Anatomy of mediastinum and it's applied anatomy full details for md exam answer 10 marks from fishman and Murray combined structured condensed
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from both Fishman's and Murray's. Let me compose the full structured 10-mark MD exam answer.
Anatomy of the Mediastinum and Applied Anatomy
Sources: Fishman's Pulmonary Diseases and Disorders, 2-Volume Set | Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set
1. DEFINITION AND BOUNDARIES
The mediastinum is the potential space between the two pleural cavities. Its boundaries are:
| Boundary | Structure |
|---|---|
| Anterior | Sternum |
| Posterior | Vertebral column |
| Superior | Thoracic inlet |
| Inferior | Diaphragm |
| Lateral | Mediastinal pleural reflections (bilateral) |
It communicates superiorly with the neck (via fascial planes) and inferiorly with the retroperitoneum - a fact of critical applied anatomical importance. (Fishman's, Ch. 80)
2. COMPARTMENTS OF THE MEDIASTINUM
Classical Three-Compartment Model (Shields, 1972)
The most widely used surgical and radiological subdivision. Each compartment extends from the thoracic inlet to the diaphragm.
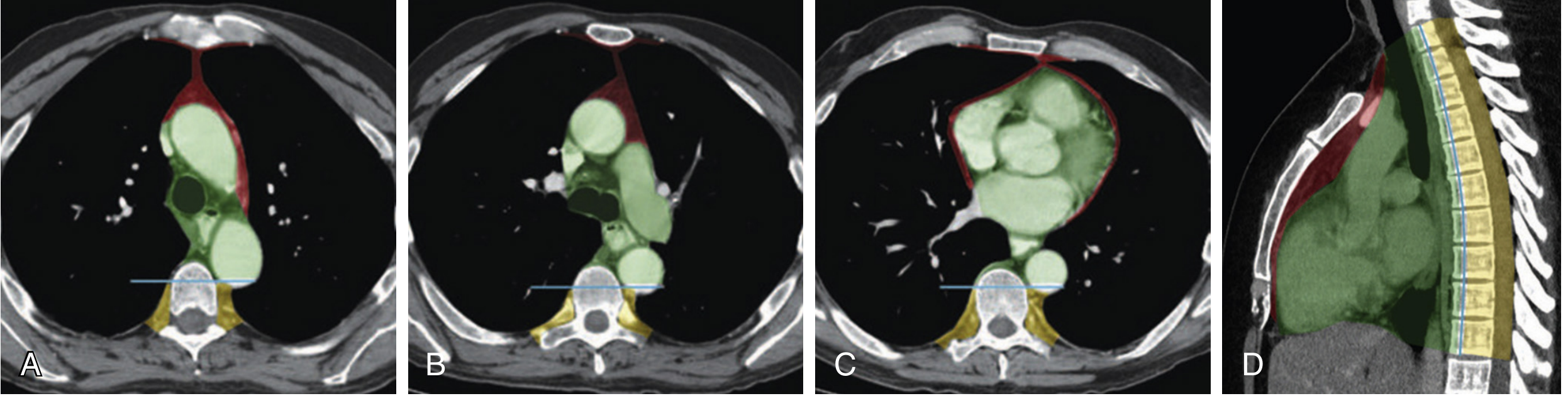
ITMIG CT-Based Classification (International Thymic Malignancy Interest Group)
A modern refinement renaming the compartments as prevascular (anterior), visceral (middle), and paravertebral (posterior), based on axial CT landmarks rather than lateral radiograph lines.
A. Anterior (Prevascular) Compartment
Boundaries:
- Anterior: posterior table of the sternum and first rib
- Posterior: anterior pericardium, anterior surface of great vessels; an imaginary curved line following the anterior heart border and brachiocephalic vessels from thoracic inlet to diaphragm
Contents:
- Thymus gland
- Pericardial fat
- Lymph nodes
- Internal mammary (thoracic) arteries and veins
- Substernal extensions of thyroid and parathyroid glands
(Fishman's, Ch. 82; Murray & Nadel, Ch. 115)
B. Middle (Visceral) Compartment
Boundaries:
- Anterior: anterior surface of pericardium
- Posterior: a vertical line on CT connecting a point 1 cm posterior to the anterior margin of each thoracic vertebral body
Contents:
- Heart and pericardium
- Trachea and main bronchi
- Ascending and transverse aorta; aortic arch with its major branches
- Innominate (brachiocephalic) veins and superior vena cava (SVC)
- Pulmonary arteries and hila
- Esophagus
- Descending aorta, azygos and hemiazygos veins
- Paravertebral lymph nodes
- Thoracic duct
- Phrenic nerve and upper vagus nerve
(Murray & Nadel, Ch. 115)
C. Posterior (Paravertebral) Compartment
Boundaries: Posterior to the middle compartment limits; posterolateral boundaries defined by a vertical line at the posterior margin of the chest wall at the lateral margin of transverse processes.
