Equipment for emergency cricothyrotomy - types, indications, limitations References - millers, Morgan, barash, baheti, dnb kaushik, all anaesthesia standard textbooks and all emergency medicine standard textbooks Guve as 10 marks question add necessary flowcharts and diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from all major textbooks. Let me compile the full 10-marks answer.
Equipment for Emergency Cricothyrotomy: Types, Indications, and Limitations
[10-Marks Answer - Anaesthesia / Emergency Medicine]
ANATOMY OF THE CRICOTHYROID MEMBRANE (CTM)
The CTM is a fibroelastic membrane located anteriorly in the midline of the neck, bordered superiorly by the thyroid cartilage and inferiorly by the cricoid cartilage. Its central triangular portion is subcutaneous, making it the ideal site for emergency airway access.
Dimensions: ~9 mm longitudinally × 30 mm transversely in an average adult.
Surface landmark: Located approximately one-third of the distance from the manubrium to the chin; roughly 2-3 cm below the laryngeal prominence (Adam's apple).
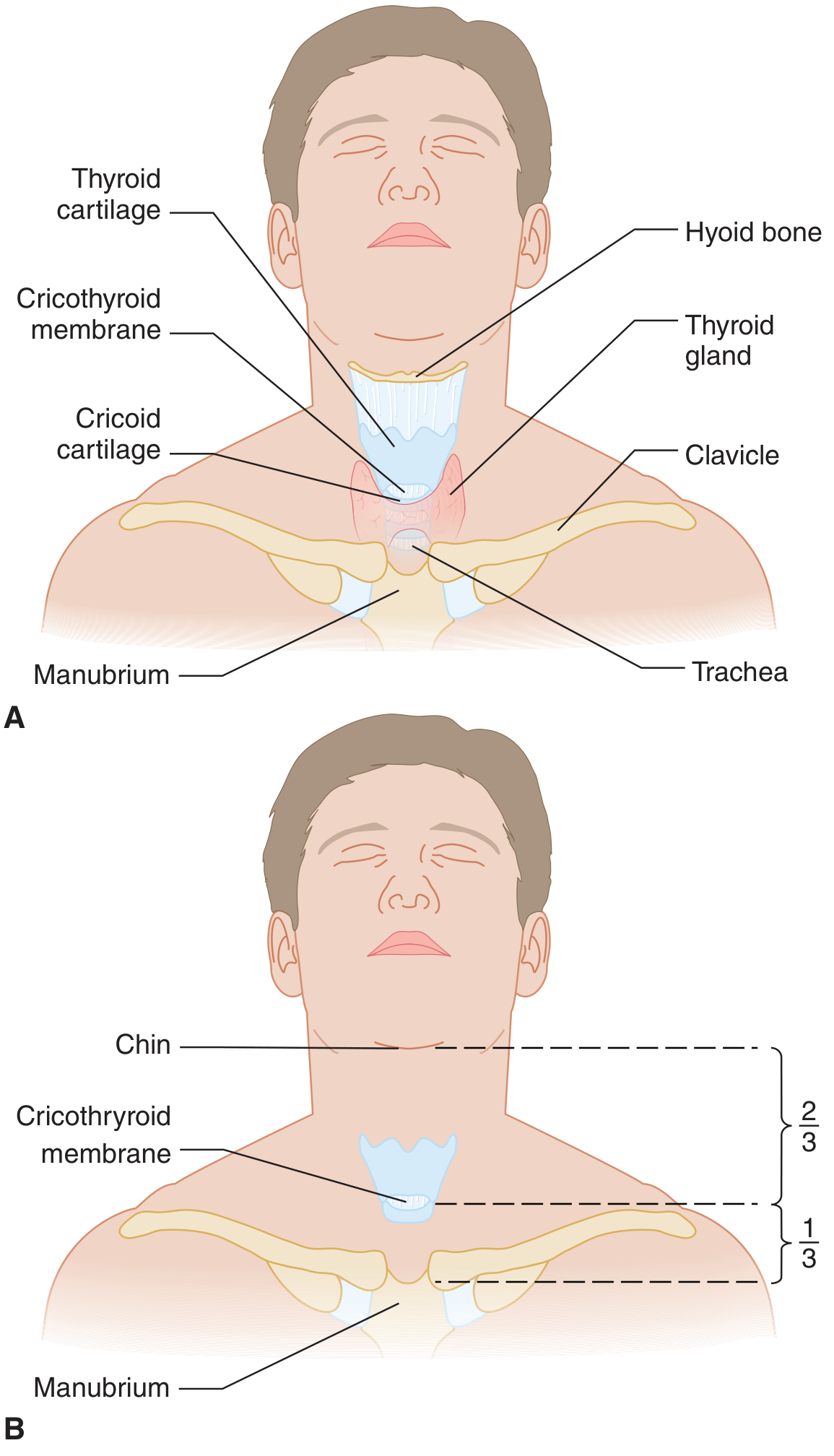
Figure: Anatomy of the neck (A) and location of the cricothyroid membrane at approximately one-third the distance from manubrium to chin (B). [Tintinalli's Emergency Medicine]
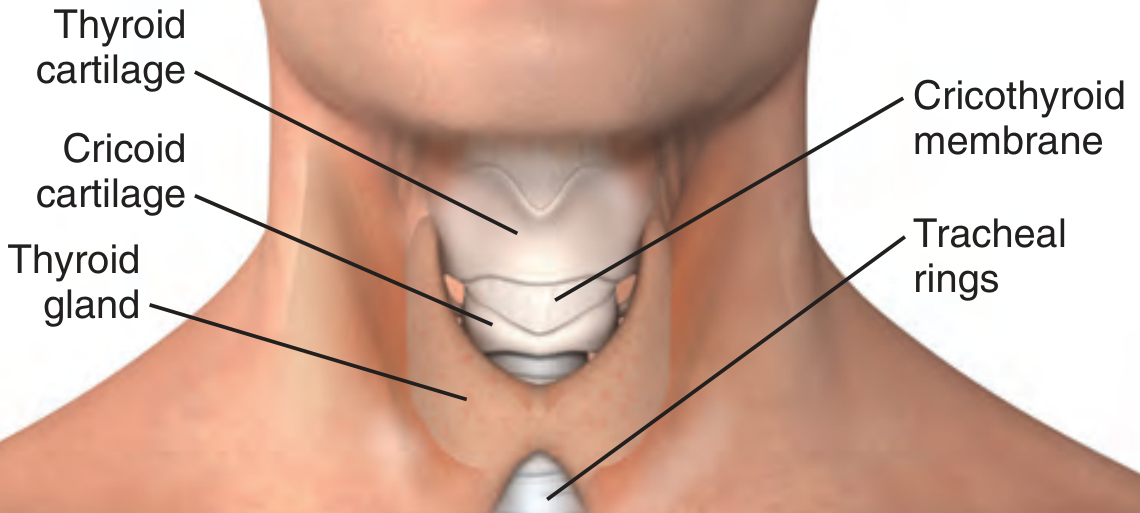
Figure: Normal adult larynx - position and configuration of the cricothyroid membrane. [Roberts and Hedges']
DEFINITION AND TERMINOLOGY
Cricothyrotomy, cricothyroidotomy, coniotomy, and minitracheostomy are synonyms for establishing an air passage through the CTM. It differs from tracheostomy in that the incision is made through the CTM (between thyroid and cricoid cartilages), NOT between tracheal rings.
