veil-like" hazy opacity over entire left hemithorax | Loss of left heart border; "Luftsichel" sign (aortic knuckle visible) |
| Left lower lobe | Triangular opacity behind heart; loss of left diaphragm silhouette | Most common collapse in clinical practice |
Silhouette Sign (essential concept):
"When an intrathoracic lesion is in anatomical contact with a border of the heart, aorta, or diaphragm, the normal radiographic silhouette of these structures is obliterated."
- RML consolidation/collapse = loss of right heart border
- Lingula disease = loss of left heart border
- Right lower lobe = loss of right diaphragm silhouette
- Left lower lobe = loss of left diaphragm silhouette
5. CARDIOMEGALY & HEART FAILURE
Cardiomegaly: CTR > 0.5 on PA film
Causes: Dilated cardiomyopathy, valvular disease, pericardial effusion, hypertensive heart disease, congenital.
Radiological stages of heart failure (ABCDE mnemonic):
| Stage | Finding | Mechanism |
|---|---|---|
| A | Alveolar edema | Bat-wing/butterfly perihilar consolidations |
| B | Kerley B lines | 1-2 cm horizontal lines at lung bases (interlobular septal thickening) |
| C | Cardiomegaly | CTR >0.5 |
| D | Diversion of blood flow | Upper lobe vascular prominence/cephalization (vessels in upper zones ≥ same diameter as lower zone vessels) |
| E | Effusions | Bilateral (usually right > left) pleural effusions |
Interstitial edema (earlier stage):
- Kerley B lines (most specific)
- Kerley A lines: 5-10 cm lines from hila toward periphery
- Peribronchial cuffing: thickened bronchial walls seen end-on as "doughnuts"
- Perihilar haziness
Alveolar edema (advanced):
- Bilateral perihilar "bat-wing" consolidation with air bronchograms
- Fluffy, cloud-like bilateral opacities
- Rapid change between serial films (unlike pneumonia)
Differentiating cardiogenic vs. non-cardiogenic pulmonary edema (ARDS):
| Feature | Cardiogenic | ARDS |
|---|---|---|
| Cardiomegaly | Yes | No |
| Cephalization | Yes | No |
| Pleural effusions | Common, bilateral | Uncommon |
| Kerley B lines | Yes | No |
| Distribution | Perihilar, central | Peripheral/diffuse |
| Air bronchograms | In alveolar edema | Diffuse, prominent |
6. MEDIASTINAL ABNORMALITIES
Widened mediastinum (>8 cm at aortic arch level):
- Trauma: aortic dissection/rupture - superior mediastinal widening, loss of aortic knuckle, tracheal deviation right, apical cap (blood)
- Lymphadenopathy: bilateral hilar/paratracheal (sarcoidosis, lymphoma, TB)
- Masses by location:
| Compartment | Common Masses |
|---|---|
| Anterior (4 T's) | Thymoma, Teratoma, Terrible lymphoma, Thyroid |
| Middle | Lymphadenopathy, pericardial/bronchogenic cysts |
| Posterior | Neurogenic tumors, oesophageal pathology, vertebral disease |
Hilar enlargement:
- Bilateral symmetric = sarcoidosis (classic), lymphoma
- Bilateral asymmetric = lymphoma, metastases, TB
- Unilateral = lung cancer (hilar mass), pulmonary embolism (increased hilar opacity then pruning)
7. DIAPHRAGM ABNORMALITIES
Elevated hemidiaphragm (unilateral):
- Phrenic nerve palsy
- Subphrenic abscess
- Hepatomegaly (right)
- Lobar collapse (ipsilateral)
- Splinting from pleurisy/pneumonia
Bilateral elevated diaphragm:
- Poor inspiration (most common, technical)
- Obesity / pregnancy
- Ascites, abdominal distension
- Diffuse pulmonary fibrosis
- Bilateral basal PE
- Lymphangitis carcinomatosa
Flattened diaphragm:
- Emphysema (chronic hyperinflation)
- Severe acute asthma
Inverted diaphragm:
- Tension pneumothorax
- Large bullae
- Massive pleural effusion
8. INTERSTITIAL LUNG DISEASE (ILD) PATTERNS
Reticular pattern (net-like):
- IPF: bibasal, peripheral honeycombing
- Lymphangitis carcinomatosa: Kerley B lines, hilar adenopathy
Nodular pattern:
- Military TB/miliary metastases: 1-3 mm diffuse tiny nodules
- Sarcoidosis: upper/mid zone nodules + bilateral hilar adenopathy
Ground-glass opacity:
