systemic examination of cvs
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a comprehensive guide to the Systemic Examination of the Cardiovascular System (CVS), drawn from Harrison's Principles of Internal Medicine, 22nd Edition (2025).
Systemic Examination of the CVS
The cardiovascular examination proceeds in a structured sequence: general inspection → vital signs → jugular venous pressure → arterial pulse → precordial inspection/palpation → auscultation → peripheral vascular examination.
1. General Inspection
Look for:
- Dyspnea at rest or on minimal exertion
- Cyanosis — central (lips, tongue) vs. peripheral (fingertips)
- Pallor, diaphoresis — low output states
- Malar flush — mitral stenosis
- Xanthelasma, corneal arcus — dyslipidaemia
- Clubbing — cyanotic congenital heart disease, infective endocarditis
- Splinter haemorrhages, Janeway lesions, Osler nodes — infective endocarditis
- Ankle/sacral oedema — right heart failure
- Marfanoid habitus — aortic root disease
2. Vital Signs
Blood Pressure
- Measured in the seated position, arm at heart level, after 5–10 min rest, with an appropriately sized cuff
- Cuff bladder length and width should be 80% and 40% of arm circumference, respectively
- A >20 mmHg difference between arms suggests subclavian stenosis or aortic dissection
- Measure in both arms and both legs when coarctation is suspected
