Eras protocol for major abdominal surgeries with use of opioid vs non opioid analgesics
Reading File
Finding Sources
Finding Sources
Searching PubMed
"enhanced recovery after surgery" AND "opioid sparing" AND "abdominal surgery"
Reading File
Reading File
Reading File
Searching PubMed
"ERAS" AND "multimodal analgesia" AND "abdominal surgery"
Reading File
Finding Sources
Searching PubMed
"ERAS" AND "non-opioid analgesia" AND "colorectal surgery"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
"opioid free anesthesia" AND "abdominal surgery" AND outcomes
Reading File
Reading File
Reading Article
Loading Image
Reading File
I now have all the essential material to write a comprehensive, well-structured answer. Let me compile it.
ERAS Protocol for Major Abdominal Surgery: Opioid vs. Non-Opioid Analgesia
What is ERAS?
Enhanced Recovery After Surgery (ERAS) is an evidence-based, multidisciplinary perioperative care program designed to accelerate recovery, reduce complications, and shorten hospital stay after major surgery. First developed by Henrik Kehlet for colorectal resections in the 1990s and formalized by the ERAS Society in 2005, ERAS addresses the systemic inflammatory and catabolic stress response through bundled care protocols spanning the preoperative, intraoperative, and postoperative phases.
In major abdominal surgery, ERAS consistently reduces postoperative non-operative morbidity by 40-50% and shortens length of stay by 2-3 days compared to traditional care. - Miller's Anesthesia, 10e
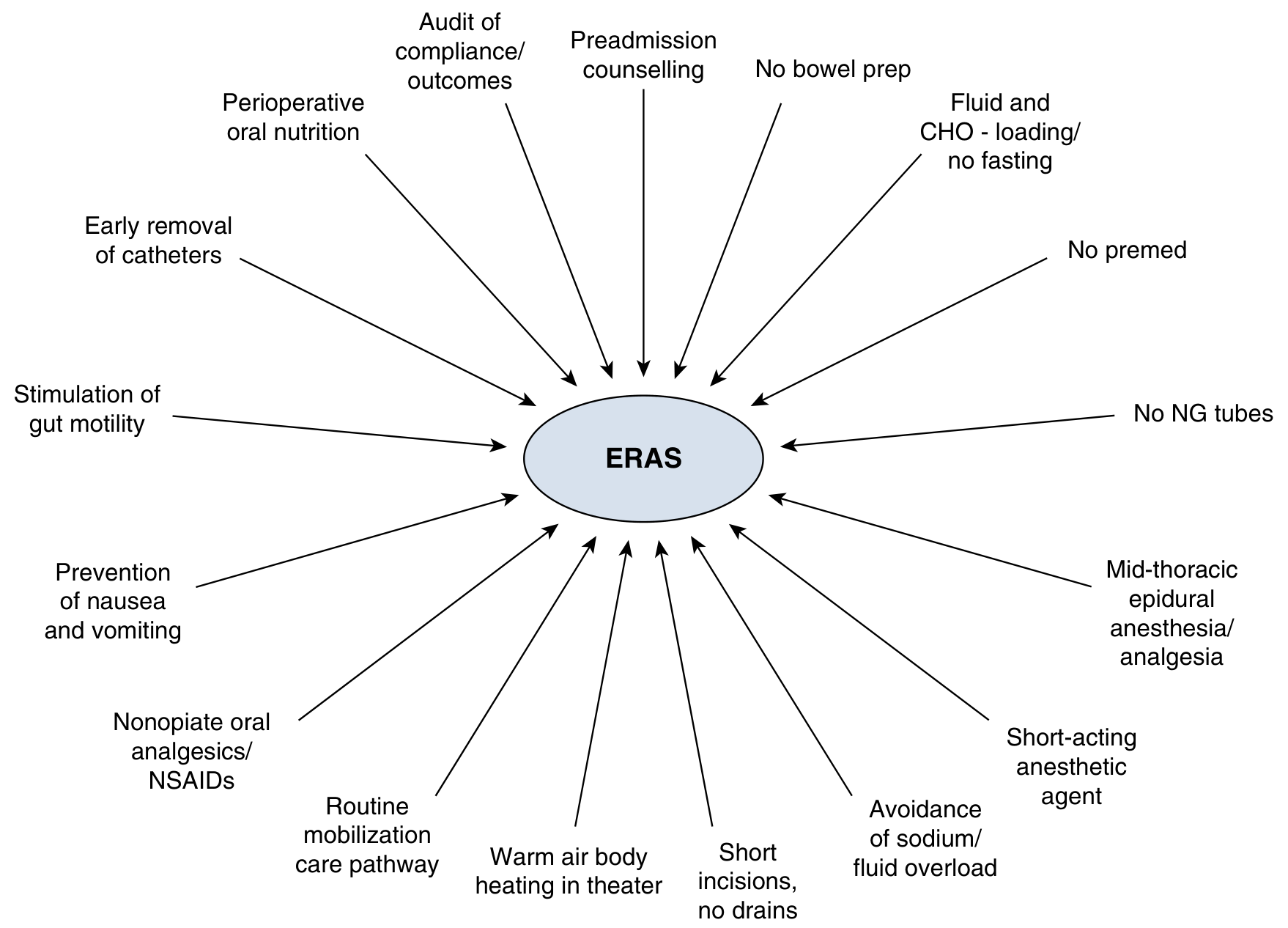
Full ERAS Pathway for Major Abdominal Surgery
PREOPERATIVE PHASE
| Element | Recommendation |
|---|---|
| Preadmission counselling | Patient education on expectations, pain management, early mobilisation |
| Bowel preparation | Selective use only (avoid routine mechanical prep); if used, add oral antibiotics (neomycin + metronidazole) |
| Fasting | Solids allowed up to 6 h; clear fluids up to 2 h before surgery |
| Carbohydrate loading | Maltodextrin drink 2 h pre-surgery - shifts body to anabolic/fed state, reduces postoperative insulin resistance by ~50% |
| Pre-emptive analgesia | Acetaminophen 1000 mg PO + Celecoxib 200-400 mg PO (or ibuprofen 400 mg) |
