Surgical site infection ms ortho 20 marks answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content from Campbell's Operative Orthopaedics 2026 and Mulholland's Surgery. Let me now write the complete 20-mark MS Ortho answer.
Surgical Site Infection (SSI) - MS Orthopaedics 20 Marks
DEFINITION
A Surgical Site Infection (SSI) is an infection occurring at the operative site within 30 days of a procedure (or within 1 year if an implant is left in place) that appears related to the operative procedure.
- CDC/NHSN 2017 guidelines provide the current standard definitions.
- Reported incidence: 2-5% of all surgical procedures; in orthopaedics, deep implant-related infection rates are 0.5-2% for joint arthroplasty.
CLASSIFICATION (CDC/NHSN)
The three anatomical types are depicted below:
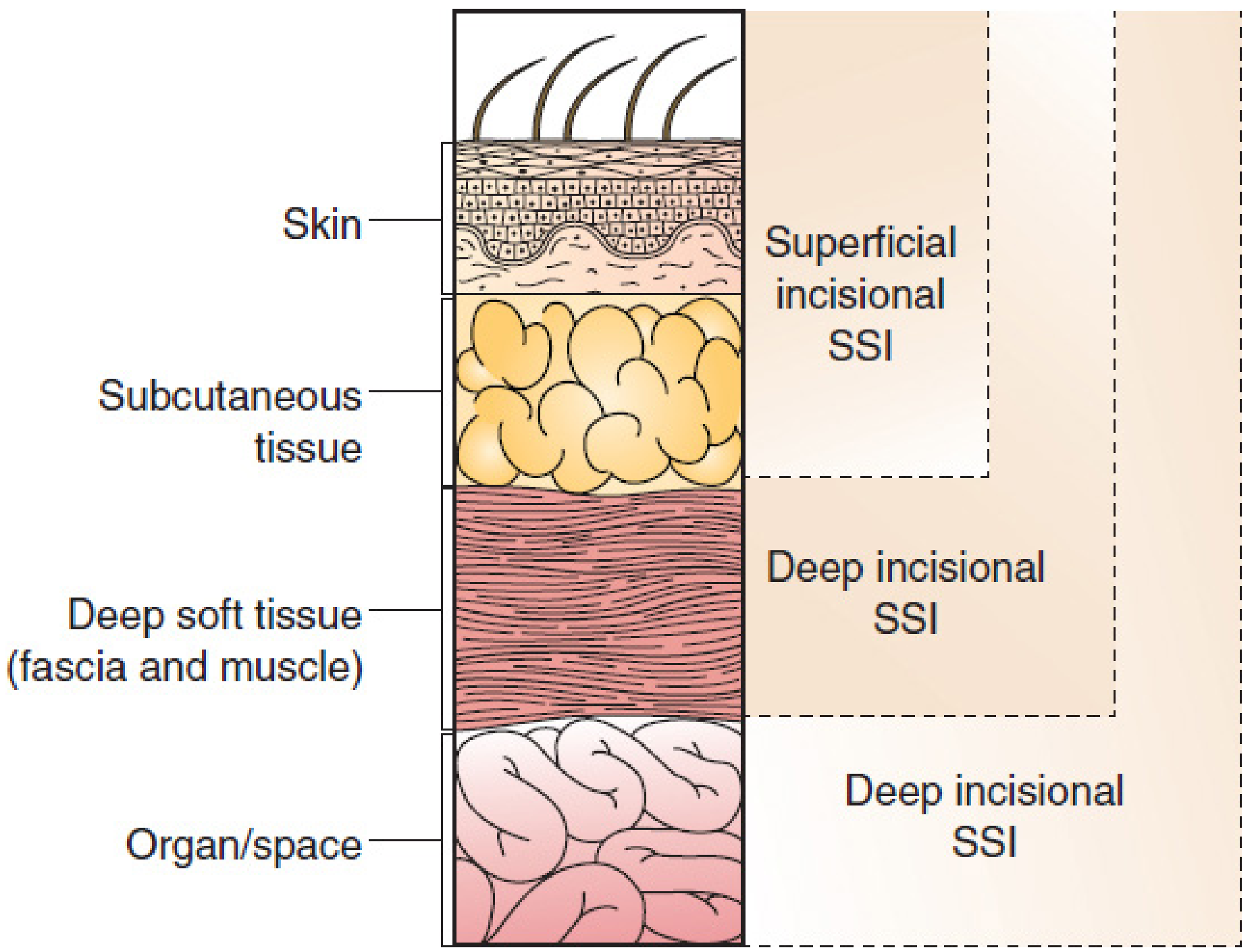
Figure: SSI definitions by CDC (Mulholland & Greenfield's Surgery, 7e, p.497)
1. Superficial Incisional SSI
- Occurs within 30 days after surgery
- Involves only skin and subcutaneous tissue
- Criteria (at least one): purulent drainage, positive culture, pain/tenderness/swelling/erythema/heat + deliberate opening by surgeon, or diagnosis by attending surgeon
2. Deep Incisional SSI
- Occurs within 30 days (no implant) or within 1 year (with implant)
- Involves deep soft tissues: fascia and muscle layers
- Criteria (at least one): purulent drainage from deep incision (not organ/space), spontaneous or deliberate dehiscence with fever >38°C or localized pain/tenderness, abscess or other evidence of infection on direct examination or reoperation, or diagnosis by surgeon
3. Organ/Space SSI
- Involves any part of the body other than the skin incision, fascia, or muscle that was opened or manipulated during surgery (e.g., joint space, bone, intra-articular abscess)
- Particularly relevant in orthopaedics: periprosthetic joint infection (PJI), osteomyelitis
WOUND CLASSIFICATION (NRC/CDC)
| Class | Type | Definition | SSI Risk |
|---|---|---|---|
| I | Clean | No inflammation; respiratory, GI, GU not entered | 1-3% |
| II | Clean-contaminated | Controlled entry into respiratory, GI, GU tracts | 3-11% |