- Barash Clinical Anesthesia, 9e - Cricothyrotomy, p. 2405
- Miller's Anesthesia, 10e - p. 5958
INDICATIONS
Primary Indication - CICO (Cannot Intubate, Cannot Oxygenate)
The primary and most critical indication is the CICO scenario - a life-threatening situation where:
- Conventional orotracheal/nasotracheal intubation has failed
- Oxygenation cannot be maintained (SpO₂ cannot be maintained >90% between intubation attempts or after three attempts)
- Bag-valve-mask ventilation has failed
Specific Indications (Roberts & Hedges; Tintinalli's; Rosen's):
| Category | Details |
|---|---|
| Failed airway | SpO₂ <90% despite BVM between attempts or after ≥3 intubation attempts |
| Failed BVM | Unable to ventilate with bag-valve-mask between attempts |
| Failed rescue devices | Failure of LMA, gum elastic bougie-guided intubation |
| Anticipated impossible intubation | Severe maxillofacial trauma, oropharyngeal hemorrhage, massive swelling/foreign body obstructing visualisation |
| Cervical spine injury | When head/neck movement is absolutely contraindicated |
| Anatomical distortion | Burns, angioedema, tumours, hematoma |
| Obstructing laryngeal pathology | Supraglottic obstruction (epiglottitis, angioedema) |
| Elective use | Severe cervical kyphoscoliosis with limited tracheal access |
"If standard intubation seems unlikely to succeed, it is not always necessary to attempt it prior to establishing a surgical airway." - Tintinalli's Emergency Medicine
CONTRAINDICATIONS
Absolute:
- Age < 5-12 years (depending on source - the cricoid is the narrowest part in children; surgical cricothyrotomy is contraindicated; needle cricothyrotomy with TTJV is preferred)
- Laryngeal fracture
- Tracheal transection or obstruction below the CTM
- Complete airway obstruction (for jet ventilation - expiration is blocked)
- Laryngeal neoplasm or subglottic stenosis
Relative:
- Coagulopathy
- Distorted or unidentifiable neck anatomy (obesity, haematoma, prior surgery)
- Local infection at puncture site
- Operator unfamiliarity
- Miller's Anesthesia 10e, p. 5958; Barash 9e, p. 2405
TYPES OF EMERGENCY CRICOTHYROTOMY & EQUIPMENT
There are three main techniques, each with distinct equipment requirements:
┌─────────────────────────────────────────────────────────────┐
│ EMERGENCY CRICOTHYROTOMY │
│ │ │
│ ┌───────────────┼───────────────┐ │
│ ▼ ▼ ▼ │
│ NEEDLE/CANNULA SURGICAL (Open) PERCUTANEOUS │
