Give answer on Silicosis for md exams 10 marks from fishman and murray only
Reading File
Give answer on asbestosis for md exams 10 marks from fishman and murray only
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete MD exam answer on Asbestosis sourced exclusively from Fishman's Pulmonary Diseases and Disorders (5th ed.) and Murray & Nadel's Textbook of Respiratory Medicine.
ASBESTOSIS
Definition
Asbestosis is a diffuse interstitial pulmonary fibrosis caused by the inhalation and accumulation of asbestos fibers in the lung parenchyma. It is a dose-dependent pneumoconiosis with a long latency period between exposure and clinical disease.
Fiber Types and Occupational Exposure
Asbestos is a fibrous hydrated magnesium silicate with six commercial forms: chrysotile (serpentine - wavy, long bundles), crocidolite, amosite, anthophyllite, actinolite, and tremolite (the last four are amphiboles). The key distinction is:
- Chrysotile (most common in the US): wavy, long fibers that tend to split longitudinally, multiplying the asbestos effect even after exposure stops
- Amphiboles (crocidolite, amosite): needle-shaped, more biopersistent, associated with higher rates of asbestosis, mesothelioma, and lung cancer than chrysotile alone
High-risk occupations include asbestos insulators ("laggers"), boilermakers, plumbers, pipefitters, sheet metal workers, shipyard workers, and building custodians. The WHO estimates 255,000 deaths annually from asbestos-related diseases (3,500 from asbestosis, 30,000 from mesothelioma, 184,000 from lung cancer).
Fishman's Pulmonary Diseases and Disorders, Ch. 85; Murray & Nadel, Ch. 101
Pathogenesis
Asbestos fibers are deposited at airway bifurcations and in respiratory bronchioles and alveoli by impaction, sedimentation, and interception. Fibers migrate into the interstitium via type I alveolar epithelial cells, causing alveolar macrophage alveolitis. The key events are:
- Macrophage activation: Alveolar macrophages engulf fibers but fail to clear them completely. Long fibers (>5 µm) resist complete phagocytosis and induce apoptosis of macrophages.
- Cytokine release: Activated macrophages release PDGF, IGF-1, TGF-β, IL-1β, TNF-α, IL-8, fibronectin, and oxygen free radicals. These stimulate fibroblast proliferation, chemotaxis, and collagen synthesis.
- Asbestos bodies: Fibers coated by iron and hemosiderin form ferruginous (asbestos) bodies - beaded, clubbed structures identifiable on light microscopy. The vast majority of fibers remain uncoated in the lung.
- Fibrosis: If the retained dust load is high and macrophage phagocytosis is incomplete, fibroblasts are recruited, proliferate, and lay down collagen, leading to irreversible chronic interstitial fibrosis.
The transcription factors AP-1 and NF-κB are activated by asbestos in mononuclear phagocytes, driving cytokine and growth factor release. BAL shows macrophage alveolitis with modest neutrophilia; neutrophilia correlates with clinical disease activity and is more pronounced in advanced disease.
Fishman's Ch. 85; Murray & Nadel Ch. 101
Pathology
Asbestosis is most prominent in the lower lobes and subpleural areas. Progression occurs in stages:
- Early/mild: Foci of peribronchiolar fibrosis with chronic interstitial inflammation, air-space macrophage accumulation, and type 2 alveolar epithelial cell proliferation. Architecture of surrounding parenchyma is preserved.
- Progressive: Fibrosis spreads to involve 2nd and 3rd order bronchioles and alveolar ducts.
- Advanced: Lungs are small, with streaks of fibrosis outlining lobar and interlobar septa, thickened visceral pleura, and honeycombing subpleurally and in lower lobes.
