Operative steps of openpneumonectomy
Reading File
Finding Sources
Searching the Web
open pneumonectomy operative steps technique surgery
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive material from Fischer's Mastery of Surgery (8th edition) covering both right and left pneumonectomy operative steps in detail. Here is the complete, structured answer:
Open Pneumonectomy - Operative Steps
Patient Positioning & Approach
The patient is placed in a lateral decubitus position. The standard approach is a posterolateral thoracotomy through the 4th or 5th intercostal space, which provides the best hilar exposure. Alternative approaches include anterior thoracotomy or hemiclamshell/clamshell incisions for large apical or anterosuperior mediastinal tumors.
One-lung ventilation via a double-lumen endotracheal tube (or bronchial blocker) is established. A thoracic epidural catheter is typically placed preoperatively for analgesia.
Right Pneumonectomy
Anatomical Considerations
- The right main pulmonary artery is longer outside the pericardium than the left, giving more room to work.
- Two-thirds of the main bronchial circumference is cartilage (horseshoe-shaped); the remaining one-third is membranous. Precise stapling orientation is required to prevent bronchial fistula.
- If there is extensive hilar adhesion, the central right pulmonary artery can be accessed between the ascending aorta and superior vena cava.
Operative Steps
Step 1 - Divide the inferior pulmonary ligament and inferior pulmonary vein
Divide the inferior pulmonary ligament. Incise the mediastinal pleura anterior and posterior to the hilum in the cranial direction. Divide the inferior pulmonary vein with a stapler.
Step 2 - Dissect station 7 (subcarinal) lymph nodes
Dissect the station 7 (subcarinal) lymph nodes. Remove station 10 (hilar) lymph nodes along the bronchus intermedius, along with the connected subcarinal nodes. This clears the area around the main bronchus and exposes the bifurcation of the main pulmonary artery.
Step 3 - Divide the superior pulmonary vein
Move to the anterior hilum and divide the superior pulmonary vein with a stapler.
Step 4 - Divide the main pulmonary artery
Dissect adipose tissue anterior to the right main pulmonary artery toward the periphery to reach the arterial sheath. Circumferentially dissect the sheath. Tape around the main pulmonary artery and clamp the central side with DeBakey forceps. Fire the stapler to divide the main pulmonary artery.
Step 5 - Division of the main bronchus
Dissect station 10 (hilar) and station 12 (lobar) lymph nodes remaining around the main bronchus. Tape around the main bronchus. Divide the main bronchus at approximately the 3rd cartilage ring, counting from the carina as zero. Cut orthogonally to the longitudinal axis. Place a TA stapler in the Sweet direction and fire. Cut off the distal cartilage to complete the pneumonectomy.
- The mechanical weak point of the bronchial stump is the membranous portion; it is important to fold the stump so that the mucous membrane faces inward.
- Reinforce with 2-0 Prolene placed on both sides of the bronchial stump in a Z-direction. Add 2-4 stitches to ensure proper introversion of the stump.
Left Pneumonectomy
Anatomical Considerations
- The left main bronchus is long, while the left main pulmonary artery is short.
- Resection of the left main bronchus must be done carefully - dividing too far from the carina creates a "dead-end pocket."
- The distance from the main trunk of the pulmonary artery to the pericardium is relatively short, leaving little room to clamp in case of arterial injury.
Operative Steps
Step 1 - Divide the inferior pulmonary ligament and inferior pulmonary vein
Divide the inferior pulmonary ligament. Incise the mediastinal pleura anterior and posterior to the hilum in the cranial direction. Divide the inferior pulmonary vein with a stapler.
Step 2 - Dissect station 7 (subcarinal) lymph nodes
Remove station 10 (hilar) lymph nodes along the bronchus intermedius and the connected station 7 (subcarinal) lymph nodes separately.
Step 3 - Divide the superior pulmonary vein
Divide the superior pulmonary vein with a stapler in the anterior hilum.
Step 4 - Divide the main pulmonary artery
Carefully remove adipose tissue anterior to the left main pulmonary artery in the peripheral direction to reach the arterial sheath. Dissect the sheath circumferentially. Tape around the main pulmonary artery and clamp the central side with DeBakey forceps. Fire the stapler to divide the main pulmonary artery.
Step 5 - Division of the main bronchus
Dissect connective tissue and lymph nodes around the left main bronchus. Tape and divide around the 3rd cartilage ring from the carina. Place a TA stapler, resect the main bronchus, and use 2-0 Prolene for introversion suturing.