│ CRICOTHYROTOMY CRICOTHYROTOMY DILATIONAL │
│ + PTLV/TTJV (Seldinger) │
└─────────────────────────────────────────────────────────────┘
TYPE 1: NEEDLE CRICOTHYROTOMY (with Percutaneous Translaryngeal Ventilation / TTJV)
Synonyms: Needle cricothyrotomy, PTLV (Percutaneous Translaryngeal Ventilation), Transtracheal Jet Ventilation (TTJV)
Equipment Required:
| Item | Specification |
|---|---|
| Cannula/catheter | 12-16 gauge over-the-needle catheter (IV catheter); kink-resistant commercial catheter preferred (e.g., Cook Transtracheal Airway Catheter, Ravussin Translaryngeal Catheter) |
| Syringe | 3-5 mL Luer lock syringe (fluid-filled with saline for air-contrast technique) |
| ETT adapter (makeshift) | 7.0 ETT adapter + 3 mL syringe barrel connecting catheter to BVM (field improvisation) |
| High-pressure O₂ source | 35-50 psi (wall O₂ or E-cylinder before standard regulators; standard wall O₂ flowmeters are insufficient) |
| Jet ventilator | Commercial: VBM Manujet III, Meditech Rapid-02, Cook ENK Oxygen Flow Modulator |
| Low-compliance tubing | Dedicated high-pressure tubing with secure Luer lock connections (NOT standard IV tubing or corrugated anaesthesia tubing) |
"Do not try to use standard oxygen tubing, three-way stopcocks, or bag-valve devices or attach to wall outlets turned to highest liter flow." - Tintinalli's, p. 240
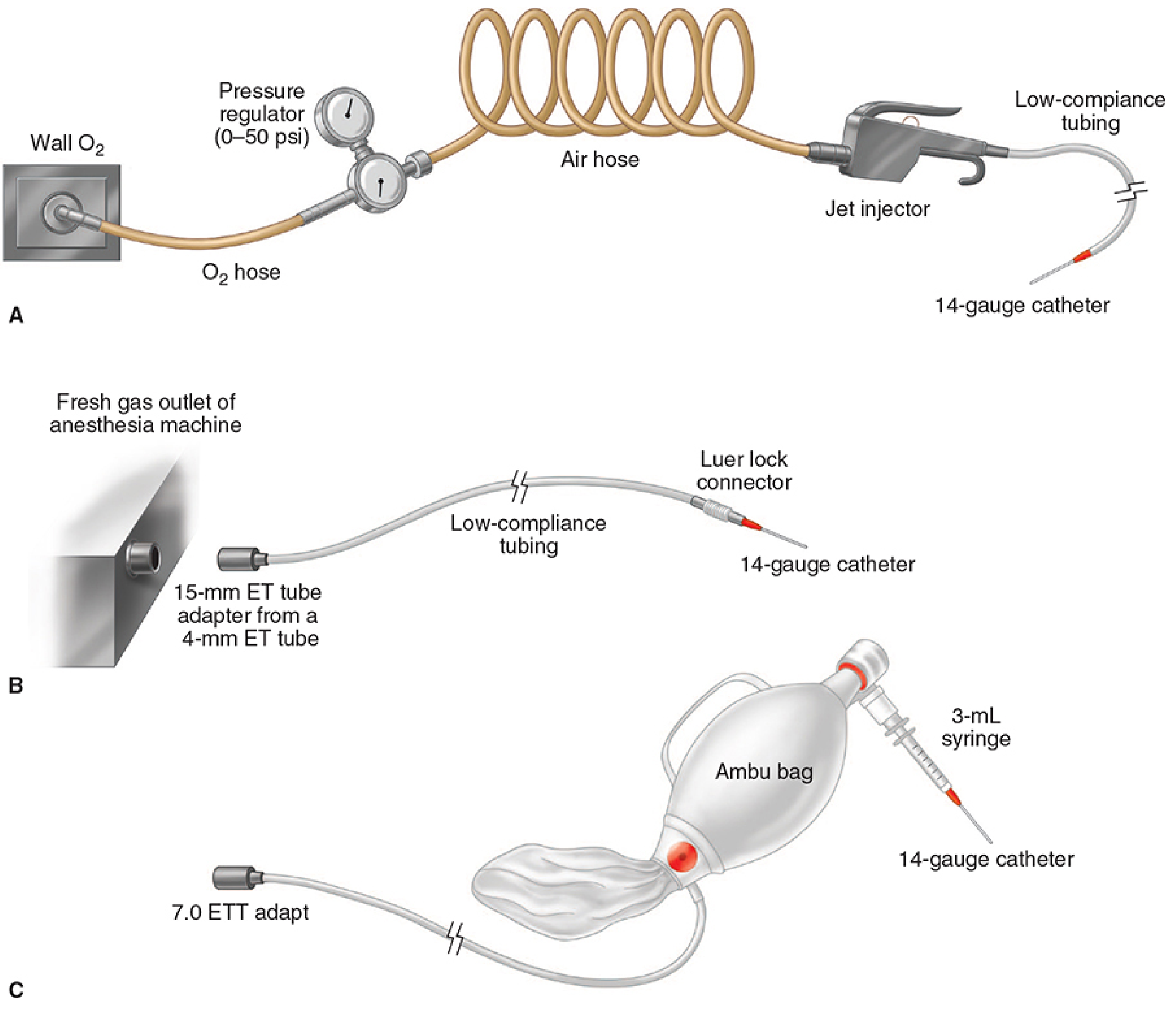
Figure: Three systems for transtracheal jet ventilation (A: jet ventilator + pressure regulator; B: fresh gas outlet of anesthesia machine; C: improvised ETT adapter + Ambu bag). [Morgan & Mikhail's Clinical Anesthesiology, 7e]
Technique Summary (Tintinalli's):
- Extend neck; identify CTM
- Stabilize thyroid cartilage with non-dominant hand
- Attach 3 mL syringe to catheter; insert at 45° caudally through CTM
- Aspirate air to confirm tracheal entry
- Advance catheter to hub; remove needle
- Connect jet ventilator; I:E ratio 1:4; max 1 second inspiration
- Monitor chest rise; auscultate bilateral breath sounds
TYPE 2: SURGICAL CRICOTHYROTOMY (Open / Standard Technique)
Equipment Required (Tintinalli's - Table 30-3; Roberts & Hedges; Miller's Box 40.4):
| Item | Specification |
|---|---|
| Scalpel | No. 10 blade (preferred for width) or No. 11 blade |
| ETT or tracheostomy tube | Cuffed ETT 6.0 mm ID (preferred in adults; max 7 mm - larger tubes increase risk of subglottic stenosis); OR Shiley tracheostomy tube No. 4 (ID 5.0 mm) or No. 6 (ID 6.4 mm) |