- Pneumocystis jirovecii pneumonia (PJP): bilateral perihilar ground-glass
- Early COVID-19: bilateral peripheral ground-glass
- Alveolar proteinosis: "crazy paving" on CT
Honeycombing (cystic changes with fibrosis):
- End-stage IPF; peripheral, bibasal
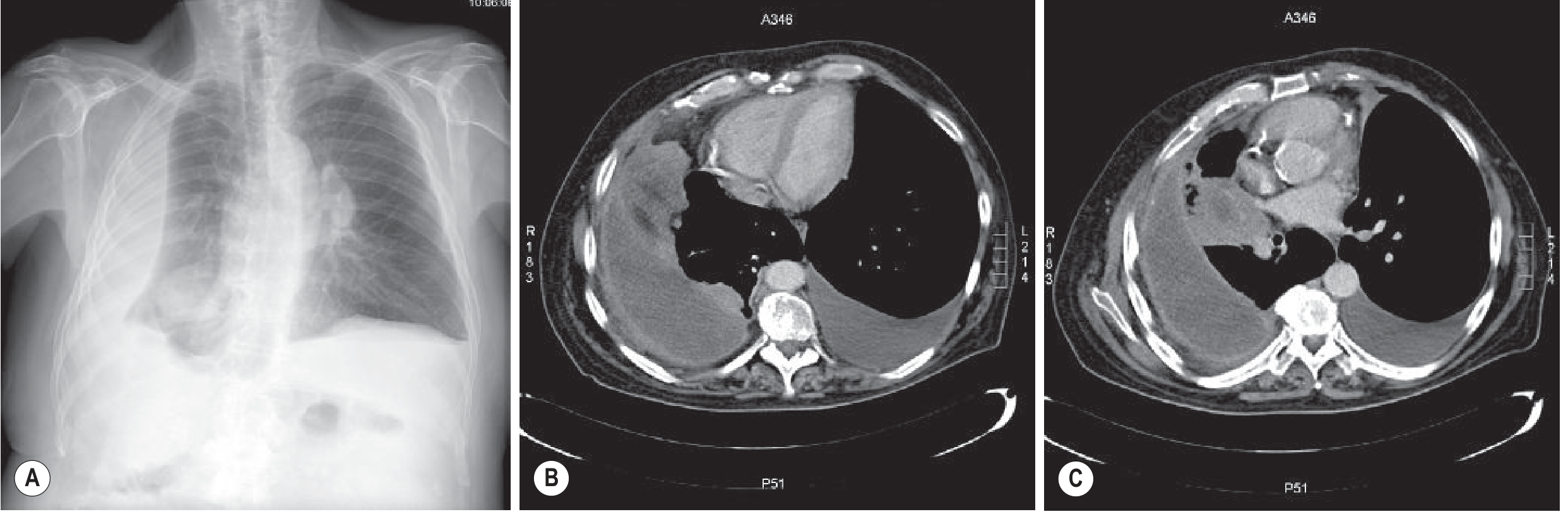
PART 5: DIFFERENTIATING THE "OPAQUE HEMITHORAX"
When one entire hemithorax is white, use these three clues to differentiate:
| Condition | Mediastinal Shift | Air Bronchograms | Volume |
|---|---|---|---|
| Massive effusion | Away (opposite side) | Absent | Increased |
| Complete collapse | Toward (same side) | Absent | Decreased |
| Consolidation (entire lung) | None | Present | Normal |
| Pneumonectomy | Toward (same side) | None | Decreased |
PART 6: QUICK CLINICAL CORRELATION TABLE
| Condition | Key CXR Finding | Clinical Scenario |
|---|---|---|
| Lobar pneumonia | Lobar consolidation + air bronchogram + preserved volume | Fever, productive cough, pleuritic pain |
| Pulmonary edema | Bat-wing + Kerley B + cardiomegaly + cephalization | Acute dyspnea, orthopnea, S3 gallop |
| Pleural effusion | Blunted CP angle + meniscus | Dyspnea, dull percussion |
| Tension pneumothorax | Tracheal deviation + absent markings + mediastinal shift | Acute severe dyspnea + hypotension |
| Lobar collapse | Volume loss + opacity + shift toward + loss of border | Post-op, obstructing lesion, mucus plug |
| Aortic dissection | Widened mediastinum + loss of aortic knuckle | Tearing chest/back pain, hypertension |
| TB (primary) | Upper lobe consolidation + ipsilateral hilar adenopathy + pleural effusion | Night sweats, weight loss, hemoptysis |
| Sarcoidosis | Bilateral hilar lymphadenopathy ("potato nodes") | Incidental or with erythema nodosum |
| Malignancy | Perihilar mass + post-obstructive collapse | Smoker, hemoptysis, weight loss |
| ARDS | Diffuse bilateral consolidation, no cardiomegaly | ICU, sepsis, trauma, pancreatitis |
PART 7: IMPORTANT RADIOLOGICAL SIGNS TO MEMORIZE
| Sign | Meaning | Condition |
|---|---|---|
| Air bronchogram | Patent bronchi in opacified lung | Consolidation (pneumonia, edema) |
| Silhouette sign | Loss of border between adjacent same-density structures | Localizes disease to lobe/segment |
| Meniscus sign | Concave upper border of fluid, higher laterally | Free pleural effusion |
| Deep sulcus sign | Abnormally deep, sharp costophrenic angle | Pneumothorax on supine film |
| Kerley B lines | Short horizontal basal lines | Interstitial edema (heart failure) |
| Hampton's hump | Peripheral wedge-shaped opacity | Pulmonary infarct from PE |
| Westermark sign | Focal oligemia distal to PE | Pulmonary embolism |
| Luftsichel sign | Crescent of air around aortic knuckle | Left upper lobe collapse |
| Golden S sign | S-shaped fissure in RUL collapse | Central obstructing mass |
| Spine sign | Lower vertebrae appear denser on lateral | Lower lobe consolidation/mass |
| CT angiogram sign | Pulmonary vessels visible through dense consolidation | Bronchioloalveolar carcinoma |
Summary: The 3-Step Approach at the Bedside
- Is it opaque or lucent?
- Opaque = consolidation, collapse, effusion, mass
- Lucent = pneumothorax, emphysema, cyst/bulla
- What is the volume?
- Increased = effusion, mass
- Decreased = collapse, fibrosis
- Normal = consolidation, infarction
- Where is the mediastinum?
- Away from opacity = effusion
- Toward opacity = collapse
- Central = consolidation
This three-step framework lets you rapidly classify almost any CXR finding before thinking about specific diagnoses.
Primary references: Grainger & Allison's Diagnostic Radiology (9780323760751); Pfenninger & Fowler's Procedures for Primary Care (9780323052672); Tintinalli's Emergency Medicine (9781260019933); RadiologyMasterclass.co.uk; LearningRadiology.com
This is a shared conversation. Sign in to Orris to start your own chat.