Normal pulmonary capillary wedge pressure.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
I now have solid data from multiple authoritative textbooks. Here is the full answer:
Normal Pulmonary Capillary Wedge Pressure (PCWP)
Normal range: 6-12 mmHg (most commonly cited), with an upper limit of normal of 15 mmHg accepted in clinical practice.
| Source | Normal PCWP Value |
|---|---|
| Goldman-Cecil Medicine (25th ed.) | 8-15 mmHg (PAOP/PAWP) |
| Fishman's Pulmonary Diseases and Disorders | ≤15 mmHg |
| Murray & Nadel's Respiratory Medicine | ~10 mmHg (mean); end-expiratory should be used |
- Goldman-Cecil Medicine, Table 94-3, p. 3779
- Fishman's Pulmonary Diseases, Table 97-2
Key Points
What it measures:
- PCWP (also called PAOP - pulmonary artery occlusion pressure, or PAWP - pulmonary artery wedge pressure) is an indirect measure of left atrial pressure (LAP) and left ventricular end-diastolic pressure (LVEDP).
- It is measured by inflating the balloon of a pulmonary artery catheter (Swan-Ganz) until it "wedges" in a distal pulmonary artery branch, reflecting the static column of blood back to the left atrium.
Normal hemodynamic context (Goldman-Cecil Medicine):
| Parameter | Normal Value |
|---|---|
| CVP | 6-12 mmHg |
| PAP (systolic/diastolic) | 25/15 mmHg |
| PCWP (PAOP/PAWP) | 8-15 mmHg |
| Cardiac output | ~5 L/min |
| Cardiac index | 2.5-4.2 L/min/m² |
Clinical Significance
| PCWP Value | Interpretation |
|---|---|
| < 6 mmHg | Hypovolemia |
| 6-12 mmHg | Normal |
| Up to 15 mmHg | Upper limit of normal (accepted by most guidelines) |
| 18-20 mmHg | Suggests left heart failure / pulmonary congestion |
| > 25 mmHg | Severe pulmonary edema likely |
Important Technical Note
Miller's Anesthesia (10th ed.) points out that the term "pulmonary capillary wedge pressure" is technically a misnomer - the correct terms are pulmonary artery wedge pressure (PAWP) or pulmonary artery occlusion pressure (PAOP). True pulmonary capillary hydrostatic pressure (which drives edema formation per Starling forces) is actually slightly higher than PAWP, and the two should not be conflated.
Additionally, when a patient is on positive-pressure ventilation or PEEP, end-expiratory PCWP should be used to avoid overestimation of the true filling pressure. - Murray & Nadel's Textbook of Respiratory Medicine
Why in porto pulmonary hypertension? The pulmonary capillary wedge pressure remains less than 15.
Finding Sources
Searching the Web
portopulmonary hypertension PCWP less than 15 pre-capillary mechanism
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is the complete explanation:
Why PCWP Remains < 15 mmHg in Portopulmonary Hypertension (POPH)
The short answer: POPH is a pre-capillary disease. The problem is in the pulmonary arterioles themselves - not in the left heart or pulmonary venous system. Since there is no left-sided obstruction or failure, the pressure downstream of the capillary bed (i.e., the pressure reflected back through the wedge) stays normal.
The Core Concept: Pre-capillary vs. Post-capillary Hypertension
| Type | Mechanism | mPAP | PCWP | PVR |
|---|---|---|---|---|
| Pre-capillary PH (e.g., POPH, idiopathic PAH) | Pulmonary arteriolar disease | ↑↑↑ | ≤ 15 mmHg (normal) | ↑↑↑ |
| Post-capillary PH (e.g., left heart failure) | Elevated left-sided filling pressure | ↑↑ | > 15 mmHg (elevated) | Normal or mildly ↑ |
In post-capillary PH, the elevated PCWP tells you that pressure is backing up from the left atrium through the pulmonary veins and capillaries into the pulmonary arteries. In POPH, the obstruction is before the capillaries - at the level of the pulmonary arterioles - so pressure cannot build up backward to elevate the PCWP.