| Trousseau dilator | For stoma dilation (traditional technique) |
| Tracheal hook | Single hook (traditional) OR Bair Claw (double hook - reduces cricoid ring fractures) |
| Gum elastic bougie | With coudé (angled) tip - for tube guidance (Seldinger-style tube passage) |
| Bag-valve-mask device | With oxygen source for ventilation |
| Suction | For blood/secretions clearance |
| Securing material | Tape, cloth ribbon/ties, sutures |
| PPE | Gloves, eye protection |
| Local anaesthetic | Lignocaine with adrenaline (if patient awake and time permits) |
Sub-techniques of surgical cricothyrotomy:
- Traditional 5-step technique: Incise skin → identify CTM → stab/incise CTM horizontally → dilate with Trousseau dilator → insert tube
- Rapid Four-Step Technique (RFST / Brantigan-Grow): Palpate → horizontal stab incision through skin AND CTM → caudal traction with tracheal hook → insert tube (omits dilator; faster but slightly higher complication rate in some studies)
- Bair Claw modification: Replaces single hook with double-hook device; reduces cricoid ring fractures; operator positioned at head of bed
Surgical Cricothyrotomy Technique (Miller's Box 40.4):
- Stand on patient's left (if right-handed)
- Stabilize larynx with left hand
- Left index finger identifies CTM (if not palpable, 8-10 cm vertical midline incision + blunt dissection)
- Transverse stab incision through skin and CTM with right hand, blade edge toward you
- Keep scalpel perpendicular; rotate 90° so cutting edge points caudally
- Swap hands; left hand maintains gentle lateral traction on scalpel (keeping handle vertical)
- Insert bougie caudally beside scalpel blade
- Remove scalpel; railroad 6 mm cuffed ETT over bougie; inflate cuff; ventilate
- Confirm placement (capnography, bilateral breath sounds)
TYPE 3: PERCUTANEOUS DILATIONAL CRICOTHYROTOMY (Seldinger Technique)
Commercial kit example: Melker Cricothyrotomy Kit (Cook Critical Care)
Equipment in Melker Kit (Roberts & Hedges):
| Item | Specification |
|---|---|
| Syringe | 6 mL |
| Introducer needle | 18-gauge with overlying TFE (tetrafluoroethylene) catheter |
| Guidewire (J-tip) | Flexible, for safe passage into trachea |
| Tapered dilator | For tract dilation over guidewire |
| Melker airway catheter | Cuffed; placed over dilator/guidewire as a unit; replaces tracheostomy tube |
| No. 15 scalpel | Small skin incision at guidewire entry point |
