Explain vasculitis
Reading File
Finding Sources
Searching PubMed
vasculitis classification pathogenesis
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich content from multiple authoritative sources. Let me compile the comprehensive answer.
Vasculitis
Vasculitis is a clinicopathologically defined process characterized by inflammation and necrosis of blood vessel walls, leading to narrowing or occlusion of the lumen, aneurysm formation, and impairment of distal organ function. The vasculitides are a heterogeneous group of rare disorders; collectively they span conditions affecting every organ system and every caliber of vessel.
- Andrews' Diseases of the Skin, p. 961
- Rheumatology 2-Volume Set (Elsevier, 2022), p. 2093
Classification - Vessel Size is the Primary Organizer
The 2012 Revised International Chapel Hill Consensus Conference (CHCC) is the most widely used nomenclature system. Vessels are divided into three main size categories:
| Vessel Size | Vessels Involved | Main Diseases |
|---|---|---|
| Large | Aorta and main branches | Takayasu arteritis, Giant cell arteritis (GCA) |
| Medium | Main visceral arteries (renal, mesenteric, coronary) | Polyarteritis nodosa (PAN), Kawasaki disease |
| Small | Arterioles, capillaries, venules | ANCA-associated (GPA, MPA, EGPA), Immune complex (IgA vasculitis/HSP, cryoglobulinemic, urticarial vasculitis) |
| Variable | Any vessel | Behçet disease, Cogan syndrome |
Small-vessel vasculitis is further subdivided by mechanism:
-
ANCA-associated (pauci-immune): Granulomatosis with polyangiitis (GPA, formerly Wegener's), Microscopic polyangiitis (MPA), Eosinophilic granulomatosis with polyangiitis (EGPA, formerly Churg-Strauss)
-
Immune complex-mediated: IgA vasculitis (Henoch-Schönlein purpura), cryoglobulinemic vasculitis, hypocomplementemic urticarial vasculitis
-
Washington Manual of Medical Therapeutics, p. 968
-
Firestein & Kelley's Textbook of Rheumatology, p. 1945
Pathogenesis
Two major immunological mechanisms drive vessel wall injury:
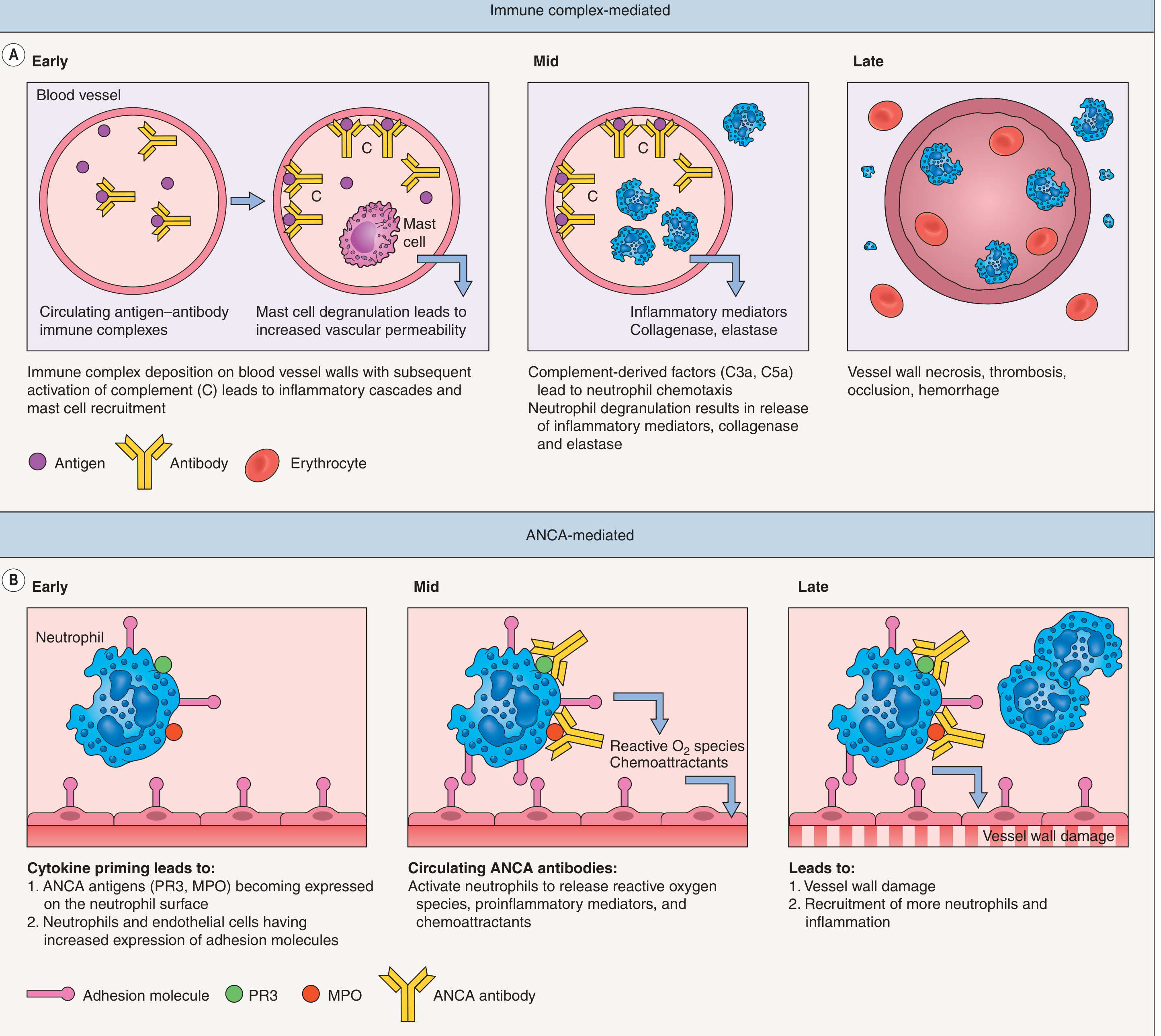
A. Immune Complex-Mediated (e.g., IgA vasculitis, cryoglobulinemic vasculitis)
- Circulating antigens (infections, drugs, neoplasms) stimulate antibody formation
- Antibody-antigen immune complexes deposit in postcapillary venule walls
- Complement activation generates C3a and C5a - potent mast cell degranulators and neutrophil chemoattractants
- Mast cell degranulation increases vascular permeability, enhancing immune complex deposition
- Adhesion molecules (E-selectin, ICAM-1, VCAM-1) upregulate on endothelium, tethering neutrophils
- Neutrophils release proteolytic enzymes (collagenase, elastase) and reactive oxygen species
- Membrane attack complex (C5-C9) activates the clotting cascade → thrombosis, necrosis, hemorrhage
B. ANCA-Mediated (pauci-immune; no significant immune complex deposits)
- Cytokine priming (e.g., TNF) causes intracellular neutrophil proteins - PR3 (proteinase 3) and MPO (myeloperoxidase) - to translocate to the cell surface
- Autoantibodies (ANCAs) form against these surface-expressed antigens
- ANCA binding activates neutrophils, increasing their adhesion to vessel walls
- Activated neutrophils release reactive oxygen species and toxic mediators → direct vessel wall damage
- Impaired neutrophil apoptosis may prolong the window for autoantibody development
- Dermatology 2-Volume Set (Elsevier, 5e), p. 506