| III | Contaminated | Open fresh traumatic wounds, gross spillage | 10-17% |
| IV | Dirty/Infected | Old traumatic wounds, established infection, perforated viscus | >27% |
ETIOLOGY AND MICROBIOLOGY
Common Causative Organisms in Orthopaedic Surgery
The most common organisms are gram-positive cocci because patient skin is the primary source of orthopaedic infection:
| Organism | Notes |
|---|---|
| Staphylococcus aureus | Most common; MRSA now comprising ~49% of SSI isolates |
| Staphylococcus epidermidis | Increasingly common; antibiotic-resistant; often forms biofilm on implants |
| Streptococcus spp. | Common in joint arthroplasty |
| Escherichia coli / Proteus | Also covered by standard prophylaxis |
| Pseudomonas aeruginosa | Gram-negative; more common in open fractures (Gustilo III) |
| Anaerobes | Relevant in contaminated/dirty wounds |
MRSA has emerged as the leading cause of postoperative infection in vascular and orthopaedic surgery, associated with substantially increased morbidity, hospital stay, and implant/graft removal rates. - Mulholland and Greenfield's Surgery, 7e, p.507
RISK FACTORS
A. Patient-Related (Non-Modifiable / Modifiable)
| Factor | Recommendation |
|---|---|
| Diabetes mellitus | Perioperative glycemic control; maintain serum glucose <180 mg/dL |
| Obesity (BMI ≥35) | Strongest independent risk; weight-adjusted antibiotic dosing |
| Smoking | Cessation at least 30 days preoperatively |
| Malnutrition | Optimize albumin/protein status before elective surgery |
| Immunosuppression | Minimize if possible; adjust antibiotic coverage |
| MRSA colonization | Preoperative nasal swab; decolonization with mupirocin + chlorhexidine baths |
| Remote infection | Treat and eradicate before elective orthopaedic procedure |
| Anemia | Preoperative optimization; blood transfusion increases SSI risk by impairing macrophage function |
| ASA score >2 | Major component of NNIS/NHSN risk index |
B. NHSN SSI Risk Index (NNIS Score)
Three independent variables - one point each:
- ASA score ≥ 3
- Wound class III or IV (contaminated or dirty)
- Operative duration > 75th percentile for that procedure
Score 0 = low risk; Score 2-3 = high risk. Laparoscopic approach reduces score by 1.