Pathophysiology of POPH: Why Arterioles Are the Target
In portal hypertension, portosystemic shunting exposes the pulmonary vasculature to substances that would normally be cleared by the liver:
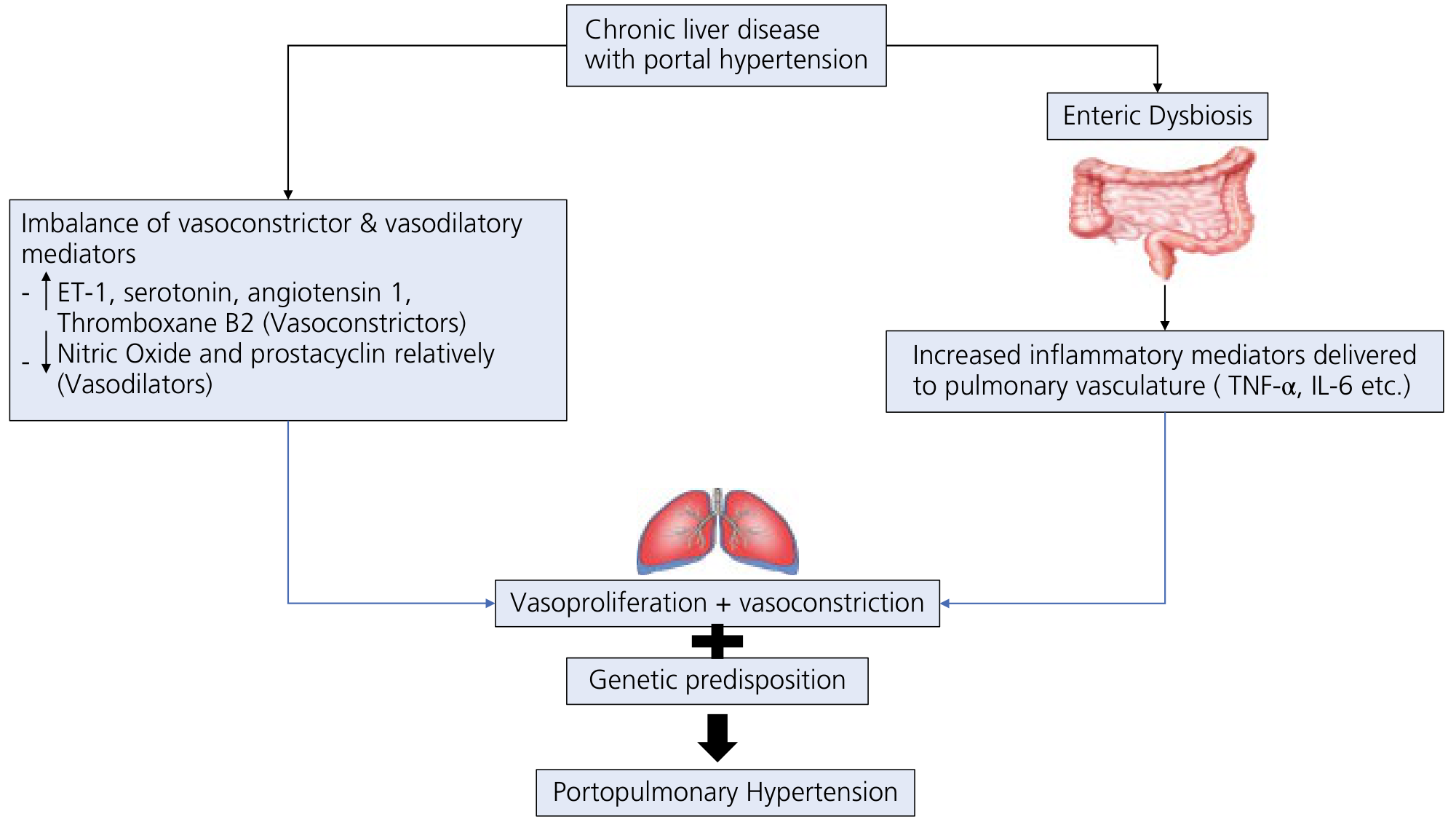
Yamada's Textbook of Gastroenterology, 7th ed., Fig. 99.6
These include:
- Vasoconstrictors: ET-1, serotonin, thromboxane B2, angiotensin 1
- Inflammatory mediators (via enteric dysbiosis): TNF-α, IL-6
- Relative deficiency of vasodilators: decreased NO and prostacyclin
The result is vasoproliferation + vasoconstriction at the pulmonary arteriolar level, producing:
- Intimal fibrosis
- Medial smooth muscle hypertrophy
- Plexiform lesions
- In-situ microthrombosis with recanalization
These structural changes obstruct flow in the pulmonary arterioles, causing dramatically elevated PVR and hence elevated mPAP - but the left atrium and pulmonary veins remain completely uninvolved, so PCWP stays normal.