Contents:
- Azygos and hemiazygos veins (traditionally; per ITMIG now in visceral)
- Thoracic duct
- Sympathetic trunk and chains
- Intercostal nerves
- Structures emerging from spinal canal
- Lower portions of vagus nerve
(Fishman's, Ch. 80, Table 80-1)
Summary Table - Contents of Mediastinal Compartments (Fishman, Table 80-1):
| Anterior | Middle (Visceral) | Posterior (Paravertebral) |
|---|---|---|
| Thymus gland | Pericardium + Heart | Azygos/hemiazygos veins |
| Pericardial fat | Trachea and main bronchi | Thoracic duct |
| Lymph nodes | Esophagus | Sympathetic trunk |
| Internal mammary vessels | Aorta | Intercostal nerves |
| Phrenic and vagus nerves | ||
| Lymph nodes |
3. MEDIASTINAL LYMPHATICS
The mediastinal lymphatic system is complex and variable. Lymph node groups are extensively interconnected, so involvement of one station frequently spreads to others. (Fishman's, Ch. 80)
- Naruke (1978) lymph node map is the standard for staging thoracic malignancies (lung cancer)
- Stations 1-9: True mediastinal lymph nodes
- Stations 10+: Lymph nodes within the pleural sac (extrapulmonary hilar nodes)
Key mediastinal nodal stations clinically:
- Station 2/4 (upper/lower paratracheal) - right and left
- Station 5 (aortopulmonary window) - left side only
- Station 6 (anterior mediastinal/pre-aortic)
- Station 7 (subcarinal) - most important for bronchogenic carcinoma staging
- Station 8/9 (paraesophageal/pulmonary ligament)
The thoracic duct (arising from the cisterna chyli, ascending in the posterior mediastinum, crossing at T4-T5 to the left side, and draining into the left subclavian-jugular junction) is a key landmark.
4. FASCIAL PLANES AND COMMUNICATIONS - KEY APPLIED ANATOMY
The deep layer of deep cervical fascia ensheathing the trachea and esophagus descends into the mediastinum as a continuous visceral space. This means:
- Air, blood, or infection can track between the neck, mediastinum, and retroperitoneum through these fascial planes
- The bronchovascular sheath merges with the pericardium, explaining spread of air or infection from alveolar rupture into the mediastinum (pneumomediastinum)
- The pericardial sac is the only true anatomical compartment - it provides a strong barrier to infection
(Fishman's, Ch. 80, Fig. 80-4)
5. APPLIED ANATOMY - CLINICAL SIGNIFICANCE
A. Mediastinal Mass - Compartmental Differential Diagnosis
Knowledge of compartmental contents allows systematic diagnosis of any mediastinal mass:
| Compartment | Common Masses (Adults) | Common Masses (Children) |
|---|---|---|
| Anterior | Thymoma, Teratoma/GCT, Thyroid, lymphoma (4 T's) | Lymphoma, GCT |
| Middle | Lymphoma, bronchogenic cyst, tracheal tumors, pericardial cyst, vascular anomalies | Bronchogenic cyst, lymphoma |
| Posterior | Neurogenic tumors (schwannoma, neurofibroma), esophageal tumors | Neurogenic tumors (most common) |
- In adults: Thymoma + thymic cysts (26.5%) and neurogenic tumors (20.2%) are most common
- In children: Neurogenic tumors predominate (41.6%)
- Malignancy rate: Anterior 59% > Middle 29% > Posterior 16% (Fishman's, Ch. 82)
- >80% of asymptomatic masses are benign; >50% of symptomatic masses are malignant (Murray & Nadel, Ch. 115)
B. SVC Syndrome
The SVC is particularly vulnerable because it is thin-walled with low intravascular pressure. Masses in the middle mediastinum (most commonly bronchogenic carcinoma and lymphoma) compress the SVC:
- Clinical features: Dilation of collateral veins (upper thorax, neck), facial/neck/upper torso edema and plethora, headache, visual disturbance, altered consciousness
- The Pemberton sign (facial plethora on raising both arms) indicates thoracic inlet obstruction
(Murray & Nadel, Ch. 115)
C. Nerve Compression Syndromes
| Nerve | Compartment | Effect of Compression/Invasion |