Chest Closure and Postoperative Drainage
- After specimen removal, the bronchial stump is tested for air leak underwater.
- The pericardium is inspected; if opened (e.g., for intrapericardial vessel ligation), it is partially reapproximated to prevent cardiac herniation. A pericardial patch may be needed if the defect is large.
- The thoracic cavity is irrigated and a chest drain is placed (often with a balanced drainage system - no suction, to avoid mediastinal shift).
- The thoracotomy is closed in layers: intercostal muscles, serratus anterior, latissimus dorsi, subcutaneous tissue, skin.
Key Technical Points
| Issue | Principle |
|---|---|
| Bronchial stump division level | 3rd cartilage ring from carina (zero position) |
| Stapler orientation | TA stapler in Sweet direction |
| Stump reinforcement | 2-0 Prolene, membranous portion folded inward (introversion) |
| Phrenic nerve | Identify and preserve on pericardium to avoid paradoxical diaphragm motion |
| Left PA injury | Limited working space - clamp access from between aorta and SVC if needed on right; left PA is short so extra care required |
| Lymph node dissection | Stations 7, 10, 12 are routinely cleared (mandatory in cancer surgery) |
| Post-resection drainage | Balanced drainage, no suction - risk of mediastinal shift and cardiac herniation with suction |
Indications (Summary)
Right pneumonectomy: Tumors of middle or lower lobe with station 11s (superior interlobar) lymph node involvement and bronchial wall invasion, or large central tumors with extensive proximal pulmonary artery infiltration.
Left pneumonectomy: Centrally located tumors with significant proximal pulmonary artery infiltration, or lower lobe tumors with station 11 (interlobar) lymph node metastasis and pulmonary artery invasion at the fissure.
Sources: Fischer's Mastery of Surgery, 8th ed.; Bailey & Love's Short Practice of Surgery, 28th ed.
Right lung hilar anatomy
Finding Sources
Searching the Web
right lung hilum anatomy structures relations surgical
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
I now have excellent diagrams and comprehensive textbook content. Here is the complete, well-structured answer:
Right Lung Hilar Anatomy
Overview
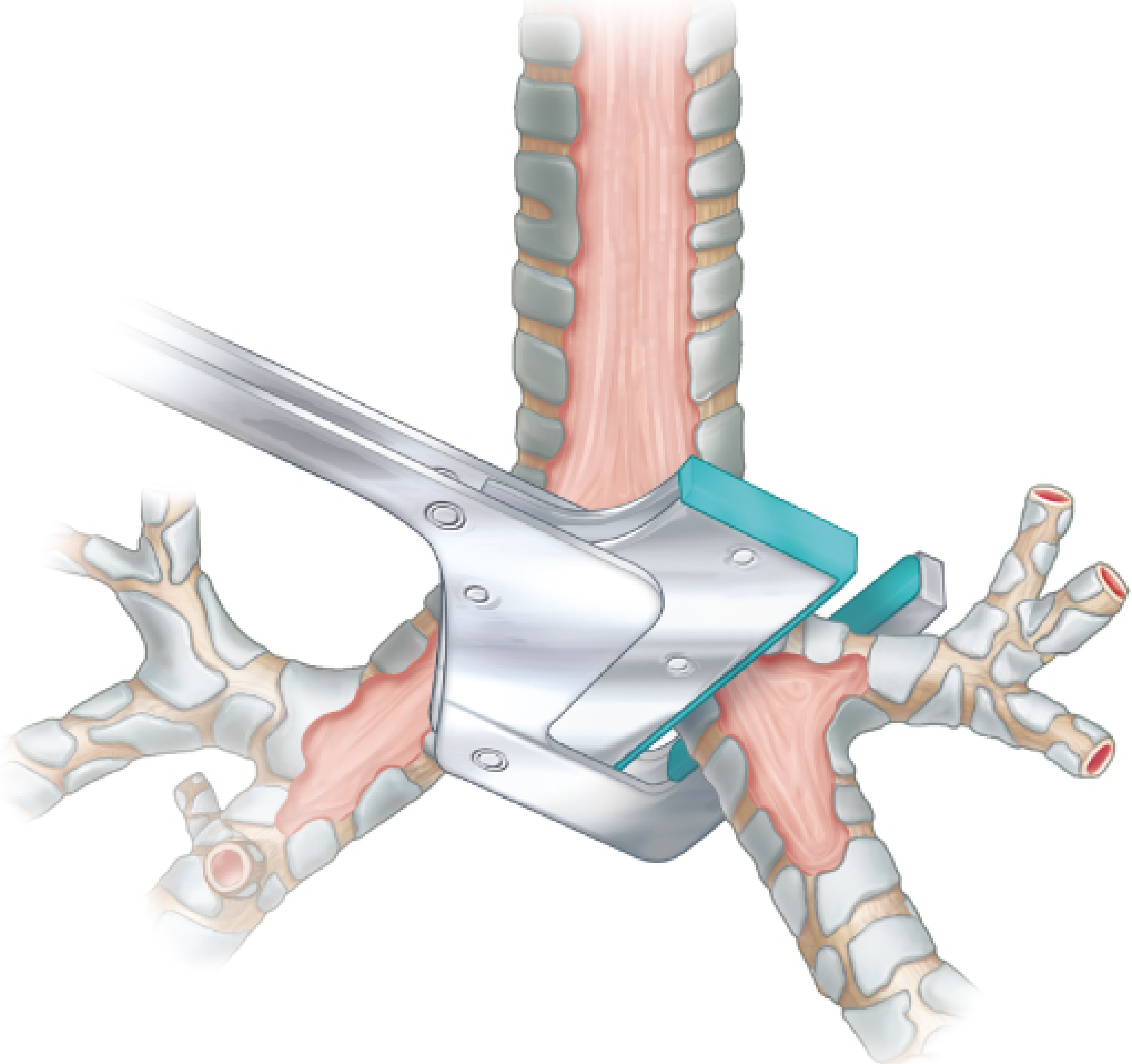
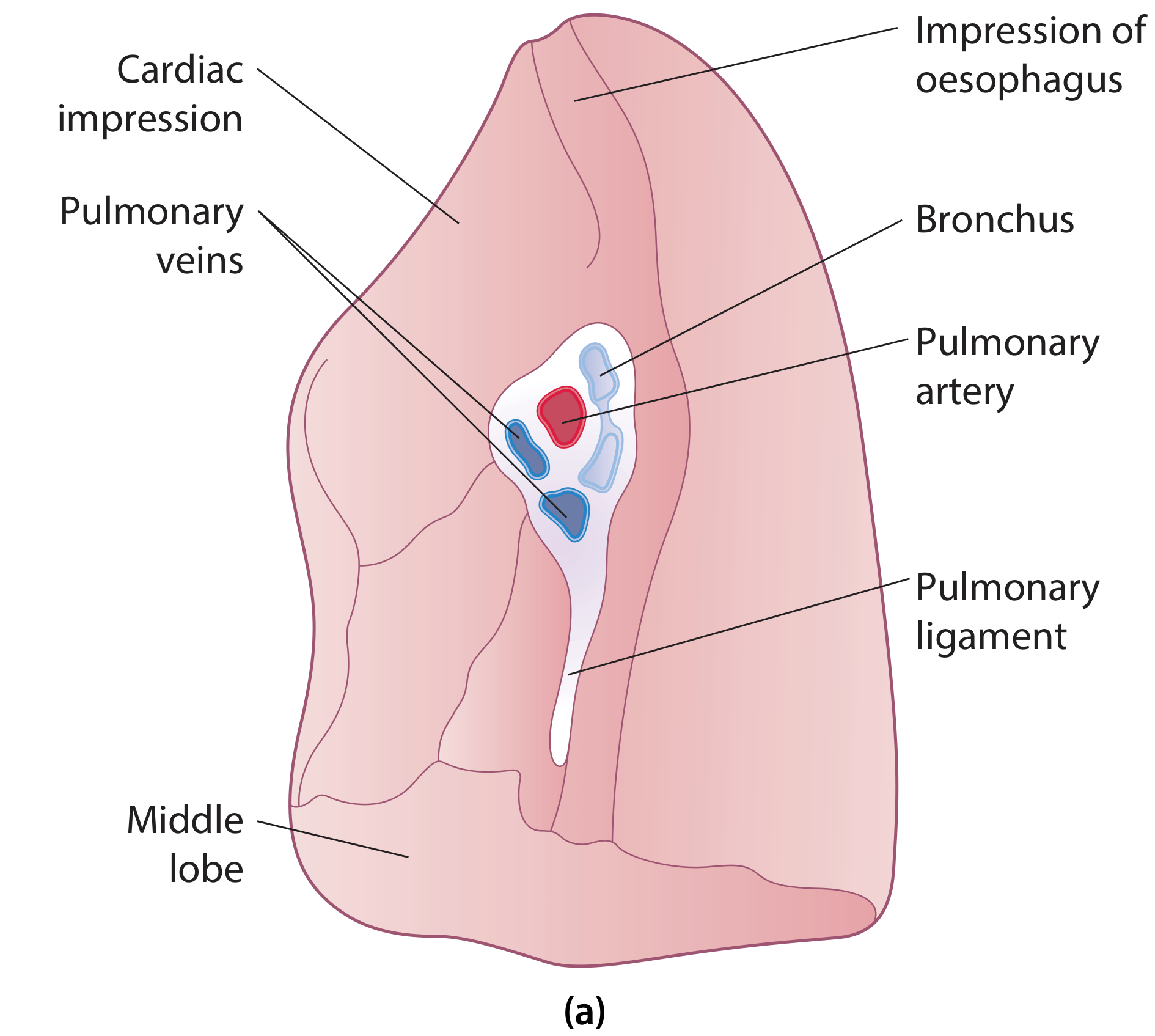
The hilum (root of the lung) is a wedge-shaped depression on the mediastinal surface of the lung, situated opposite the 5th-7th thoracic vertebrae. It is the gateway through which all structures enter and leave the lung. The right hilum differs importantly from the left.