- Orthostatic hypotension: fall in systolic BP >20 mmHg or diastolic >10 mmHg on standing
Heart Rate and Rhythm
- Rate, regularity, and character
3. Jugular Venous Pressure (JVP)
The internal jugular vein is preferred (directly in line with the SVC and right atrium). The JVP is the single most important bedside measure of volume status.
Technique:
- Patient at 30–45° elevation; look for pulsation above clavicle
- Measure vertical height of pulsation above the sternal angle (angle of Louis)
-
4.5 cm at 30° elevation = elevated CVP
- Venous pulsations above the clavicle in the sitting position are clearly abnormal
Abdominojugular reflux: Firm pressure on the right upper quadrant >15 s; a sustained rise >3 cm = positive. Predicts pulmonary artery wedge pressure >15 mmHg in heart failure.
JVP Waveform Components
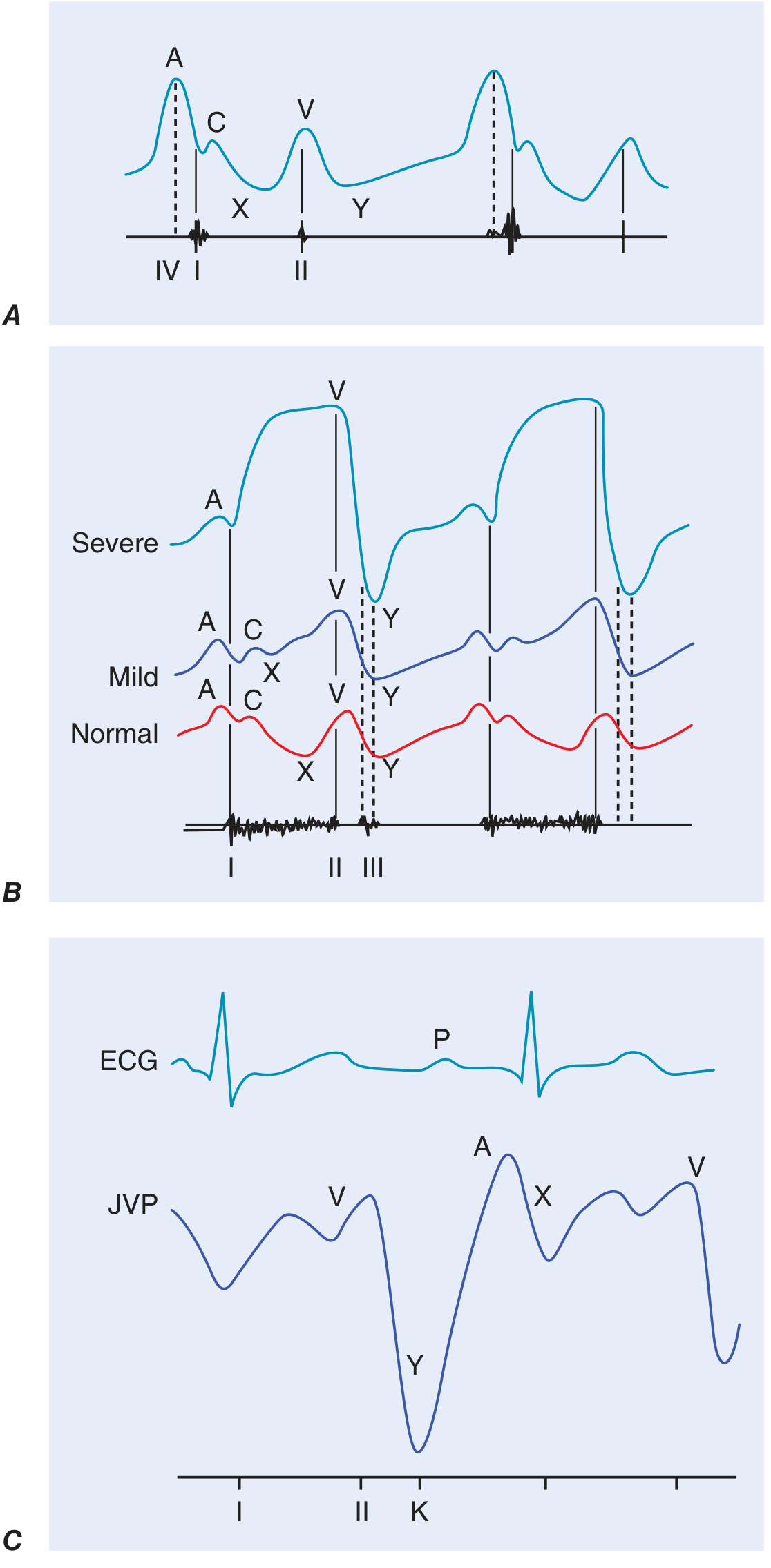
| Wave/Descent | Timing | Significance |
|---|---|---|
| a wave | Pre-systolic; after P wave, before S1 | Right atrial contraction |
| Cannon a wave | — | AV dissociation (atrial contracting against closed tricuspid) |
| Absent a wave | — | Atrial fibrillation |
| c wave | Early systole | Tricuspid valve pushed into RA |
| x descent | Systole | Fall in RA pressure after valve opening |
| v wave | During ventricular systole | Atrial filling; accentuated in tricuspid regurgitation (TR) |
| y descent | After tricuspid opens | Rapid in constrictive pericarditis (= pericardial knock) |