| VTE prophylaxis | Heparin 5000 U SC or enoxaparin + pneumatic compression devices |
| Antibiotics | Cefazolin 2 g IV within 1 hour of incision (+ metronidazole if bowel resection) |
| Neuraxial placement | Thoracic epidural catheter placed before induction for open major surgery |
| No premedication | Avoid routine benzodiazepine premedication (causes delirium, delayed recovery) |
(Sabiston Textbook of Surgery, 21e; Current Surgical Therapy, 14e)
INTRAOPERATIVE PHASE
| Element | Recommendation |
|---|---|
| Anesthetic agents | Short-acting agents preferred (sevoflurane/desflurane, propofol TIVA) |
| Fluid management | Goal-directed: balanced crystalloids, vasopressors for hypotension, target near-zero fluid balance (<2 kg weight gain) |
| Normothermia | Forced-air warming, warmed IV/irrigation fluids, ambient temperature ≥21°C |
| NG tubes | Avoid routine nasogastric decompression |
| Incisions | Minimize length; avoid unnecessary drains |
| Pain strategy | Opioid-sparing multimodal analgesia (see below) |
| PONV prophylaxis | Dexamethasone 8-10 mg IV + ondansetron 4 mg IV ± droperidol |
POSTOPERATIVE PHASE
| Element | Recommendation |
|---|---|
| Feeding | Early oral intake same day or POD 1 |
| Fluids | Transition to oral fluids promptly; avoid prolonged IV fluids |
| Catheter/drains | Remove urinary catheter POD 1-2; early drain removal |
| Mobilisation | Out of bed same day (within 4-6 hours of surgery) |
| Gut motility | Alvimopan, laxatives, early enteral nutrition to prevent ileus |
| Analgesia | Continue multimodal oral/IV regimen (see below) |
Analgesia in ERAS: The Central Role
"ERAS protocols focus on opioids as a single component of a comprehensive pain relief strategy, not as the mainstay for treatment. Instead, multimodal analgesia should be emphasized." - Schwartz's Principles of Surgery, 11e
The goal is opioid-sparing multimodal analgesia - using several analgesic classes with complementary mechanisms to achieve adequate pain control while minimizing opioid-related adverse effects (PONV, respiratory depression, ileus, urinary retention, immune suppression, opioid-induced hyperalgesia).