C. Procedure-Related Factors
- Wound classification
- Perioperative antibiotics (timing, selection, duration)
- Intraoperative hypothermia
- Blood loss and transfusion
- Surgical duration (risk increases 37% per additional 60 minutes; 25% per 20 minutes)
- Skin preparation method
- Hair removal technique (clipping - not shaving)
- Operating room traffic and door openings
- Surgeon technique - dead space, tissue handling
PATHOGENESIS
- Inoculation of pathogens at time of surgery (primary) or hematogenous spread to implant (secondary, can occur years later)
- Biofilm formation on orthopaedic implants: bacteria adhere to metal/polymer surfaces, secrete extracellular polysaccharide matrix, rendering them resistant to antibiotics and host defenses
- Contamination sources: patient's own skin flora (primary), airborne particles (5,000-55,000 shed/min per person in OR), surgical team, equipment
- Airborne bacteria are predominantly gram-positive and originate almost exclusively from humans in the OR - Campbell's Operative Orthopaedics, 15e, p.963
DIAGNOSIS
Clinical Features
- Early infection (within weeks): wound erythema, warmth, swelling, discharge, dehiscence, fever
- Late/chronic infection (months-years with implants): persistent or new-onset pain, sinus tract formation, implant loosening, failure of fracture fixation
Investigations
Laboratory:
- WBC count - often elevated but non-specific
- ESR - sensitive but non-specific
- CRP - more reliable; typically returns to normal by 3 weeks post-op; persistently elevated = suspect infection
- D-dimer - noninferior to CRP in diagnosis of PJI (2023 data)
- Procalcitonin, IL-6 - emerging markers
Microbiological:
- Gram stain and culture - mandatory before empiric treatment; critical in era of multidrug-resistant pathogens
- Deep wound swabs, tissue biopsy, joint aspirate
- Synovial fluid analysis: WBC >3000 cells/µL, PMN >80% suggestive of PJI
Imaging:
- Plain X-ray: periosteal reaction, bone resorption at bone-cement interface, osteolysis, cyst formation (usually late)
- CT scan: soft tissue involvement, sinus tracts, abscess
- MRI: best for soft tissue and marrow involvement
- Nuclear medicine:
- Technetium-99m bone scan: sensitive but non-specific
- Indium-111-labeled WBC scan combined with technetium scan: differentiates infection from aseptic loosening; sensitivity 64-77%, specificity 78-86%
PREVENTION
I. Preoperative Measures
- Screen and treat remote infection before elective orthopaedic surgery
- MRSA decolonization: nasal swab PCR; mupirocin ointment + chlorhexidine baths if positive
- Glycemic control: HbA1c optimization before elective procedures
- Smoking cessation: at least 30 days preoperatively
- Nutritional optimization: correct hypoalbuminemia
- Skin antisepsis: chlorhexidine-alcohol preparation is superior to povidone-iodine
- Hair removal: clip (do not shave) - shaving creates skin micro-abrasions
II. Perioperative/Intraoperative Measures
Prophylactic Antibiotics (Campbell's Concepts):
- Begin 30-60 minutes before skin incision (60-120 min for vancomycin/fluoroquinolones)
- First-generation cephalosporin (Cefazolin) is drug of choice: weight-adjusted - 1g (<60 kg), 2g (60-120 kg), 3g (>120 kg)
- Redose every 4 hours intraoperatively or when blood loss exceeds 1500 mL
- Stop within 24 hours post-operatively (not extended even with drains/catheters in situ)
- If penicillin allergy (anaphylaxis): vancomycin (15 mg/kg over ≥1 hr to prevent Red Man Syndrome) or clindamycin
- Cephalosporins are preferred over semisynthetic penicillins as they are more effective against S. epidermidis
- For hip/knee arthroplasty: cefazolin or cefuroxime; vancomycin if β-lactam allergy
Operative Technique:
- Strict aseptic technique; minimize OR personnel and door openings
- Gentle tissue handling; obliterate dead space
- Minimize operative time (<2.5 hours when possible)
- Control blood loss; use tranexamic acid
- Irrigation: 3L for Gustilo I, 6L for Gustilo II, 9L for Gustilo III open fractures
- 0.3% Povidone-iodine irrigation - 2.3-fold reduction in SSI, recommended by CDC and WHO (avoid if articular cartilage present)
- Do NOT add antibiotics to irrigation solution routinely (no added benefit)
- Topical vancomycin powder: reduces SSI in spine surgery; mixed evidence vs IV vancomycin
OR Environment:
- Hand washing: 2-minute hand scrub equally effective as traditional 5-minute scrub; alcohol-based hand rubs with chlorhexidine are superior to povidone-iodine scrubs
