5.A 67-year-old man notices difficulty swallowing for 3 months: he says that it feels like food is getting stuck in the chest when swallowing. For one week, he has difficulty drinking water. He is losing weight without trying; his trousers have become loose and he has to tighten his belt by one extra hole. 1 What further signs and symptoms will you elicit? 2. What condition do you suspect? 3. How will you investigate the patient? 4. What treatment options are available if your initial clinical diagnosis is proven correct?
esophageal carcinoma dysphagia progressive weight loss clinical features symptoms signs
esophageal cancer investigation endoscopy biopsy staging CT scan treatment surgery radiotherapy chemotherapy
esophageal carcinoma endoscopy barium swallow imaging
Clinical Case: 67-year-old Man with Progressive Dysphagia and Weight Loss
2. Suspected Diagnosis
- Progressive dysphagia (initially solids, now liquids) — hallmark of mechanical obstruction
- Significant unintentional weight loss
- Older male patient
1. Further History and Signs to Elicit
Symptoms to Ask About
| System | Specific Questions |
|---|---|
| Dysphagia | Onset, progression (solids → liquids?), exact level of hold-up, complete obstruction? |
| Pain | Odynophagia (pain on swallowing), retrosternal/back pain (suggests local invasion) |
| Respiratory | Cough (especially after swallowing — tracheo-oesophageal fistula), hoarseness (left recurrent laryngeal nerve involvement), haemoptysis |
| GI | Haematemesis, melaena, regurgitation of undigested food |
| Systemic | Anorexia, fatigue, night sweats, quantify weight loss |
| Risk factors | Smoking, alcohol, GORD/Barrett's oesophagus, history of achalasia, caustic ingestion, previous head & neck cancer, diet (nitrosamines), geography |
Signs to Elicit on Examination
| Finding | Significance |
|---|---|
| Cervical/supraclavicular lymphadenopathy (esp. left Virchow's node) | Metastatic spread |
| Cachexia and muscle wasting | Advanced disease |
| Hepatomegaly | Liver metastases |
| Hoarseness | Left recurrent laryngeal nerve palsy (locally advanced) |
| Horner's syndrome | Sympathetic chain involvement |
| Signs of aspiration pneumonia | Tracheo-oesophageal fistula |
| Anaemia (pallor) | Chronic bleeding, nutritional deficiency |
| Bone tenderness | Bone metastases |
3. Investigations
First-line
| Investigation | Purpose |
|---|---|
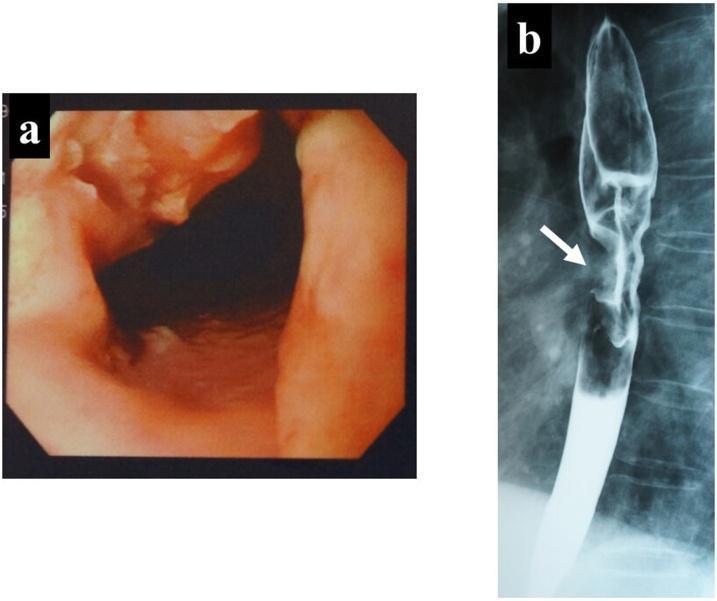
| Upper GI Endoscopy (OGD) + biopsy | Visualises tumour, defines site and extent, obtains histology — gold standard |
| Barium swallow | Characterises length and degree of stricture; shows classic "rat-tail" or "apple-core" narrowing |
| FBC, U&E, LFTs, albumin | Assess anaemia, nutritional status, liver function |
| Coagulation screen | Pre-operative and pre-procedure |
Staging Investigations
| Investigation | Purpose |
|---|---|
| CT chest/abdomen/pelvis (with contrast) | Assess local invasion, lymph node and distant metastases (liver, lung, adrenals) |
| PET-CT (FDG) | Detect occult distant metastases, superior to CT alone for staging |
| Endoscopic Ultrasound (EUS) | Best modality for T-staging (depth of invasion) and regional N-staging |
| Bronchoscopy | If mid/upper oesophageal lesion — exclude tracheo-bronchial invasion |
| Laparoscopy/staging laparotomy | For lower-third/GOJ tumours before planned surgery |
4. Treatment Options (if Oesophageal Carcinoma Confirmed)
Curative Intent
| Modality | Indication |
|---|---|
| Oesophagectomy (Ivor Lewis, McKeown, or transhiatal) | Resectable tumours (T1–T3, N0/N1, M0) in fit patients |