In TR, the v wave becomes prominent and the waveform becomes "ventriculised." In constrictive pericarditis, a sharp, rapid y descent corresponds to the pericardial knock.
4. Arterial Pulse
Assessed at the carotid (character), radial (rate/rhythm), brachial, femoral, popliteal, dorsalis pedis, and posterior tibial arteries.
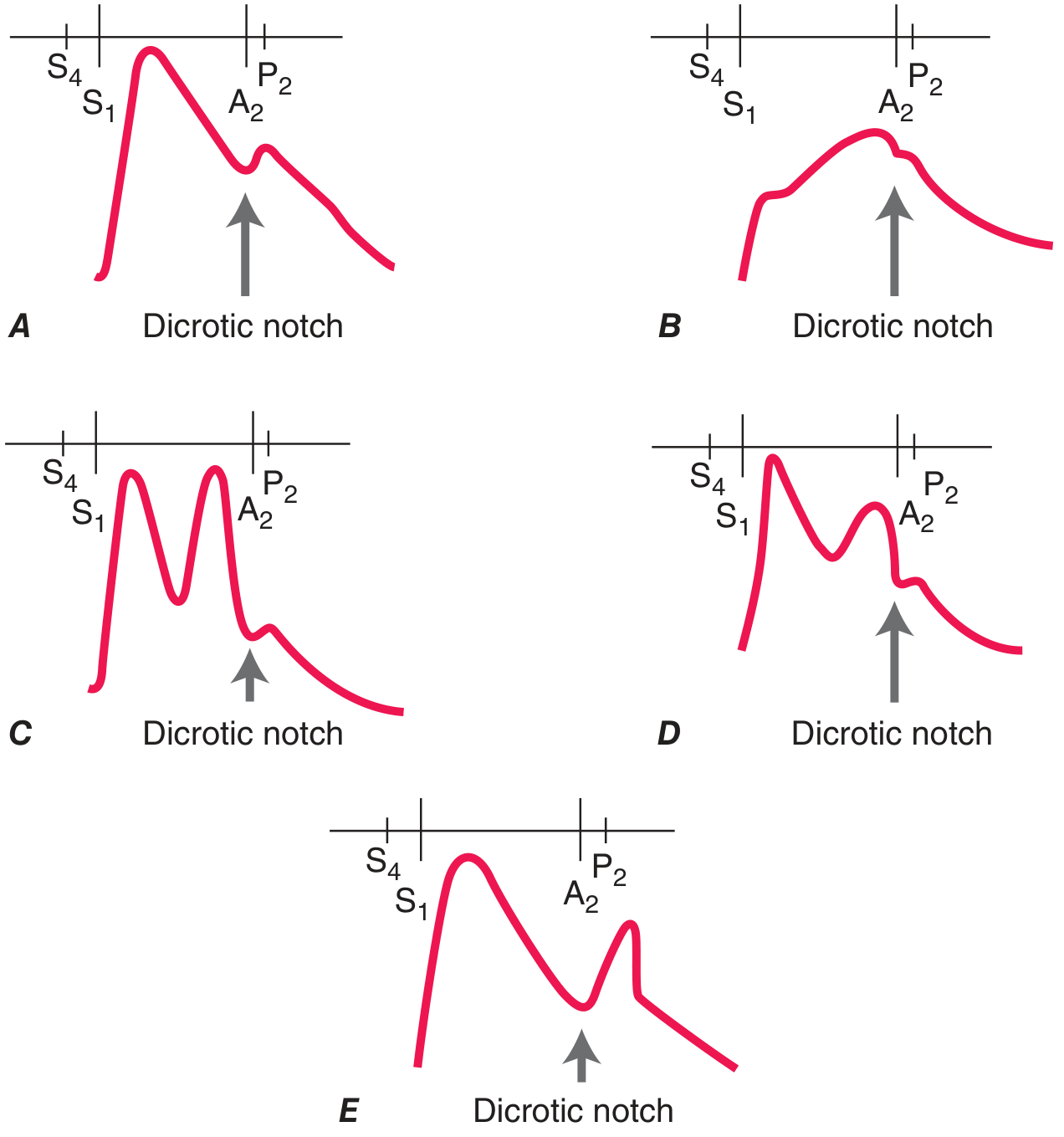
| Pulse Type | Character | Condition |
|---|---|---|
| Pulsus parvus et tardus | Weak, slow-rising | Severe aortic stenosis |
| Anacrotic pulse | Slow upstroke with notch/shudder | Severe AS |
| Corrigan's (water-hammer) pulse | Sharp rise, rapid collapse | Chronic severe aortic regurgitation (AR) |
| Bisferiens pulse | Two systolic peaks | Severe AR; HOCM (percussion + tidal waves) |
| Dicrotic pulse | Systolic + diastolic peak | Sepsis, IABP counterpulsation |
| Pulsus paradoxus | SBP fall >10 mmHg on inspiration | Cardiac tamponade, massive PE, severe asthma |
| Pulsus alternans | Beat-to-beat amplitude variation | Severe LV systolic dysfunction |
Pulsus paradoxus is measured by slowly deflating the BP cuff: note the gap between pressure where Korotkoff sounds first appear (expiration only) and where they are heard every beat.
Peripheral pulses: Assess all peripheral pulses; note bruits over carotid, subclavian, aorta, and femoral arteries. A bruit extending into diastole or associated with a thrill indicates severe stenosis.