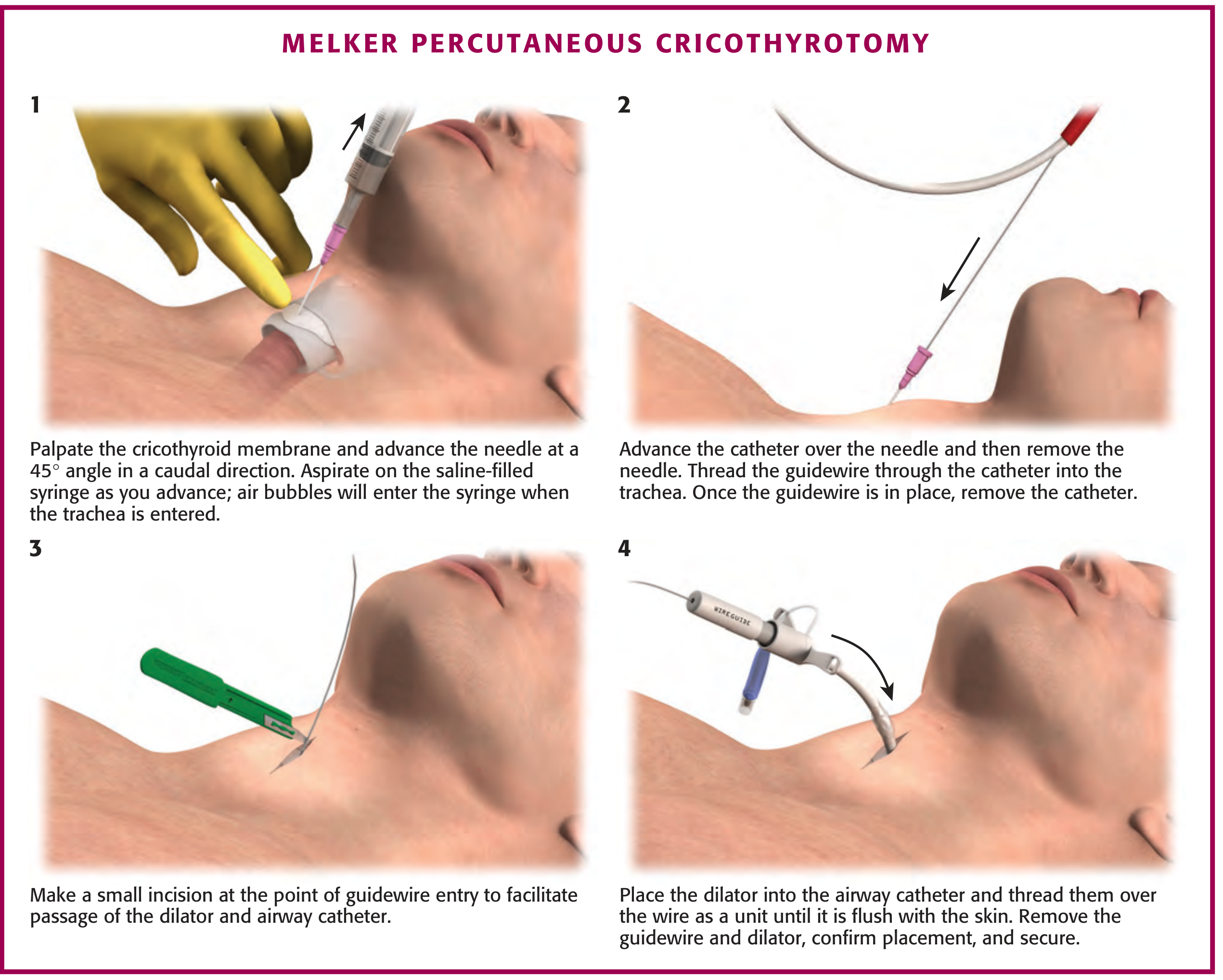
Figure: Melker percutaneous cricothyrotomy - 4-step Seldinger technique. Step 1: Needle insertion at 45° with saline aspiration. Step 2: Thread guidewire. Step 3: Skin incision at entry point. Step 4: Dilator + airway catheter threaded over wire as unit. [Roberts and Hedges']
Technique:
- Identify CTM; insert 18G needle with syringe at 45° caudally; aspirate air/saline bubbles confirm entry
- Advance TFE catheter; remove needle; insert guidewire through catheter; remove catheter
- Small skin incision at guidewire entry
- Thread dilator + Melker catheter together over wire → advance flush with skin → remove guidewire and dilator
- Inflate cuff; confirm placement; ventilate
COMPARISON OF TECHNIQUES
| Feature | Needle/PTLV | Surgical (Open) | Percutaneous Seldinger |
|---|---|---|---|
| Speed | Fastest | Fast (RFST: ~40 sec) | Slower (2-3 min) |
| Skill required | Low-moderate | Moderate | Moderate |
| Ventilation quality | Oxygenation only (30-45 min) | Full ventilation | Full ventilation |
| CO₂ clearance | Poor (hypercapnia accumulates) | Adequate | Adequate |
| Equipment needed | Minimal (can improvise) | Surgical tray | Commercial kit |
| Success rate (anesthesia provider) | ~50% | 90-100% (surgeon) | Moderate |
| Use in children | YES (preferred <10-12 yrs) | NO (<5-12 yrs) | NO (<5-12 yrs) |
| Definitive airway | No (bridge only) | Yes (temporary) | Yes (temporary) |
| Risk of kinking | High (especially IV catheters) | None | Low |
- Miller's Anesthesia 10e, p. 5958; Barash 9e, p. 2405
LIMITATIONS OF EACH TECHNIQUE
Needle Cricothyrotomy Limitations:
- Not a definitive airway - bridge only; CO₂ accumulates rapidly (safe for ~30-45 minutes only)
- Kinking of catheter - standard IV catheters kink easily; dedicated kink-resistant catheters (Cook, Ravussin) are mandatory
- High-pressure source mandatory - BVM and standard wall O₂ flowmeters are inadequate; if proper jet ventilator is unavailable, ventilation is ineffective
- Barotrauma risk - pneumothorax, massive subcutaneous emphysema, mediastinal emphysema if catheter misplaced or ventilation excessive
- Requires patent upper airway for exhalation - passive exhalation must occur via glottis; complete upper airway obstruction is the only absolute contraindication
- Small catheter lumen - limits gas flow; 16G or larger preferred (13G commercial catheters ideal)