| Neoadjuvant chemoradiotherapy (CRT) → surgery | Locally advanced but resectable (T3/T4a, N+); CROSS trial regimen (carboplatin + paclitaxel + RT) is standard |
| Definitive chemoradiotherapy | Unresectable or cervical oesophageal tumours, or patients unfit for surgery; also curative in squamous cell carcinoma |
| Endoscopic mucosal resection (EMR) / ESD | Early-stage tumours (T1a/T1b), especially in the context of Barrett's oesophagus |
Palliative/Non-Surgical Options
| Modality | Purpose |
|---|---|
| Oesophageal stenting (SEMS) | Relieves dysphagia rapidly in unresectable disease |
| Palliative chemotherapy | Systemic disease — fluoropyrimidine + platinum ± trastuzumab (if HER2+) |
| Palliative radiotherapy | Dysphagia relief, haemostasis |
| Laser therapy / photodynamic therapy | Endoscopic palliation of luminal obstruction |
| Nutritional support (NG tube, PEG, TPN) | Maintain nutritional status pre/post-treatment |
| Immunotherapy (nivolumab, pembrolizumab) | Advanced/metastatic disease, particularly PD-L1 positive tumours |
Summary Algorithm
Confirm diagnosis (OGD + biopsy)
↓
Staging (CT + PET-CT + EUS)
↓
┌─────────────────┬──────────────────┐
Localised Locally advanced Metastatic/unfit
(T1–T2, N0) (T3/T4, N+)
↓ ↓ ↓
Surgery or EMR Neoadjuvant CRT Palliative stent,
(early stage) → surgery (if fit) chemo, RT, immunotherapy
OR definitive CRT
What’s the contraindications..
oesophagectomy contraindications unresectable esophageal cancer criteria
Contraindications to Oesophagectomy
Oncological Contraindications (Unresectable Disease)
| Finding | Reason |
|---|---|
| Distant metastases (liver, lung, peritoneum, bone) | M1 disease — surgery offers no survival benefit |
| Tracheo-bronchial invasion (T4b) | Cannot achieve clear resection margins |
| Aortic invasion | Technically unresectable |
| Involvement of the recurrent laryngeal nerve bilaterally | Unresectable locally advanced disease |
| Malignant tracheo-oesophageal fistula | Indicates invasion of the airway |
| Involvement of great vessels (aorta, vena cava) | T4b — unresectable |
| Malignant pleural or pericardial effusion | Systemic/metastatic spread |
| Bulky, fixed mediastinal lymph nodes | Suggests unresectable locoregional disease |
| Cervical oesophageal tumours | Technically very difficult; usually managed with definitive CRT instead |
Patient-Related (Fitness) Contraindications
| Category | Specific Contraindication |
|---|---|
| Cardiorespiratory | Severe COPD (FEV₁ < 1.0–1.2 L), recent MI, severe heart failure, uncontrolled arrhythmia |
| Pulmonary function | Poor predicted post-operative FEV₁ or diffusion capacity |
| Nutritional/metabolic | Severe malnutrition, cachexia (relative — may be optimised pre-operatively) |
| Performance status | WHO/ECOG PS ≥ 3 — unable to tolerate major surgery |
| Liver disease | Cirrhosis / significant hepatic dysfunction |
| Renal failure | Significant CKD increases peri-operative mortality |
| Age alone | NOT an absolute contraindication, but combined with comorbidities increases risk |
| Previous thoracic surgery | Dense adhesions may make oesophagectomy technically hazardous |
Contraindications Specific to Neoadjuvant Chemoradiotherapy
| Contraindication | Reason |
|---|---|
| Poor performance status (ECOG ≥ 3) | Cannot tolerate toxicity of combined modality treatment |
| Severe renal impairment | Limits platinum-based chemotherapy use |
| Prior thoracic/mediastinal radiation | Risk of cumulative toxicity |
| Active severe infection or sepsis | Must be treated first |