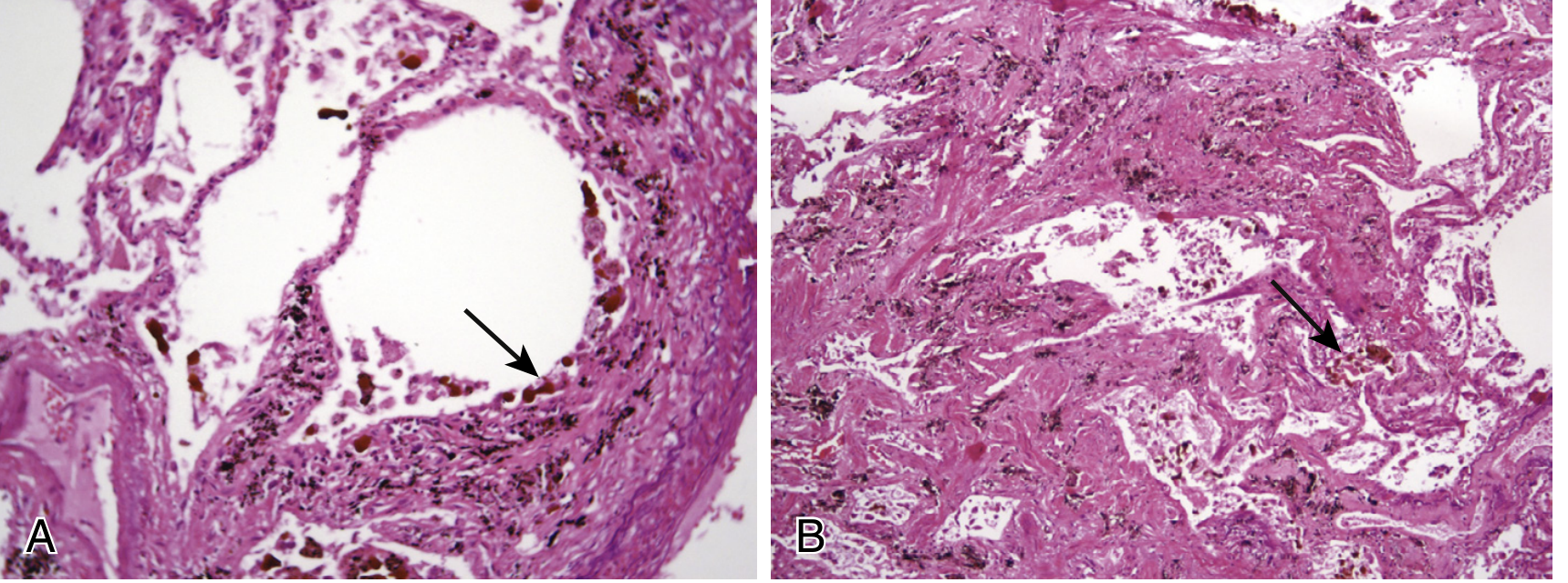
Advanced asbestos-related fibrosis is indistinguishable from other causes of advanced fibrosis except by the presence of asbestos bodies or uncoated asbestos fibers on light microscopy or mineralogic analysis.
Murray & Nadel Ch. 101
Clinical Features
Symptoms:
- Dyspnea on exertion - earliest and most consistently reported symptom
- Persistent cough (often spasmodic, with sputum production)
- Chest tightness; wheezing may occur
- Symptoms develop insidiously; may appear or worsen after exposure ceases
Signs:
- Bilateral basal rales (crackles) - the most distinctive physical finding; late to pan-inspiratory, heard best at posterior lung bases, NOT cleared by coughing. They first appear in the mid-axillary line at the bases and spread posteriorly. In surveys, ~83% of patients with higher radiographic categories had bilateral rales.
- Digital clubbing - seen in ~52% of cases (22 of 42 patients in one clinical series)
- Signs of cor pulmonale in advanced disease
Fishman's Ch. 85
Pulmonary Function Tests
The characteristic pattern is restrictive:
- Reduced FVC and total lung capacity (TLC)
- Reduced DLCO (diffusing capacity for CO) - may be abnormal even before spirometric changes
- FEV1/FVC ratio: generally well preserved (distinguishing from obstruction)
- Arterial hypoxemia at rest or on exercise
- In one longitudinal study of 77 workers, mean annual decline: FVC = 92 ± 28 mL/year, FEV1 = 66 ± 22 mL/year, TLC = 14 ± 53 mL/year
Frequency of abnormal FVC increased to >50% with prolonged follow-up in asbestos insulator cohorts. Profusion of irregular opacities on chest radiograph inversely correlates with FVC percent predicted.