Clinical Features by Vessel Size
The skin and organ findings correlate tightly with vessel caliber:
| Organ System | Small Vessel | Medium Vessel | Large Vessel |
|---|---|---|---|
| Skin | Palpable purpura (hallmark) | Livedo reticularis, subcutaneous nodules | Cyanosis, claudication |
| Kidney | Hematuria + RBC casts, proteinuria | Hematuria, flank pain, infarct | Hypertension (renal artery stenosis) |
| GI | GI bleeding | Bowel perforation | Bowel infarction |
| Nervous | Polyneuropathy | Mononeuritis multiplex, strokes | Strokes, TIA |
| Lung | Pulmonary capillaritis, hemorrhage | - | - |
Palpable purpura is the hallmark of small-vessel (postcapillary venule) disease. Lesions predominate on the lower legs and ankles (gravity-dependent areas). In bedridden patients, the buttocks may be affected.

Leukocytoclastic vasculitis showing classic palpable purpura - Andrews' Diseases of the Skin
Key Individual Diseases
1. Giant Cell Arteritis (GCA) - Large Vessel
- Most common systemic vasculitis in people >50 years (median onset age 75); 4x more common in women
- Affects the temporal artery and branches of the external carotid
- Presents with: temporal headache, jaw claudication (very specific), scalp tenderness, visual loss (ischemic optic neuropathy - an emergency), 40-50% overlap with polymyalgia rheumatica (PMR)
- Elevated ESR (often >50 mm/hr) and CRP
- Treated with high-dose glucocorticoids (prednisone 1 mg/kg/day) urgently; tocilizumab (IL-6 inhibitor) as steroid-sparing therapy
2. Takayasu Arteritis - Large Vessel
- "Pulseless disease" - affects the aorta and its main branches
- Most common in Asian women in the third decade of life
- Three phases: (1) constitutional symptoms, (2) vessel pain/tenderness (carotidynia), (3) fibrotic/ischemic phase with absent pulses, limb claudication, hypertension, strokes
- Treated with glucocorticoids + steroid-sparing agents (methotrexate, azathioprine, anti-TNF, tocilizumab)
3. Polyarteritis Nodosa (PAN) - Medium Vessel
- Necrotizing arteritis of medium arteries WITHOUT glomerulonephritis or capillaritis
- ANCA-negative; 30% associated with hepatitis B
- Features: livedo reticularis, subcutaneous nodules, mononeuritis multiplex, renal infarcts (but NOT glomerulonephritis), mesenteric ischemia
- Treatment: glucocorticoids; cyclophosphamide for severe disease
4. ANCA-Associated Vasculitis (AAV) - Small Vessel, Pauci-immune
Granulomatosis with Polyangiitis (GPA) - formerly Wegener's
- Classic triad: upper respiratory tract (sinusitis, saddle-nose deformity, subglottic stenosis) + lower respiratory tract (nodules, cavities) + renal disease (crescentic GN)
- c-ANCA / PR3-ANCA positive in ~90% of generalized disease
Microscopic Polyangiitis (MPA)
- Capillaritis and glomerulonephritis WITHOUT granulomas or upper respiratory involvement
- p-ANCA / MPO-ANCA positive
- Pulmonary-renal syndrome common
Eosinophilic Granulomatosis with Polyangiitis (EGPA) - formerly Churg-Strauss
- Triad: asthma + eosinophilia (>10%) + granulomatous vasculitis
- Classic cardiac involvement (eosinophilic cardiomyopathy)
- p-ANCA positive in ~50%
2022 ACR/EULAR classification criteria for AAV use weighted scoring systems with >90% sensitivity and specificity - Firestein & Kelley's Rheumatology, p. 1945
5. IgA Vasculitis (Henoch-Schönlein Purpura) - Small Vessel, Immune Complex