Practical Summary
- Resectable tumour (T1–T3, no T4b, no M1) — AND
- Adequate cardiopulmonary reserve (able to lose ~25% lung function post-operatively and survive a 4–8 hour operation)
Management Curable Surgery (esophagectomy) o 3 methods i. Modified Ivor Lewis ii. Mckeown (3 field esophagectomy) iii. Transhiatal esophagectomy o Contraindication for surgery i. Metastasize N2 (celiac, cervical or supraclavicular LN) or solid organs ii. Invasion of adjacent structure (RLN, tracheobronchial tree, aorta, pericardium) iii. Severe associated comorbid (CVS/RS diseases) Adjuvant therapy- chemo or radiotherapy Incurable Palliative care (chemo or radiotherapy) Stenting Laser recanalisation Comparatively to this management, is this sufficient or do I have to add anything from yours. Also explain the treatments to me as I don’t understand
Ivor Lewis McKeown transhiatal esophagectomy technique approach comparison
neoadjuvant chemoradiotherapy esophageal cancer CROSS trial adjuvant therapy palliative stenting laser
Assessment of Your Management Plan
What to Add
- Neoadjuvant therapy (given before surgery) — this is now standard of care for locally advanced resectable disease, not just adjuvant (after surgery)
- Definitive chemoradiotherapy — for patients with resectable disease who are unfit for surgery, or cervical oesophageal tumours; can be curative on its own
- Endoscopic resection (EMR/ESD) — for very early stage (T1a) tumours only
- Nutritional support (nasogastric feeding, PEG tube)
- Best supportive care / hospice
Explanations of Each Treatment
CURABLE TREATMENTS
1. The Three Surgical Methods (Oesophagectomy)
| Incisions | Abdomen + right chest (2 cuts) |
| What happens | Stomach mobilised from below → oesophagus removed from the right chest → stomach pulled up → joined in the chest |
| Anastomosis (join) | In the chest (intrathoracic) |
| Best for | Middle and lower third oesophageal tumours |
| Advantage | Good access to mid-oesophagus and chest lymph nodes |
| Disadvantage | If the join leaks, it leaks into the chest — serious complication |
| Incisions | Abdomen + right chest + neck (3 cuts) |
| What happens | Same as Ivor Lewis but the join is made in the neck instead of the chest |
| Anastomosis (join) | In the neck (cervical) |
| Best for | Upper and middle third tumours, or when you need a very wide clearance |
| Advantage | If the neck join leaks, it's easier to manage (just opens up at the skin) — less dangerous than a chest leak |
| Disadvantage | Longer operation, higher risk of recurrent laryngeal nerve injury (hoarse voice) |
| Incisions | Abdomen + neck only — no chest incision |
| What happens | Surgeon reaches up through the diaphragm hiatus (the hole where the oesophagus passes through) and down through the neck to blindly dissect and remove the oesophagus without opening the chest |
| Anastomosis (join) | In the neck |
| Best for | Lower third tumours, patients who cannot tolerate opening the chest (poor lung function) |
| Advantage | Avoids thoracotomy — better tolerated by frail patients |
| Disadvantage | Limited visibility — cannot do a thorough lymph node dissection in the chest; not suitable for tumours invading chest structures |
Imagine the oesophagus is a blocked water pipe running from the basement (abdomen) through the walls (chest) to the top floor (neck). Ivor Lewis opens the basement and the wall. McKeown opens the basement, the wall, and the top floor. Transhiatal opens only the basement and top floor, reaching through without opening the wall.