- Catheter displacement - requires constant manual stabilization; easily dislodged
Surgical Cricothyrotomy Limitations:
- Contraindicated in children <5-12 years - funnel-shaped compliant pediatric larynx; cricoid is narrowest point; thyroid isthmus overlies CTM
- Subglottic stenosis - historically feared; now known to be infrequent; risk increased with prolonged cannulation, old age, diabetes, concurrent laryngeal pathology
- Requires identifiable CTM - obesity, haematoma, prior surgery may obscure landmarks
- Not a permanent airway - must be converted to formal tracheostomy (ideally within 72 hours) or removed
- Vocal cord/laryngeal injury - if blade passes too deeply or cephalad
- Bleeding - thyroidea ima artery (midline branch of aorta), cricothyroid vessels laterally
- Tube malposition - mainstem bronchial intubation, tube impinging on vocal cords
- Cricoid ring fracture - reported with single-hook RFST; reduced with Bair Claw
Percutaneous Seldinger Limitations:
- Requires easily identifiable CTM - anatomical distortion makes needle localisation difficult (unlike surgical technique where skin incision first exposes anatomy)
- Guidewire complications - wire may pass in wrong direction or kink
- Slower than surgical technique - multiple steps; less suited to extreme emergencies
- Less reliable in soiled/bloody fields - guidewire placement less reliable with active hemorrhage
- Smaller airway catheter - compared to standard ETT, may limit suctioning
COMPLICATIONS
Acute Complications (More Common):
- Tube malposition / failed placement
- Hemorrhage (thyroidea ima, cricothyroid vessels)
- Mainstem bronchial intubation
- Laryngotracheal injury
- Subcutaneous emphysema
- Tension pneumothorax (rare)
Acute Complications (Less Common):
- Esophageal puncture
- Aspiration
- Retrograde pharyngeal intubation
Late Complications:
- Subglottic / glottic stenosis (infrequent; risk factors: prolonged cannulation, DM, old age, laryngeal pathology)
- Voice change (most common reported long-term complaint)
- Difficulty swallowing
- Wound infection
- Tracheomalacia (especially with TTJV)
- Vocal cord changes
"Chevalier Jackson's 1921 concern about subglottic stenosis was refuted by Brantigan and Grow (1976) who reported only 6.1% overall complication rate with no chronic subglottic stenosis." - Roberts & Hedges', p. 193
FAILED AIRWAY ALGORITHM - CICO PATHWAY
FAILED INTUBATION
│
▼
Can you oxygenate with BVM / SGA?