Contents of the Right Hilum
| Structure | Number | Notes |
|---|---|---|
| Right main bronchus | 1 | Divides into upper lobe (eparterial) bronchus + bronchus intermedius |
| Pulmonary artery | 1 | Passes anterior to the right main bronchus |
| Pulmonary veins | 2 | Superior and inferior; most anterior in the hilum |
| Bronchial arteries | 1-2 | Closely follow the bronchial tree |
| Bronchial veins | - | Drain to azygos system |
| Lymphatics & lymph nodes | - | Stations 10 (hilar), 11 (interlobar) |
| Autonomic nerve plexuses | - | Anterior and posterior pulmonary plexuses |
Arrangement of Structures
Anterior-to-Posterior Order
Vein → Artery → Bronchus
- Pulmonary veins are the most anterior structures; their course is predominantly inferomedial
- Pulmonary artery lies intermediately; its course is predominantly transverse - it passes anterior to the right main bronchus (in contrast to the left PA, which arches superior to the left main bronchus)
- Bronchus is the most posterior structure; its course is superolateral
Superior-to-Inferior Order
Pulmonary artery (superior) → Upper lobe bronchus → Bronchus intermedius → Superior pulmonary vein → Inferior pulmonary vein (inferior)
- The right upper lobe (eparterial) bronchus arises above the level of the right pulmonary artery - this is why it is called "eparterial" (above the artery). This feature is unique to the right side.
- All other lobar bronchi on both sides are hyparterial (below the artery)
Relations of the Right Hilum
| Direction | Relation |
|---|---|
| Anterior | Superior vena cava (SVC); right phrenic nerve + pericardiophrenic vessels (in mediastinal adventitia on pericardial sac - the only longitudinal structures anterior to the root) |
| Posterior | Right vagus nerve; esophagus (the vagus passes posteriorly near the tracheal bifurcation and associates with the esophagus) |
| Superior | Arch of the azygos vein (crosses from posterior mediastinum to SVC just cephalad to the hilum - a constant and important surgical landmark) |
| Inferior | Pulmonary ligament (a pleural sleeve extending inferiorly, allowing hilar movement) |