2. Neoadjuvant Therapy (given BEFORE surgery)
- Shrink the tumour to make surgery easier and more likely to achieve clear margins
- Kill any microscopic spread early
- In some patients, the tumour completely disappears (pathological complete response) — these patients have the best outcomes
3. Adjuvant Therapy (given AFTER surgery)
4. Definitive Chemoradiotherapy (no surgery)
PALLIATIVE TREATMENTS (Incurable Disease)
5. Oesophageal Stenting (SEMS — Self-Expanding Metal Stent)
6. Palliative Chemotherapy
7. Palliative Radiotherapy
8. Laser Recanalisation
9. Nutritional Support
- Nasogastric (NG) tube — fine tube through the nose into the stomach
- PEG tube (Percutaneous Endoscopic Gastrostomy) — tube placed directly into the stomach through the skin
- Total parenteral nutrition (TPN) — feeding directly into a vein, bypassing the gut entirely
Revised Complete Management Framework
CONFIRMED OESOPHAGEAL CARCINOMA
│
┌──────┴──────┐
CURABLE INCURABLE
(no metastases, (M1, T4b, or
resectable) unfit)
│ │
FIT for surgery? Palliative:
├── YES → • Stenting
│ Neoadjuvant • Chemo/RT
│ CRT → Surgery • Laser
│ (Ivor Lewis / • Nutrition
│ McKeown / • Supportive
│ Transhiatal) care
│ ± Adjuvant CRT
│
└── NO (poor fitness,
cervical tumour) →
Definitive CRT
(curative intent)
4. What treatment options are available if your initial clinical diagnosis is proven correct? -Curable A) Surgery (esophagectomy) *3 methods(suitable for early lesion & physically fit patients) i. Modified Ivor Lewis ii. Mckeown (3 field esophagectomy) iii. Transhiatal esophagectomy *Contraindication for surgery i. Metastasize N2 (celiac, cervical or supraclavicular LN) or solid organs ii. Invasion of adjacent structure (RLN, tracheobronchial tree, aorta, pericardium) iii. Severe associated comorbid (Cardiovascular or Respiratory diseases) B) Adjuvant therapy- chemo or radiotherapy -Incurable Palliative Treatment of Advanced Inoperable Carcinoma of Oesophagus • Intubation with Souttar tube or Celestin tube • Expandable metal stents • Endoscopic laser • Endoscopic bipolar diathermy ◦ Endoscopic argon-beam plasma coagulationm Is this answer okay for question 4
What You Have — Assessment
| Section | Verdict |
|---|---|
| 3 surgical methods | ✅ Correct |
| Contraindications | ✅ Correct |
| Adjuvant therapy | ✅ Correct but incomplete (see below) |
| Palliative intubation/stenting | ✅ Good — Souttar/Celestin tubes are older but valid to mention |
| Laser + diathermy + argon plasma | ✅ Good additions |
What to Add or Improve
Under Curable — Section B (Adjuvant Therapy)
- Neoadjuvant therapy — given before surgery to shrink the tumour (this is now standard of care and arguably more important than adjuvant)
- Adjuvant therapy — given after surgery to eliminate residual disease
B) Neoadjuvant + Adjuvant Chemo/Radiotherapy
- Neoadjuvant CRT (chemo + radiotherapy given before surgery) — shrinks tumour, improves resectability, standard for locally advanced disease
- Adjuvant CRT (after surgery) — for high-risk histological findings post-operatively
Under Curable — Add Section C
- Definitive Chemoradiotherapy (no surgery) — for patients who are unfit for surgery or have cervical oesophageal tumours; given with curative intent, not just palliative
Under Palliative — Add These
- Palliative chemotherapy (systemic — slows disease progression)
- Palliative radiotherapy (shrinks tumour, relieves dysphagia/bleeding)
- Nutritional support — NG tube, PEG tube, or TPN (very important in practice)
- Best supportive care / hospice
Your Revised Complete Answer 4
- Modified Ivor Lewis
- McKeown (3-field oesophagectomy)
- Transhiatal oesophagectomy
- Metastasis to N2 nodes (coeliac, cervical, supraclavicular) or solid organs
- Invasion of adjacent structures (RLN, tracheobronchial tree, aorta, pericardium)
- Severe cardiovascular or respiratory comorbidities
- Shrinks tumour and improves surgical outcomes
- Standard for locally advanced resectable disease
- For high-risk features on post-operative pathology
- For patients unfit for surgery or cervical oesophageal tumours
- Intubation with Souttar tube or Celestin tube
- Expandable metal stents (SEMS)
- Endoscopic laser recanalisation
- Endoscopic bipolar diathermy
- Endoscopic argon-beam plasma coagulation
- Palliative chemotherapy
- Palliative radiotherapy
- Nutritional support (NG tube / PEG tube / TPN)
- Best supportive care