|---|---|---|
| Recurrent laryngeal nerve | Middle (loops under aortic arch on left) | Hoarseness |
| Phrenic nerve | Middle | Diaphragmatic paralysis, dyspnea |
| Vagus nerve | Middle/Posterior | Tachycardia, autonomic dysfunction |
| Sympathetic chain | Posterior | Horner syndrome (ptosis, miosis, anhidrosis) |
| Spinal cord (posterior) | Posterior | Cord compression |
D. Pneumomediastinum
Air in the mediastinum (mediastinal emphysema) spreads via fascial planes:
- Macklin effect: Alveolar rupture → perivascular interstitium → bronchovascular sheath → mediastinum
- Air dissects into pericardium (pneumopericardium), subcutaneous tissue, neck, retroperitoneum
- Pneumomediastinum rupturing into the pleural space = pneumothorax
- Hamman's sign: Crunching systolic sound on auscultation
(Fishman's, Ch. 80)
E. Mediastinitis
- Acute mediastinitis: Surgical emergency. Sources: descending necrotizing mediastinitis from oropharyngeal/dental infections (tracking down fascial planes), esophageal perforation (Boerhaave syndrome), or post-sternotomy
- Spread is facilitated by the continuous fascial plane connecting neck → mediastinum → retroperitoneum
- Descending infection from oropharynx can reach the mediastinum within hours
- Chronic fibrosing mediastinitis: Most commonly from Histoplasma capsulatum; may cause SVC obstruction, esophageal obstruction, constrictive pericarditis
F. Thymoma and Myasthenia Gravis
- Thymoma is the most common anterior mediastinal neoplasm in adults
- 40-70% have paraneoplastic syndromes; myasthenia gravis in 10-50% (autoantibodies to postsynaptic acetylcholine receptor)
- Other associations: pure red cell aplasia, hypogammaglobulinemia, collagen vascular disease
G. Imaging Landmarks
CT is the investigation of choice for mediastinal evaluation. Key CT features with diagnostic relevance (Murray & Nadel, Ch. 115, Table 115.1):
| CT Feature | Likely Etiology |
|---|---|
| Bulky anterior mass | Lymphoma, GCT, thymic neoplasm |
| Fat density | Mediastinal lipomatosis, thymolipoma, teratoma |
| Rim calcification | Cystic thymoma, thyroid adenoma, aneurysm |
| Central calcification | Germ cell tumor, granulomatous disease |
| Cystic mass | Bronchogenic cyst, pericardial cyst, cystic thymoma |
6. IMPORTANT ANATOMICAL MNEMONICS FOR EXAM
Anterior mediastinal masses - "4 T's":
- Thymoma
- Teratoma / Germ Cell Tumors
- Thyroid (substernal)
- Terrible lymphoma (non-Hodgkin's)
Posterior mediastinal masses - "3 N's":
- Neurogenic tumors (most common)
- Nodal masses (lymphoma)
- Nullify esophageal tumors (esophageal lesions)
SUMMARY TABLE: High-Yield Points for 10-Mark Answer
| Feature | Key Fact |
|---|---|
| Anterior boundary | Sternum |
| Posterior boundary | Vertebral column |
| Only true anatomical compartment | Pericardial sac |
| Most common mediastinal mass (adults) | Thymoma + thymic cysts |
| Most common mediastinal mass (children) | Neurogenic tumors |
| Most malignant compartment | Anterior (59%) |
| Compartment with SVC | Middle |
| Hoarseness due to | Recurrent laryngeal nerve compression (middle) |
| Horner syndrome due to | Sympathetic chain (posterior) |
| Fascial plane connects | Neck - Mediastinum - Retroperitoneum |
| Lymph node staging map | Naruke map (stations 1-9 = mediastinal) |
| ITMIG classification | Prevascular / Visceral / Paravertebral |
| Pneumomediastinum mechanism | Macklin effect |
| Most common cause of SVC syndrome | Bronchogenic carcinoma, then lymphoma |
Based on: Fishman's Pulmonary Diseases and Disorders (Ch. 80 - Nonneoplastic Disorders of the Mediastinum; Ch. 82 - Primary Benign and Malignant Neoplasms) and Murray & Nadel's Textbook of Respiratory Medicine (Ch. 115 - Diseases of the Mediastinum)
This is a shared conversation. Sign in to Orris to start your own chat.