The Hemodynamic Comparison in Cirrhosis
Yamada's Textbook of Gastroenterology clearly illustrates the three patterns that can raise mPAP in cirrhosis and why only POPH keeps PCWP normal:
| Condition | mPAP | PCWP | PVR | Cardiac Output |
|---|---|---|---|---|
| Hyperdynamic circulation | ↑ | Normal | Normal | ↑↑↑ |
| Volume overload | ↑↑ | ↑↑ (elevated) | Normal/↑ | ↑↑ |
| Portopulmonary hypertension | ↑↑↑ | Normal (≤15) | ↑↑↑ | Initially ↑↑↑, drops at end stage |
- Yamada's Textbook of Gastroenterology, 7th ed., Table 99.10
This table is diagnostically key: volume overload raises PCWP because it overloads the left heart; POPH does not touch the left heart, so PCWP stays normal despite massively elevated mPAP.
Formal Diagnostic Criteria for POPH
Right heart catheterization must demonstrate all three:
- mPAP > 25 mmHg (at rest)
- PCWP < 15 mmHg (normal - confirms pre-capillary location of disease)
- PVR > 3 Wood units (240 dynes·s·cm⁻⁵)
The PCWP < 15 mmHg criterion is what definitionally separates POPH (and all Group 1 PAH) from pulmonary hypertension due to left heart disease. - European Respiratory Review, PoPH & HPS and Harrison's Principles of Internal Medicine, 22nd ed.
In one sentence: PCWP is normal in POPH because the disease process (vasoconstriction and vasoproliferation from gut-derived mediators) affects only the pulmonary arterioles, never reaching the left atrium - so there is no backward pressure elevation to register at the wedge position.
Cirrhosis r cardio myopathy.
Finding Sources
Searching the Web
cirrhotic cardiomyopathy pathophysiology diagnosis criteria 2024
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Here is the complete answer:
Cirrhotic Cardiomyopathy (CCM)
Definition
CCM is defined as chronic cardiac dysfunction in patients with cirrhosis, characterized by impaired contractile responsiveness to stress and/or altered diastolic relaxation with electrophysiological abnormalities, in the absence of other known cardiac disease.
- First formally defined at the 2005 World Congress of Gastroenterology, later refined by the Cirrhotic Cardiomyopathy Consortium (2019) with updated echocardiographic criteria.
- Affects up to 50% of all cirrhotic patients and is often unrecognized clinically.