- Most common vasculitis in children (though adults can be affected)
- Classic tetrad: palpable purpura (lower extremities) + arthralgia/arthritis + abdominal pain + renal disease (hematuria, proteinuria)
- Defining feature: IgA deposits in vessel walls on immunofluorescence
- Usually self-limiting (6-16 weeks); treatment is primarily supportive
- Renal prognosis worse in adults than children
Histology
The classic finding in small-vessel vasculitis is leukocytoclastic vasculitis (LCV):
- Segmental inflammation of postcapillary venules
- Fibrinoid necrosis of vessel walls
- Neutrophil infiltration with nuclear fragmentation (karyorrhexis/leukocytoclasia)
- Endothelial cell swelling, vascular thrombosis
- On immunofluorescence: immunoglobulins, complement, and fibrin in vessel walls (if biopsy taken within 24 hours)
- IgA deposits persist longer in IgA vasculitis and are the diagnostic hallmark
Etiology
| Category | Examples |
|---|---|
| Idiopathic | Most cases of cutaneous LCV |
| Infections | Hepatitis B (PAN), Hepatitis C (cryoglobulinemic vasculitis), HIV, streptococcal infection (IgA vasculitis) |
| Drugs | Penicillins, sulfonamides, allopurinol, propylthiouracil (drug-induced ANCA vasculitis) |
| Autoimmune | Rheumatoid arthritis, SLE, Sjögren syndrome |
| Malignancy | Lymphoreticular malignancies > solid tumors; IgA vasculitis in adults can be malignancy-associated |
| Genetic | HLA associations; environmental triggers |
Diagnosis
- Clinical suspicion: systemic symptoms + unexplained organ dysfunction or palpable purpura
- Labs: CBC, ESR, CRP, ANCA (c-ANCA/PR3-ANCA, p-ANCA/MPO-ANCA), cryoglobulins, complement (C3, C4), hepatitis serology, ANA, urinalysis
- Imaging: CT/MR angiography for large/medium vessel disease; PET scan for active arteritis
- Tissue biopsy: Skin (punch biopsy within 24-48 hours), temporal artery, kidney, or lung - to confirm diagnosis and guide classification
- 2022 ACR/EULAR criteria now available for GPA, MPA, EGPA, GCA, Takayasu, PAN, IgA vasculitis
Treatment Principles
| Disease Category | Induction | Maintenance |
|---|---|---|
| AAV (GPA, MPA, EGPA) | High-dose glucocorticoids + rituximab or cyclophosphamide | Rituximab or azathioprine; taper steroids |
| GCA | Prednisone 40-60 mg/day | Tocilizumab (anti-IL-6); slow steroid taper over 12-24 months |
| Takayasu | Prednisone 1 mg/kg/day | Methotrexate, azathioprine, tocilizumab, anti-TNF agents |
| PAN | Prednisone ± cyclophosphamide | Steroid taper |
| IgA vasculitis | Supportive (colchicine, dapsone for skin) | Steroids for GI/renal disease; IVIG for refractory cases |
| Cutaneous LCV | Remove offending cause (drug, infection) | Usually self-resolving in 3-4 weeks |
Summary
Vasculitis is best understood through the lens of vessel size + mechanism:
- Large vessel: granulomatous inflammation, ischemic symptoms (GCA, Takayasu)
- Medium vessel: necrotizing arteritis causing organ infarction (PAN, Kawasaki)
- Small vessel, pauci-immune (ANCA+): direct neutrophil-mediated damage, glomerulonephritis, pulmonary hemorrhage
- Small vessel, immune complex: complement-driven inflammation, palpable purpura, IgA deposits (HSP)
The 2022 ACR/EULAR classification criteria (PMID: 38913291) represent the current standard for research classification, though clinical diagnosis requires integrating serology, biopsy, and imaging findings.
This is a shared conversation. Sign in to Orris to start your own chat.