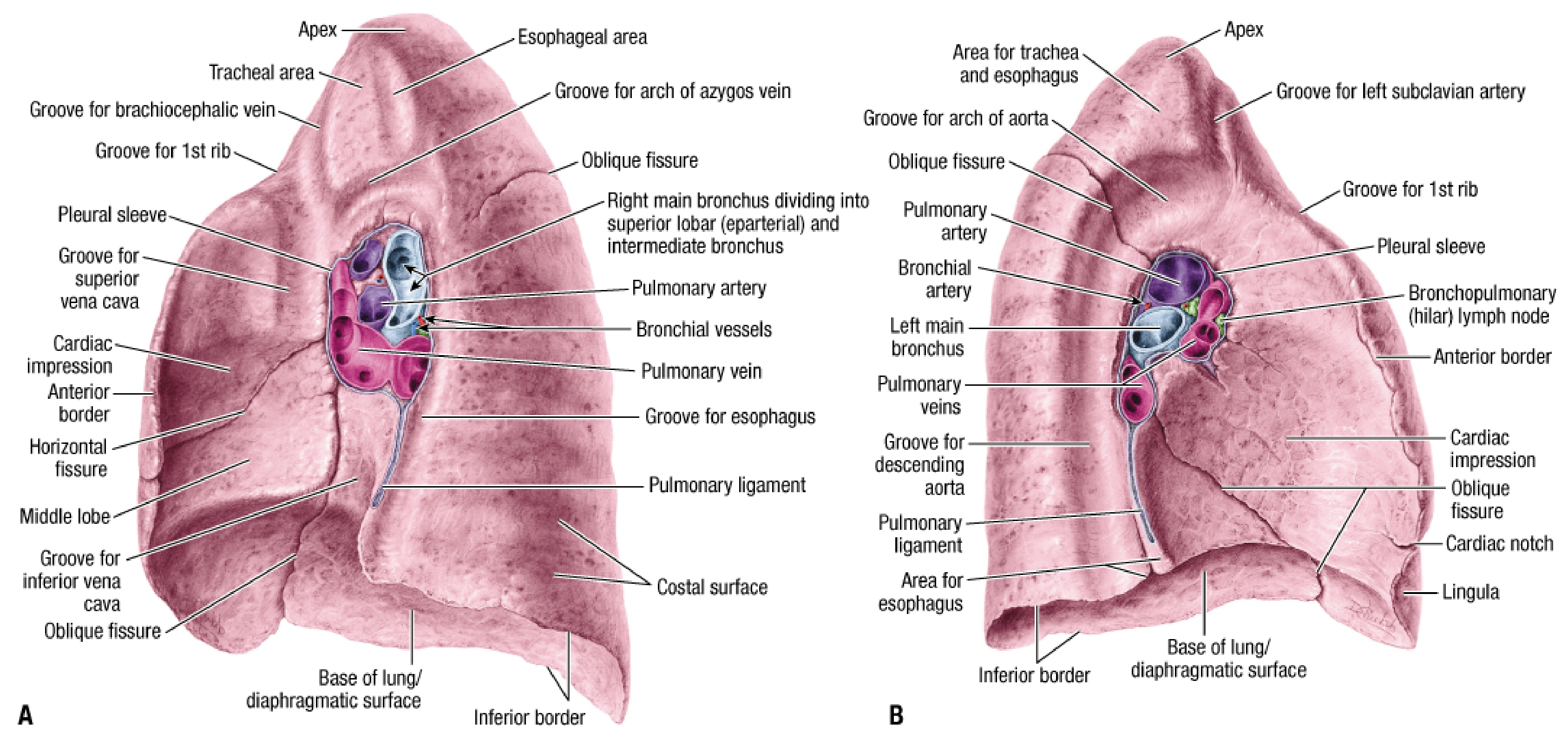
Right vs Left Hilum - Key Differences
| Feature | Right | Left |
|---|---|---|
| PA position | Passes anterior to bronchus | Arches superior to bronchus |
| Eparterial bronchus | Present (right upper lobe bronchus above PA) | Absent |
| Superior relation | Azygos vein arch | Aortic arch |
| Anterior relation | Superior vena cava | Phrenic nerve (on pericardium) |
| Posterior relation | Right vagus + esophagus | Left vagus + descending aorta |
| Main bronchus length | Shorter (~2.5 cm) | Longer (~5 cm) |
| PA length outside pericardium | Longer (more room to work surgically) | Shorter (less surgical room) |
| Visibility of posterior bronchial wall | Visible on CXR (outlined by air) | Usually not visible (left lower lobe artery intervenes) |
Surgical Significance
- The right PA is anterior to the bronchus - in right pneumonectomy/lobectomy the artery is encountered first at the anterior hilum after the veins are controlled.
- Azygos vein must be identified (and sometimes divided) to access the right upper lobe hilum superiorly. The right vagus lies between the azygos vein and the trachea - it can be damaged if the azygos is divided carelessly.
- Right phrenic nerve runs in the mediastinal adventitia of the SVC and pericardial sac - it is in a different tissue plane from the lung root and must not be included in lung retraction.
- Esophagus lies directly posterior to the hilum; the pulmonary ligament's mediastinal side is immediately anterior to the esophagus inferiorly.
- Eparterial bronchus means the right upper lobe bronchus is at risk during any hilar dissection at the superior aspect - it must be separately identified and preserved (or specifically targeted) during upper lobectomy.
- In the right upper lobe, the pulmonary vein is located most anterior to the pulmonary artery and bronchi at the hilum; the upper lobe vein arises from the same branch as the middle lobe vein (shared superior pulmonary vein trunk).
Sources: Fischer's Mastery of Surgery, 8th ed.; Scott-Brown's Otorhinolaryngology, Head & Neck Surgery; Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.