NON-OPIOID ANALGESICS IN ERAS
1. Acetaminophen (Paracetamol)
- Indication: ALL patients without contraindication
- Preoperative: 975-1000 mg IV or PO
- Postoperative: Regular scheduled dosing, max 4 g/24 h
- Mechanism: Central COX inhibition, endocannabinoid modulation
- Advantage: No effect on platelet function, no renal risk, no GI bleeding
- Contraindication: Acute decompensated liver failure
2. NSAIDs / COX-2 Inhibitors
- Indication: ALL patients without contraindication
- Agents: Celecoxib 200-400 mg PO, ibuprofen 400 mg, ketorolac 15-30 mg IV
- Mechanism: Peripheral COX-1/COX-2 inhibition, reduces prostaglandin-mediated sensitization
- Advantage: Anti-inflammatory, synergistic with opioids (reduces opioid requirements by 30-40%)
- Contraindications: Pre-existing renal insufficiency, hypovolemia, major blood loss, hypotension, bleeding/coagulation disorders, GI bleeding history, NSAID hypersensitivity
3. Epidural Analgesia (Gold standard for open abdominal surgery)
- Indication: Major open thoracic and abdominal surgery
- Technique: Mid-thoracic catheter (T6-T9 level), local anesthetic (bupivacaine) ± low-dose opioid
- Advantages:
- Profound somatic and visceral analgesia
- Reduces systemic opioid requirements
- Attenuates surgical stress response
- Favorable cardiorespiratory effects (reduces pulmonary complications, improves bowel recovery)
- Epidural local anesthetics independently accelerate return of GI function
- Concerns: Postural hypotension (delays mobilisation), VTE prophylaxis timing conflicts, urinary retention
- Note: Role is decreasing in laparoscopic ERAS due to availability of equivalent alternatives (TAP blocks)
4. IV Lidocaine Infusion
- Indication: Major open abdominal surgery when regional analgesia is not possible
- Dosing: 1.5 mg/kg IBW bolus, then 2 mg/kg/h infusion (can continue postoperatively on monitored floor)
- Mechanism: Sodium channel blockade, anti-inflammatory properties
- Advantages: Opioid-sparing, reduces PONV, hastens return of bowel function (particularly valuable in colorectal ERAS), possible anti-cancer effect
- Contraindications: Cardiac arrhythmias, seizure disorder, electrolyte imbalance, pregnancy; do NOT combine with regional LA blocks (risk of toxicity)
5. Ketamine
- Indication: Opioid-tolerant patients or major painful surgery when non-opioid approaches are insufficient
- Dosing: 0.25 mg/kg IBW bolus + 0.1 mg/kg/h infusion (no role for single bolus doses alone)
- Mechanism: NMDA receptor antagonist
- Advantages:
- Opioid-sparing
- May prevent opioid-induced hyperalgesia
- May prevent chronic post-surgical pain syndromes
- Contraindications: Psychiatric disturbance, cardiovascular or hepatic disease, pregnancy
- Note: Dysphoria and hallucinations at higher doses; subanesthetic doses (0.1-0.35 mg/kg) are well-tolerated
6. Gabapentinoids (Gabapentin / Pregabalin)
- Indication: Preoperative dose for opioid-sparing, especially in opioid-tolerant patients
- Dosing: Gabapentin 300 mg PO (<65 years); 100-300 mg PO (>65 years); adjust for renal function
- Mechanism: Alpha-2-delta calcium channel subunit blockade - reduces central sensitization
- Advantages: Opioid-sparing, reduces postoperative pain, reduces opioid side effects
- Concerns: Visual disturbances, sedation, dizziness; dose reduce in renal impairment; recent debate on routine use due to sedation risk
7. Dexamethasone
- Indication: All patients without contraindication
- Dosing: 8-10 mg IV single intraoperative dose
- Primary role: PONV prophylaxis
- Secondary role: Anti-inflammatory analgesic adjunct
- Contraindications: Poorly controlled diabetes (HbA1c >10%) - transient hyperglycemia
8. Regional/Fascial Plane Blocks
| Block | Indication | Notes |
|---|---|---|
| TAP (Transversus Abdominis Plane) block | Open and laparoscopic lower abdominal surgery | 4-quadrant TAP using bupivacaine 0.25% + epinephrine; excellent alternative to epidural for laparoscopic surgery |
| Erector Spinae Plane (ESP) block | Upper and lower abdominal surgery | Covers broader dermatomal range |
| Paravertebral block | Open thoracic, hepatobiliary surgery | Equivalent to epidural with fewer hemodynamic effects |
| Surgical site infiltration | All surgeries | Must infiltrate all layers (peritoneal, musculofascial, subdermal); liposomal bupivacaine 266 mg (diluted to 180 mL saline) prolongs duration |
9. Magnesium
- Dosing: Bolus 1-3 g IV, infusion 0.5-1 g/h
- Mechanism: NMDA antagonism (similar to ketamine but weaker), calcium channel effects
- Advantage: Opioid-sparing
- Contraindications: Renal insufficiency, neuromuscular disorders, bradyarrhythmias, hypotension
10. Dexmedetomidine
- Dosing: Bolus 0.5-0.6 mcg/kg; infusion 0.3-1 mcg/kg/h
- Advantage: Opioid-sparing, useful as perineural adjunct for nerve blocks
- Caution: No independent role in pain management in ERAS; concerns of prolonged hypotension and sedation delaying mobilisation
OPIOIDS IN ERAS: Appropriate Use
Despite the opioid-sparing framework, opioids remain part of ERAS - as a rescue or adjunct, not the foundation.
