UTI empirical treatment
Reading File
Finding Sources
Searching PubMed
"urinary tract infection" AND "empirical treatment" AND "antibiotic"
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a structured summary of empirical UTI treatment based on multiple authoritative textbooks.
Empirical UTI Treatment
The appropriate empirical regimen depends on three factors: (1) whether the infection is uncomplicated or complicated, (2) the anatomical site (lower vs upper tract), and (3) patient-specific factors such as sex, pregnancy, immunosuppression, or structural abnormalities.
1. Uncomplicated Lower UTI (Acute Cystitis) - Adult Non-pregnant Women
These are first-line preferred agents (IDSA guidelines emphasized):
| Agent | Dose | Duration | Notes |
|---|---|---|---|
| Nitrofurantoin (monohydrate/macrocrystals) | 100 mg BD | 5 days | First-line; resistance <5% for E. coli; avoid if GFR <30; NOT for pyelonephritis |
| TMP-SMX DS (160/800 mg) | 1 tab BD | 3 days | Use only if local resistance <20%; low collateral damage, low cost |
| Fosfomycin | 3 g single dose | Single dose | First-line where available; 2% resistance rate; effective vs ESBL E. coli |
| Pivmecillinam | 400 mg BD | 5 days | Primarily European; active vs ESBL; minimal collateral damage |
Second-line (if first-line unsuitable):
- Oral fluoroquinolone (e.g., ciprofloxacin 250 mg BD x 3 days) - use sparingly to preserve activity for serious infections; the FDA states risks outweigh benefits for uncomplicated cystitis
- Beta-lactams: cefpodoxime, cefdinir, cefaclor, or amoxicillin-clavulanate in 3-7 day courses - generally inferior to TMP-SMX or fluoroquinolones
- Aminopenicillins alone (amoxicillin) are NOT recommended as first-line due to resistance and Klebsiella selection risk
No initial urine culture is required for uncomplicated cystitis. Culture community resistance patterns if TMP-SMX is considered.
2. Outpatient Pyelonephritis (Uncomplicated, Tolerating Orals)
| Agent | Dose | Duration |
|---|---|---|
| Ciprofloxacin | 500 mg BD | 5-7 days |
| Levofloxacin | 750 mg OD | 5 days |
| TMP-SMX DS | 1 tab BD | 7-14 days (if susceptible) |
- Fluoroquinolones are the most studied agents for pyelonephritis, but quinolone resistance is now increasing
- Where fluoroquinolone resistance exceeds 10% locally, give an initial single IV/IM dose of a beta-lactam or aminoglycoside before starting oral therapy, then switch to oral once culture sensitivities return
- Avoid nitrofurantoin, fosfomycin, and pivmecillinam for pyelonephritis - these do not achieve adequate renal tissue levels
- Oral beta-lactams are less effective and require close follow-up with a longer course if used
3. Inpatient / Complicated UTI (Including Pyelonephritis Requiring Admission)
(Tintinalli Table 91-6 / Harrison's 22E)
| Agent | Dose |
|---|---|
| Ceftriaxone | 1-2 g IV OD |
| Ciprofloxacin | 400 mg IV q12h |
| Cefotaxime | 1-2 g IV q8h |
| Cefepime | 1-2 g IV q8h |
| Piperacillin-tazobactam | 3.375 g IV q6h |
| Gentamicin/tobramycin ± ampicillin | 3 mg/kg/d div q8h ± ampicillin 2 g q6h |
| Ertapenem | 1 g IV OD |
| Meropenem | 1 g IV q8h |
| Imipenem | 500 mg IV q8h |
Alternatives include ceftazidime, amikacin, and meropenem-vaborbactam (for drug-resistant uropathogens). Once the patient improves clinically, step down to oral agents guided by culture sensitivities.