5. Inspection and Palpation of the Precordium
Inspection
- Normal apex beat: 5th intercostal space, midclavicular line
- Visible pulsations elsewhere = abnormal
- Left anterior chest wall heave: enlarged/hyperdynamic LV or RV
- Right upper parasternal pulsation: ascending aortic aneurysm
Palpation
- Patient supine at 30°; enhanced in left lateral decubitus position
- Normal LV impulse: <2 cm diameter, taps quickly away from fingers
- Best felt in end-expiration
| Finding | Significance |
|---|---|
| Displaced apex beat (down and out) | LV dilatation |
| Sustained apex beat | Pressure overload — AS, hypertension |
| Palpable S4 (presystolic impulse) | Reduced LV compliance |
| Palpable S3 (diastolic impulse) | Volume overload, dilated cardiomyopathy |
| Parasternal heave (RV lift) | RV hypertrophy/enlargement (e.g., pulmonary hypertension) |
| Systolic thrill | Grade ≥4 murmur (turbulent flow, e.g., severe AS, VSD) |
6. Auscultation
Position and Technique
- Diaphragm for high-pitched sounds (S1, S2, aortic/mitral regurgitation murmurs)
- Bell for low-pitched sounds (S3, S4, mitral stenosis rumble)
- Auscultate at: apex (mitral), left lower sternal border (tricuspid), left upper sternal border (pulmonary), right upper sternal border (aortic)
Heart Sounds
S1 (closure of mitral + tricuspid valves):
- Loud in mitral stenosis (pliable leaflets), tachycardia, thin chest
- Soft in severe MR (leaflets don't coapt well), LV dysfunction, PR prolongation
S2 (closure of aortic [A2] + pulmonic [P2] valves):
- Normal splitting: A2 before P2; widens on inspiration (increased RV filling delays P2)
- Wide fixed splitting: ASD (fixed), RBBB
- Paradoxical (reversed) splitting: LBBB, severe AS, HCM (P2 before A2; widens on expiration)
- Loud P2: Pulmonary hypertension
S3 (ventricular gallop):
- Early diastole; heard at apex with bell
- Pathological in adults: dilated cardiomyopathy, heart failure, volume overload
- Normal in children and young adults
S4 (atrial gallop):
- Late diastole (pre-systolic); heard at apex with bell
- Reduced ventricular compliance: hypertension, AS, HOCM, acute MI
Cardiac Murmurs
Grading (Levine scale):
| Grade | Character |
|---|---|
| 1/6 | Very faint; heard only in ideal conditions |
| 2/6 | Quiet but heard immediately |
| 3/6 | Moderate; no thrill |
| 4/6 | Loud with thrill |
| 5/6 | Very loud; heard with stethoscope edge on chest |
| 6/6 | Audible without stethoscope |
Timing and key murmurs:
| Murmur | Timing | Location | Radiation | Condition |
|---|---|---|---|---|
| Ejection systolic | Systole (mid) | RUSB | Carotids | Aortic stenosis |
| Pansystolic | Throughout systole | Apex | Axilla | Mitral regurgitation |
| Pansystolic | LLSB | — | — | VSD, TR |
| Early diastolic (blowing) | Immediately after S2 | LUSB/LLSB | — | Aortic regurgitation |
| Mid-diastolic rumble | Mid-diastole | Apex | — | Mitral stenosis |
| Continuous | Systole + diastole | Below left clavicle | — | PDA |
Dynamic auscultation:
- Valsalva (decreased preload): most murmurs soften; HCM and MVP murmurs intensify
- Squatting (increased preload): HCM and MVP murmurs soften
- Inspiration: right-sided murmurs louder (Carvallo sign — TR)
- Expiration: left-sided murmurs louder
Additional Sounds
- Opening snap: Mitral stenosis; short S2–OS interval = severe MS
- Ejection click: Aortic or pulmonic valve abnormality
- Pericardial friction rub: Three-component scratchy sound; best heard with patient leaning forward
7. Peripheral Vascular Examination
- Ankle-brachial index (ABI): lower ankle pressure ÷ higher arm pressure; <0.9 = peripheral arterial disease
- Pulse oximetry discordance: >2% difference between finger and toe SpO₂ suggests lower extremity PAD
- Capillary refill time: >2 s abnormal
- Femoral/popliteal aneurysms: always examine in patients with known AAA
- Dependent rubor / pallor on elevation: chronic limb ischaemia
Summary: Key Examination Findings and Their Significance
| Sign | Likely Condition |
|---|---|
| Elevated JVP + pitting oedema + S3 | Congestive heart failure |
| Cannon a waves in JVP | AV dissociation (ventricular tachycardia) |
| Slow-rising pulse + ejection systolic murmur | Aortic stenosis |
| Collapsing pulse + early diastolic murmur | Aortic regurgitation |
| Prominent v wave in JVP + pansystolic murmur at LLSB | Tricuspid regurgitation |
| Loud P2 + parasternal heave + right-sided S4 | Pulmonary hypertension |
| Pulsus paradoxus >10 mmHg | Cardiac tamponade |
| Absent a wave in JVP | Atrial fibrillation |
| Rapid y descent in JVP + pericardial knock | Constrictive pericarditis |
Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 246 — Cardiovascular Examination.
systemic examination of cns
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.