- Laminar flow: NOT routinely recommended; horizontal laminar flow may paradoxically increase infection rates
- Ultraviolet light: effective but not recommended due to risk to personnel; useful for terminal room cleaning
- Double-glove technique; change gloves when perforation noted
Physiological:
- Maintain normothermia (hypothermia impairs neutrophil function and wound healing)
- Supplemental oxygen intraoperatively
- Perioperative glucose <180 mg/dL
III. Postoperative Measures
- Incisional negative pressure wound therapy (iNPWT): superior to silver-impregnated dressings in high-risk patients (e.g., total joint arthroplasty)
- Subcuticular sutures with skin adhesive preferred; avoid non-absorbable sutures
- Avoid excessive electrocautery
- Wound monitoring, early detection
TREATMENT
SSI Treatment - Four-Step Strategy (Mulholland & Greenfield's Surgery, 7e)
- Early empiric antimicrobial therapy - directed against likely pathogens (gram-positive coverage as default; gram-negative cover for open fractures, immunocompromised)
- Decision on wound opening - open if fluctuance, purulent drainage, or wound dehiscence present; debride necrotic tissue
- Pathogen identification - Gram stain + culture from wound ALWAYS before or at time of opening (mandatory in era of MDR organisms)
- De-escalation of antimicrobial therapy once culture and sensitivity results are available
Management by SSI Type
Superficial SSI:
- Wound opening, irrigation, debridement
- Dressing changes
- Oral/IV antibiotics guided by culture
Deep Incisional SSI (without implant):
- Surgical debridement, washout
- Open wound management with delayed primary closure or secondary healing
- IV antibiotics
Deep Infection with Implant (Periprosthetic Joint Infection):
| Timing | Management |
|---|---|
| Early acute (<3 weeks, well-fixed implant) | Irrigation, debridement, polyethylene exchange (DAIR - Debridement, Antibiotics, Implant Retention) |
| Late chronic | Two-stage revision arthroplasty (gold standard): Stage 1 - implant removal + antibiotic spacer; Stage 2 - reimplantation after 6-12 weeks of IV antibiotics |
| Acute hematogenous (previously well-functioning, now acutely infected) | DAIR if <3-4 weeks duration and well-fixed prosthesis |
Open Fracture Infection:
- Debridement, repeated if needed
- External fixation if internal fixation compromised
- Antibiotic-impregnated beads/spacers (local delivery)
- Bone grafting after infection eradication
MRSA Bundle (when MRSA SSI diagnosed):
- MRSA nasal screening (PCR) on admission/transfer/discharge
- Contact isolation of positive patients
- Standardized hand hygiene
- Cultural transformation - staff and leadership engagement
- Targeted decolonization therapy
CURRENT CHALLENGES IN SSI
- Rising MRSA prevalence: increased from 22.5% (1986-2003) to 49.2% of all SSI isolates by 2007
- Increasingly elderly, obese, and immunocompromised patients undergoing orthopaedic surgery
- More prosthetic device implantations - biofilm-forming organisms
- Antibiotic resistance: coagulase-negative staphylococci (S. epidermidis) increasingly resistant; need for antibiogram-guided prophylaxis
- Cost burden: PJI is one of the most expensive complications in orthopaedic surgery
SUMMARY TABLE: Key Points for Exam
| Aspect | Key Fact |
|---|---|
| Definition | Infection at operative site within 30 days (1 year with implant) |
| Classification | Superficial / Deep incisional / Organ-space |
| Most common organism | S. aureus (MRSA now ~49% of isolates) |
| Drug of choice prophylaxis | Cefazolin (weight-adjusted); Vancomycin if penicillin allergy |
| Antibiotic timing | 30-60 min before incision; stop within 24 hrs |
| NNIS Risk Index | ASA ≥3 + Wound class III/IV + Op duration >75th percentile |
| Irrigation SSI reduction | 0.3% povidone-iodine (2.3x reduction; avoid if articular surface) |
| Gold standard for chronic PJI | Two-stage revision arthroplasty |
| DAIR criteria | Well-fixed implant, acute infection <3 weeks |
| Best blood marker | CRP (returns to normal reliably post-op) |
Sources:
- Campbell's Operative Orthopaedics, 15th Ed 2026 (Chapter 22 - SSI Prevention)
- Mulholland & Greenfield's Surgery: Scientific Principles and Practice, 7e (Chapter 8 - SSI)
- Sabiston Textbook of Surgery, The Biological Basis of Modern Surgical Practice
- CDC/NHSN Guidelines 2017; WHO Global Guidelines for Prevention of SSI, 2017; SCIP/SIP Performance Measures
This is a shared conversation. Sign in to Orris to start your own chat.