Hypersensitivity type 1
Reading File
search_medical_text
type 1 hypersensitivity IgE mediated anaphylaxis mechanism pathophysiology
search_medical_text
type 1 hypersensitivity clinical features diagnosis management treatment
search_medical_image
type 1 hypersensitivity IgE mast cell degranulation mechanism diagram
GradeResponse
GradeResponse
GradeResponse
Type I Hypersensitivity (Immediate / IgE-Mediated)
Overview
Type I hypersensitivity is an immediate, IgE-mediated immune reaction that occurs within minutes of re-exposure to an allergen in a previously sensitized individual. It underlies conditions like anaphylaxis, allergic asthma, allergic rhinitis, urticaria, and atopic dermatitis.
Mechanism & Pathophysiology
Two-Phase Process
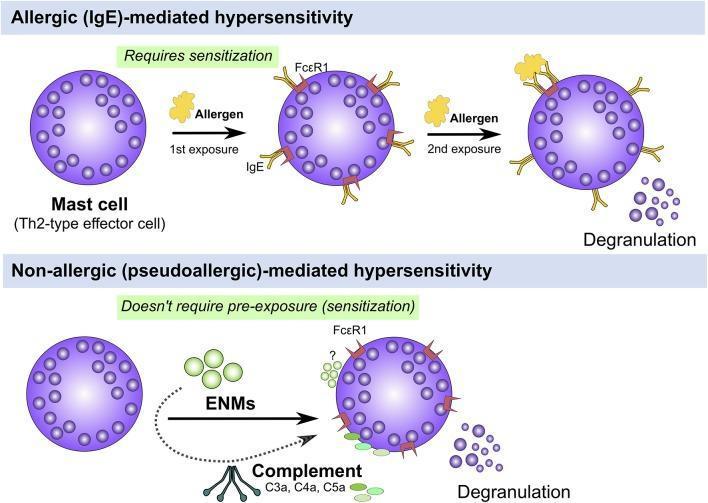
Phase 1 — Sensitization (First Exposure)
- Antigen (allergen) is processed by antigen-presenting cells (APCs).
- Th2 cells are activated → secrete IL-4, IL-5, IL-6, IL-10, IL-13.
- A specialized subset, Tfh13 cells, produce IL-4, IL-5, and IL-13, driving allergen-specific IgE production by B cells.
- IgE antibodies bind to high-affinity FcεRI receptors on mast cells (tissue) and basophils (blood) → cell becomes "armed."
(Harrison's, p. 9830)
Phase 2 — Re-Exposure (Elicitation)
- Allergen cross-links two adjacent IgE–FcεRI complexes on the mast cell surface → degranulation.
- Pre-formed and newly synthesized mediators are released.
Mediators Released
Mast cell/basophil mediators fall into three categories:
| Category | Mediators | Effects |
|---|---|---|
| Preformed (granule) | Histamine, tryptase, heparin, TNF-α | Vasodilation, ↑ vascular permeability, bronchoconstriction, pruritus |
| Lipid-derived (newly synthesized) | Prostaglandins (PGD₂), Leukotrienes (LTC₄, LTD₄, LTE₄), PAF | Sustained bronchoconstriction, mucus secretion, chemotaxis |
| Cytokines | IL-4, IL-5, IL-13, TNF-α | Eosinophil recruitment, perpetuation of Th2 response |
Phases of the Allergic Response
| Phase | Timing | Mediators | Features |
|---|---|---|---|
| Early (immediate) | Minutes (0–30 min) | Histamine, tryptase | Wheal-and-flare, bronchospasm, pruritus |
| Late | 4–12 hours later | Leukotrienes, cytokines, eosinophils | Sustained inflammation, tissue damage |
Clinical Manifestations
Severity ranges from local to systemic:
| Condition | Features |
|---|---|
| Anaphylaxis | Multisystem: urticaria, angioedema, bronchospasm, hypotension, cardiovascular collapse |
| Allergic asthma | Reversible bronchoconstriction, wheeze, dyspnea |
| Allergic rhinitis | Sneezing, rhinorrhea, nasal congestion, pruritus |
| Urticaria / Angioedema | Raised itchy wheals; deeper tissue swelling |
| Atopic dermatitis | Chronic eczematous inflammation |
| Allergic conjunctivitis | Tearing, conjunctival injection, itching |
| Food allergy | GI cramping, vomiting, systemic reactions |
Diagnosis
- Skin prick test (SPT): allergen introduced intradermally → wheal-and-flare within 15–20 min confirms sensitization.
- Serum specific IgE (ImmunoCAP/RAST): measures allergen-specific IgE levels.
- Serum total IgE: elevated in atopic individuals (less specific).
- Serum tryptase: elevated after anaphylaxis; confirms mast cell activation.
- Basophil activation test (BAT): flow cytometry-based; useful when SPT/specific IgE are inconclusive.
Management
1. Acute (Anaphylaxis)
- Epinephrine IM (0.3–0.5 mg, 1:1000) — first-line; given into the anterolateral thigh.
- IV fluids for hypotension.
- H1 antihistamines (diphenhydramine) + H2 blockers — adjunctive only.
- Corticosteroids (methylprednisolone) — adjunctive; prevent late-phase reaction.
- Bronchodilators (salbutamol) for bronchospasm.
- Patient should carry an auto-injector (EpiPen) after discharge.
2. Chronic / Prevention
| Strategy | Examples |
|---|---|
| Allergen avoidance | Identify and eliminate triggers |
| H1 antihistamines | Cetirizine, loratadine, fexofenadine (2nd gen preferred) |
| Intranasal corticosteroids | Fluticasone, mometasone (allergic rhinitis) |
| Inhaled corticosteroids + LABA | Asthma control |
| Leukotriene receptor antagonists | Montelukast |
| Allergen immunotherapy (AIT) | Subcutaneous (SCIT) or sublingual (SLIT) — modifies disease course by shifting Th2 → Th1/Treg response |
| Biologics | Omalizumab (anti-IgE); dupilumab (anti-IL-4Rα) for severe asthma/atopic dermatitis |
Key Comparison: Gell & Coombs Classification
| Type | Mechanism | Timing | Example |
|---|---|---|---|
| I | IgE, mast cells, basophils | Minutes | Anaphylaxis, asthma |
| II | IgG/IgM + complement | Hours | Hemolytic transfusion reaction |
| III | Immune complexes | 6–12 h | Serum sickness, SLE |
| IV | T-cell mediated (delayed) | 48–72 h | Contact dermatitis, TB skin test |
Summary: Type I hypersensitivity is a rapid, IgE-mediated reaction where allergen cross-linking of mast cell-bound IgE triggers degranulation and release of vasoactive, bronchospastic, and chemotactic mediators. Clinically it spans from mild local reactions to life-threatening anaphylaxis, with epinephrine as the cornerstone of acute treatment and immunotherapy as the only disease-modifying option. (Harrison's Principles of Internal Medicine, 21st Ed., p. 9830)
This is a shared conversation. Sign in to Orris to start your own chat.