| Agent | Route | ERAS Role |
|---|---|---|
| Morphine / Hydromorphone | PCA | Rescue; patient-controlled; titrate to effect |
| Fentanyl | IV intraoperative | Minimized or omitted; exposure in OR worsens postoperative pain scores |
| Intrathecal morphine | Single-shot spinal | Excellent for laparoscopic colorectal/major abdominal; provides 12-24 h analgesia |
| Epidural opioid (low dose) | Combined with LA | Part of thoracic epidural infusion |
| Oral oxycodone/tramadol | PO postoperative | Short course rescue; minimize duration |
Disadvantages of opioids that ERAS specifically targets:
- Worsen pain scores after they wear off (hyperalgesia)
- Increase postoperative opioid requirements
- PONV (nausea/vomiting)
- Respiratory depression
- Reduced GI motility - major driver of ileus and delayed discharge in abdominal surgery
- Urinary retention
- Endocrine dysfunction (ADH release, immune suppression)
- Cancer growth (immunomodulation)
(Schwartz's Principles of Surgery, 11e)
Opioid-Free vs. Opioid-Sparing: What Does the Evidence Show?
A 2024 systematic review and meta-analysis (26 RCTs, 2,025 patients) comparing opioid-free vs. opioid anesthesia in minimally invasive abdominal surgery found:
- PONV significantly reduced with opioid-free anesthesia (RR 0.55, 95% CI 0.40-0.74; p<0.001)
- Opioid consumption at 2 hours post-surgery was significantly lower (MD -5.4 mg oral morphine equivalents)
- Pain scores were marginally higher in the opioid-free group but not clinically meaningful
- No difference in PACU length of stay
- Conclusion: Opioid-free anesthesia is a valid alternative for minimally invasive abdominal surgery, especially in patients at high PONV risk - [da Silveira et al., Can J Anaesth 2024, PMID 39500840]
A 2024 RCT compared opioid-free vs. opioid-sparing strategies for laparoscopic colectomy and found comparable outcomes, with the opioid-free group achieving equivalent analgesia using a combination of regional anesthesia, ketamine, lidocaine, and NSAIDs. - [PMID 39393528]
Practical ERAS Analgesic Protocol Summary
Preoperative (1-2 hours before surgery)
- Acetaminophen 1000 mg PO
- Celecoxib 200-400 mg PO (or ibuprofen 400 mg)
- Gabapentin 100-300 mg PO (especially opioid-tolerant patients)
- Place thoracic epidural catheter (for open surgery)
Intraoperative
- Epidural infusion (bupivacaine ± low-dose opioid) OR TAP/ESP blocks
- IV Lidocaine infusion 1.5 mg/kg bolus → 2 mg/kg/h (open abdominal surgery without epidural)
- IV Ketamine 0.1-0.35 mg/kg ± infusion (opioid-tolerant patients)
- Dexamethasone 8-10 mg IV (PONV + analgesic adjunct)
- Magnesium 1-2 g IV
- Minimize/avoid intraoperative fentanyl; if used, low dose only
- Surgical wound infiltration with bupivacaine or liposomal bupivacaine at closure
Postoperative
- Scheduled acetaminophen 1000 mg IV/PO q6h (max 4 g/day)
- Scheduled NSAID (celecoxib 200 mg PO q12h or ketorolac 15-30 mg IV q6h, short course)
- Continue epidural infusion OR IV lidocaine for 24-48 h (open surgery)
- PRN opioid rescue (low-dose oral oxycodone or morphine PCA) only for breakthrough pain
- Early oral analgesic transition (step down from IV to PO as soon as tolerating diet)
Key Principles Summarized
- Multimodal is mandatory - no single agent provides complete analgesia without excessive dose-dependent side effects
- Epidural remains gold standard for open major abdominal surgery (colorectal, hepatobiliary, esophageal) but is being replaced by fascial plane blocks in laparoscopic settings
- IV lidocaine infusion is the preferred systemic non-opioid for open abdominal surgery without epidural - especially valuable for its pro-motility effects
- Acetaminophen + NSAID scheduled around the clock for all patients forms the analgesic base
- Ketamine is reserved for opioid-tolerant patients or for prevention of chronic pain
- Opioids are rescue agents, not scheduled first-line, and should be discontinued as early as possible
- Regional blocks (TAP, ESP) are the preferred opioid-sparing strategy in laparoscopic surgery
- Pain management goal in ERAS is to facilitate early mobilization, not simply to achieve a numerical pain score target
Sources: Sabiston Textbook of Surgery 21e; Schwartz's Principles of Surgery 11e; Miller's Anesthesia 10e; Current Surgical Therapy 14e; Barash Clinical Anesthesia 9e; da Silveira et al., Can J Anaesth 2024 [PMID 39500840]; Collange et al., Anaesth Crit Care Pain Med 2024 [PMID 39393528]
This is a shared conversation. Sign in to Orris to start your own chat.