Total treatment duration:
- 7-14 days for most complicated UTI/pyelonephritis
- 21 days if sepsis syndrome present
4. Special Populations
Complicated UTI (defined as UTI in males, diabetics, immunosuppressed, abnormal urinary tract, indwelling catheter, stone disease, spinal cord injury)
- Urine culture should be obtained before starting antibiotics whenever possible
- Empirical treatment follows inpatient regimens above
- Imaging (KUB + renal US, or CT) is indicated to exclude obstruction/stones
- Antibiotics alone may be insufficient - surgical drainage or stone removal may be required
Men with UTI
- All UTI in males is by definition complicated
- In men <50 years, STI must be excluded first
- In men >50 years, consider underlying LUTS/prostate pathology
- Treat for 7 days (rather than 14), which is sufficient if uncomplicated prostate involvement is absent
Prostatitis
- Acute bacterial prostatitis: fluoroquinolone or TMP-SMX for at least 2-4 weeks
- Chronic bacterial prostatitis: 4-6 weeks (up to 12 weeks for recurrences)
Pregnancy
- Beta-lactams, nitrofurantoin (avoid near term), fosfomycin, metronidazole, and vancomycin are generally considered safe
- Avoid: fluoroquinolones and tetracyclines
- Asymptomatic bacteriuria must be treated in pregnancy (unlike in non-pregnant adults)
5. Recurrent UTI - Prophylaxis
For women with ≥3 UTIs/year or ≥2 in 6 months:
| Agent | Dose | Schedule |
|---|---|---|
| Nitrofurantoin | 50-100 mg | Daily continuous, or postcoital |
| TMP-SMX | 40/200 mg | Daily, 3x/week, or postcoital |
| Trimethoprim | 100 mg | Daily |
| Cephalexin | 125-250 mg | Daily or postcoital |
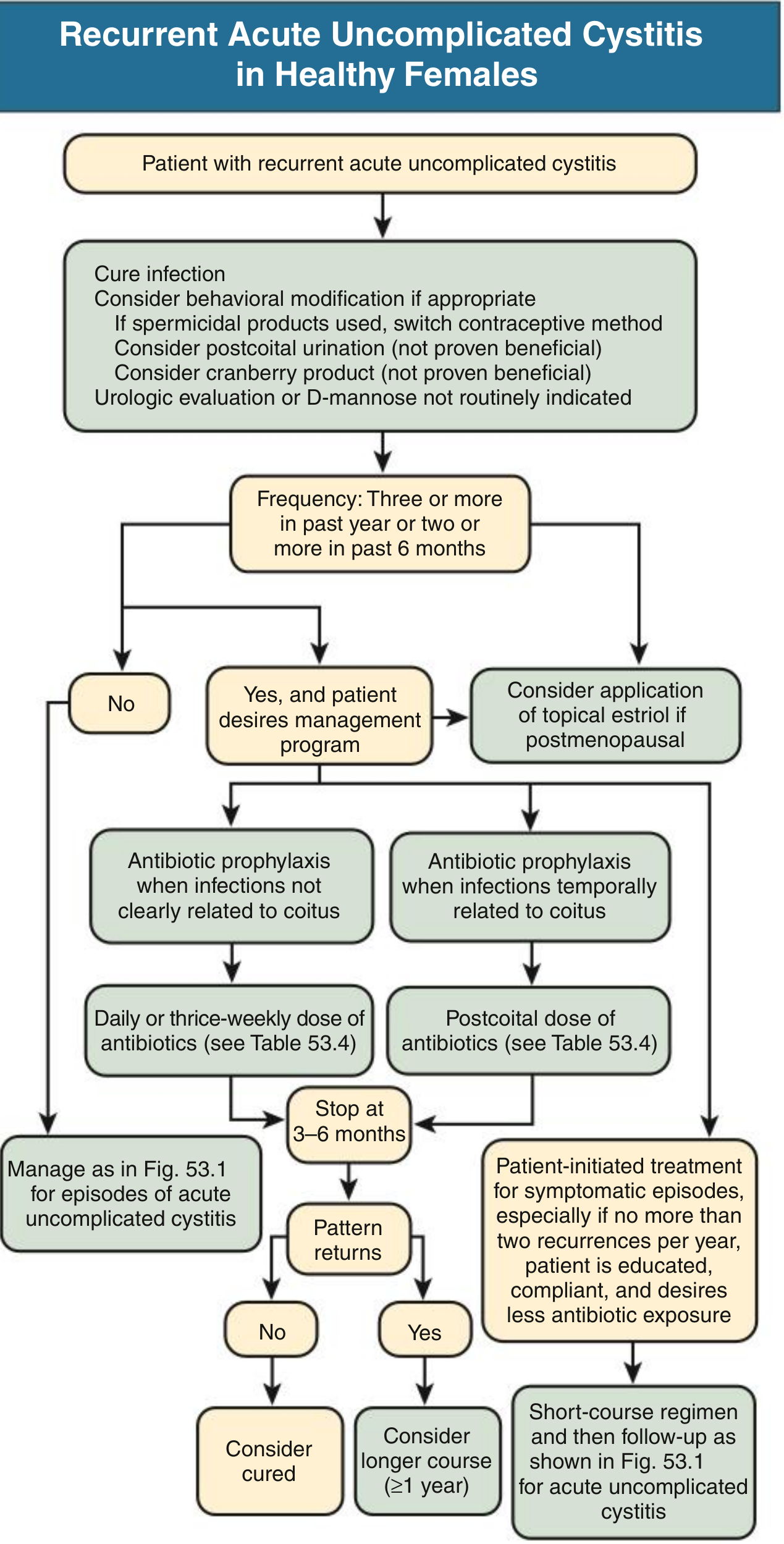
Recurrent cystitis management flowchart - Comprehensive Clinical Nephrology, 7th Edition
Key Principles
- Always check local resistance rates - TMP-SMX should not be used empirically if local E. coli resistance exceeds 20%
- Fluoroquinolones should be reserved for pyelonephritis or complicated infections - avoid for simple cystitis to preserve efficacy
- ESBL-producing organisms: nitrofurantoin and fosfomycin remain active (resistance ~6% and 3% respectively)
- Avoid aminopenicillins (amoxicillin alone) as empirical therapy due to high resistance rates and risk of selecting Klebsiella
Sources: Tintinalli's Emergency Medicine (Table 91-5, 91-6); Harrison's Principles of Internal Medicine 22E; Comprehensive Clinical Nephrology 7th Ed (Table 53.3, 53.4); Sabiston Textbook of Surgery; Smith & Tanagho's General Urology; Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.