│
YES │ NO (CICO)
│ │
│ ▼
│ ┌─────────────────────────────────────┐
│ │ FRONT OF NECK ACCESS (FONA) │
│ │ │
│ │ Age ≥ 10-12 years? │
│ │ │ │ │
│ │ YES NO │
│ │ │ │ │
│ │ ▼ ▼ │
│ │ SURGICAL NEEDLE │
│ │ CRICOTHYROTOMY CRICOTHYROTOMY │
│ │ (preferred) + TTJV │
│ │ │ (children) │
│ │ ▼ │
│ │ 6 mm cuffed ETT via │
│ │ bougie / scalpel-bougie │
│ │ technique │
│ │ │ │
│ │ ▼ │
│ │ Stabilize → Plan for tracheostomy │
│ └─────────────────────────────────────┘
│
▼
Awaken patient if possible /
continue with definitive plan
Based on: ASA Difficult Airway Algorithm; DAS 2015 Guidelines; Barash 9e; Miller's 10e; Rosen's Emergency Medicine
POST-PROCEDURE CONSIDERATIONS
- Cricothyrotomy is NOT a permanent airway - conversion to formal tracheostomy should be planned
- Confirm placement with capnography and bilateral auscultation
- Secure tube with tapes/ties/sutures
- Plan for ICU admission
- Decannulate as soon as clinically feasible to reduce subglottic stenosis risk
KEY POINTS SUMMARY
- CTM is ~9 mm × 30 mm, subcutaneous, midline - the safest anterior neck access point
- Three techniques: Needle (TTJV), Surgical (Open), Percutaneous Seldinger
- Primary indication: CICO (SpO₂ <90%, failed BVM, failed ≥3 intubation attempts)
- Surgical cricothyrotomy is contraindicated below age 5-12 years; needle technique is preferred in children
- Dedicated kink-resistant catheters and high-pressure (35-50 psi) O₂ are mandatory for effective TTJV
- Surgical technique has highest success rate (90-100%); cannula technique ~50% by anaesthesiologists
- Not a permanent airway - convert to tracheostomy after stabilisation
- The feared complication of subglottic stenosis is now known to be infrequent
References:
- Barash Clinical Anesthesia, 9e - pp. 2405-2411
- Miller's Anesthesia, 10e - Box 40.4, pp. 5958-5962
- Tintinalli's Emergency Medicine, 9e - Chapter 30, Tables 30-3, 30-5
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, 7e - Chapter 6, Boxes 6.2, 6.3
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 19, Chapter 55, Figure 55-6
- Washington Manual of Medical Therapeutics - pp. 3514-3568
- Rosen's Emergency Medicine, 9e - Chapter 1 (Failed Airway Algorithm)
This is a shared conversation. Sign in to Orris to start your own chat.