Fishman's Ch. 85
Chest Imaging
Plain Chest Radiograph (ILO classification):
- Irregular opacities (s, t, u shapes) predominantly in lower lung zones (in contrast to silicosis with upper zone nodular opacities)
- ILO profusion categories 1/0 through 3/+ indicate progressive disease
- Pleural plaques (calcified or non-calcified) - parietal pleura, diaphragm, mediastinal pleura
- Diffuse pleural thickening - continuous pleural opacity, commonly blunts costophrenic angles
HRCT:
- More sensitive than plain radiography for early parenchymal fibrosis
- Findings: subpleural irregular lines, intralobular lines, honeycombing in lower lobes, traction bronchiectasis
- Demonstrates pleural plaques, diffuse pleural thickening, and their relationship to parenchymal disease
- Can identify rounded atelectasis (pseudotumor): characterized by a comet tail of vessels and bronchi sweeping into a wedge-shaped pleural-based mass, most often in the lower posterior lung - caused by folding over of fibrotic pleura trapping underlying lung
Fishman's Ch. 85; Murray & Nadel Ch. 101
Asbestos-Related Pleural Manifestations
Four distinct pleural disorders occur:
| Manifestation | Key Features |
|---|---|
| Pleural Plaques | Circumscribed, parietal pleura, diaphragm, ± calcification; latency >20 years; not premalignant per se |
| Diffuse Pleural Thickening | Visceral pleura involved; continuous sheet ≥5-10 cm; blunts costophrenic angle (90%); may cause restrictive physiology |
| Benign Pleural Effusion | Earliest pleural manifestation; latency 12-15 years; small, exudative, blood-tinged; diagnosis by exclusion; precedes pleural fibrosis |
| Rounded Atelectasis | Pseudotumor due to viscero-parietal pleural fusion; comet-tail sign on CT; lower lobes (lingula and RML in 49/74 cases) |
Benign pleural effusion diagnostic criteria (Murray & Nadel): (1) exposure history, (2) absence of other causes, (3) no tumor on 3-year follow-up. Asbestos bodies are rarely found in the fluid.
Diagnosis
Diagnosis is based on:
- Adequate exposure history to asbestos (with appropriate latency)
- Radiologic evidence of bilateral irregular lower zone opacities ± pleural disease
- Restrictive physiology with reduced DLCO
- Physical findings: bilateral basal crackles, digital clubbing
- Exclusion of other causes of pulmonary fibrosis
Lung biopsy is not routinely required. Surgical biopsy is indicated if diagnostic uncertainty exists (e.g., concern for malignancy). The ATS 2004 criteria for non-malignant asbestos-related disease are widely used.
Complications and Malignancy
Asbestosis carries risk for:
-
Lung cancer: Risk is multiplicative (not merely additive) with cigarette smoking. The relative risk of lung cancer is substantially elevated in smokers with asbestosis. Low-dose CT surveillance is recommended for asbestos-exposed workers with smoking history >30 pack-years and age >55 years (annual basis).
-
Malignant pleural mesothelioma: 85% of affected men and 50% of women have an occupational asbestos history. Latency is typically >20-30 years. Histologic types: epithelial (50%), sarcomatous (20%), biphasic/mixed (30%). Differentiation from adenocarcinoma: mesotheliomas stain positive for hyaluronic acid (Alcian blue, colloidal iron stain), are negative for CEA and B72.3, and are TTF-1 negative.
-
Connective tissue disease: Asbestos exposure is associated with increased risk of autoimmune diseases.
Fishman's Ch. 85
Management and Prevention
- No established specific treatment alters the course of asbestosis. There is no proven disease-modifying therapy.
- Patients with end-stage disease may be considered for lung or heart-lung transplantation (though technical difficulties arise due to associated pleural disease).
- Smoking cessation is the single most important modifiable risk factor - smoking multiplies the lung cancer risk and may contribute to initiation and progression of parenchymal fibrosis.
- Medical surveillance: Annual low-dose CT for high-risk individuals (>30 pack-years, age >55).
- Further asbestos exposure should be avoided once the diagnosis is established - even without additional exposure, disease may progress because of the dust load already in the lungs.
- Occupational and employment advice should be given; notification of asbestos-related disease is mandatory in many jurisdictions.
- Workers with pleural fibrosis or plaques are at increased risk for parenchymal fibrosis, mesothelioma, and lung cancer and require ongoing surveillance.
Murray & Nadel Ch. 101; Fishman's Ch. 85
Key Differentiating Points (Exam-Relevant Summary)
| Feature | Asbestosis | Silicosis |
|---|---|---|
| Fiber/dust | Asbestos (amphiboles > chrysotile) | Crystalline silica (RCS) |
| Distribution of opacities | Lower zone, irregular (s,t,u) | Upper zone, nodular (p,q,r) |
| Pleural plaques | YES - characteristic | Rare (eggshell calcification of lymph nodes) |
| Malignancy risk | Lung cancer + Mesothelioma | Lung cancer |
| Pathology | Diffuse interstitial fibrosis, asbestos bodies | Silicotic nodules, whorled collagen |
| Physiology | Restrictive | Restrictive (may have obstruction) |
| Smoking interaction | Multiplicative for lung cancer | Additive for airflow obstruction |
Sources: Fishman's Pulmonary Diseases and Disorders (5th edition), Chapter 85 (Asbestos-Related Lung Disease); Murray & Nadel's Textbook of Respiratory Medicine (7th edition), Chapter 101 (Pneumoconioses - Asbestos-Related Fibrosis of the Lungs and Pleura).
This is a shared conversation. Sign in to Orris to start your own chat.