- Fuster & Hurst's The Heart, 15th ed., p. 1293
Why It Goes Unrecognized
The low systemic vascular resistance (SVR) of cirrhosis (from splanchnic vasodilation) reduces afterload dramatically. This masks the underlying poor LV function on routine echo - the heart appears to function normally because it is pumping against very little resistance. Only under physiologic or pharmacologic stress is the dysfunction unmasked. - Morgan & Mikhail's Clinical Anesthesiology, 7th ed., p. 3977
Pathophysiology
The fundamental mechanism is progressive failure of compensatory mechanisms in the face of splanchnic vasodilation:
Several factors drive the myocardial impairment:
| Factor | Mechanism |
|---|---|
| Intestinal bacterial translocation | Inflammation-mediated LV remodeling |
| Cytokines (TNF-α, IL-6) | Negative inotropic effects |
| Nitric oxide & carbon monoxide | Vasodilation + negative inotropy |
| Endogenous cannabinoids | Negative inotropic + chronotropic effects |
| Bile acid accumulation | Oxidative stress + mitochondrial impairment in cardiomyocytes |
| ↓ β-adrenoceptor density/signaling | Blunted response to catecholamines and stress |
| RAAS activation | LV dilation and remodeling |
- Fuster & Hurst's The Heart, 15th ed., p. 1294
Clinical Features
CCM follows a progressive pattern:
| Phase | Predominant Feature |
|---|---|
| Early | Diastolic dysfunction (impaired relaxation), hyperdynamic circulation |
| Advanced | Systolic dysfunction + LV dilation |
| Throughout | Electrophysiological abnormalities |
The Three Diagnostic Pillars
1. Systolic Dysfunction
- Blunted contractile response to physiologic/pharmacologic stress (most common)
- Resting LVEF < 55% (less common in early stages - often masked by low afterload)
- The heart can appear hyperdynamic at rest yet be truly dysfunctional
2. Diastolic Dysfunction (most prevalent - >50% of cirrhotics)
- Impaired LV relaxation and decreased compliance
- Increased left atrial volume
- Assessed by echocardiography with tissue Doppler imaging (TDI):
- E/A ratio (mitral inflow)
- E/E' ratio (transmitral/annular velocity - estimates filling pressure)
- Correlates with disease severity; predicts mortality and is a predictor of death after TIPS placement
- Pretransplant diastolic dysfunction is an independent predictor of post-transplant adverse cardiac events (24% developed HF post-LT in one series)
3. Electrophysiological / Electromechanical Abnormalities
- QTc prolongation - most recognized ECG finding; present in >50% of cases; correlates with cirrhosis severity
- Electromechanical dyssynchrony
- Chronotropic incompetence - failure of heart rate to appropriately increase with stress
- Inotropic incompetence - failure of contractility to increase under demand
- Autonomic dysfunction
Diagnostic Criteria (2005 vs. 2019)
| Criterion | 2005 (World Congress of Gastroenterology) | 2019 (CCM Consortium) |
|---|---|---|
| Systolic dysfunction | Blunted stress response ± resting LVEF < 55% | LVEF < 55% at rest OR blunted stress response |
| Diastolic dysfunction | E/A < 1, deceleration time >200 ms, IVRT >80 ms | ASE/EACVI criteria; E/e' ratio first to assess filling pressure, then E/A grading |
| Other | QTc > 440 ms, enlarged LA, LV hypertrophy, elevated BNP | QTc prolongation, elevated NT-proBNP/troponin, chronotropic incompetence |
- Fuster & Hurst's The Heart, 15th ed., Table 41-8
Clinical Consequences
| Complication | Link to CCM |
|---|---|
| Hepatorenal syndrome (HRS) | CCM → decreased renal blood flow & GFR → higher HRS probability |
| Post-TIPS complications | TIPS increases preload and PAP; diastolic dysfunction predicts death after TIPS |
| Post-liver transplant HF | Diastolic dysfunction pre-transplant predicts intraoperative and early post-op cardiac failure |
| Postreperfusion syndrome | Unmasked LV dysfunction during portal unclamping |
Treatment & Reversibility
-
Liver transplantation is the cornerstone therapy - many cardiac changes of CCM reverse after successful LT
-
Pre-transplant treatment of HF (diuretics, beta-blockers with caution) may reduce perioperative complications
-
CCM does not constitute a contraindication to liver transplantation or TIPS, but must be recognized pre-procedurally
-
Taurine has been studied for mitigating bile acid-mediated mitochondrial damage
-
Miller's Anesthesia, 10th ed., p. 8623; Fuster & Hurst's The Heart, 15th ed., p. 1295
This is a shared conversation. Sign in to Orris to start your own chat.