1) Osteogenic sarcoma
Reading File
Finding Sources
Searching PubMed
"osteosarcoma" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Let me compile the full response.
Osteogenic Sarcoma (Osteosarcoma)
Definition
Osteogenic sarcoma (osteosarcoma) is a malignant tumor whose cells produce osteoid matrix or mineralized bone. It is the most common non-hematopoietic primary malignant tumor of bone.
- Incidence: ~3-4 per million population per year
- Male predominance: M:F = 1.6:1 (exception: parosteal osteosarcoma is more common in females)
Epidemiology & Age Distribution
The age distribution is bimodal:
- First peak (75% of cases): Adolescents - coincides with the pubertal growth spurt (most 10-20 years)
- Second peak: Older adults (>40 years), almost always secondary osteosarcoma
In adolescents, tumors arise preferentially at the metaphyseal region of long bones at sites of most rapid growth: ~50-75% are near the knee (distal femur or proximal tibia). Other sites: proximal humerus, proximal femur, ilium.
Classification (WHO 2013)
| Category | Features |
|---|---|
| Conventional (central) osteosarcoma | ~75% of all; high-grade intramedullary |
| Telangiectatic osteosarcoma | Very high grade; blood-filled cavities; mimics aneurysmal bone cyst |
| Low-grade central osteosarcoma | Indolent, may mimic fibrous dysplasia |
| Small cell osteosarcoma | High grade; mimics Ewing sarcoma |
| Parosteal osteosarcoma | Low grade; arises on bone surface; posterior distal femur |
| Periosteal osteosarcoma | Intermediate grade; diaphyseal surface |
| High-grade surface osteosarcoma | High grade; surface origin |
Secondary osteosarcomas arise in the setting of: Paget disease (~1% risk; 5-10% in polyostotic), previous radiation (>2500 cGy), bone infarcts, fibrous dysplasia, chronic osteomyelitis.
Pathogenesis
The peak incidence at the adolescent growth spurt is linked to increased osteoblastic proliferation near growth plates - increased cell division raises mutation risk. Key molecular events:
- RB mutations - present in up to 70% of sporadic cases; germline RB mutations (hereditary retinoblastoma) increase risk 1000-fold
- TP53 mutations - germline mutations underlie Li-Fraumeni syndrome; somatic mutations common in sporadic tumors
- MDM2 and CDK4 overexpression - inhibit p53 and RB function respectively; common in low-grade osteosarcomas
- CDKN2A inactivation - encodes p16 and p14 tumor suppressors
- MYC amplification - in up to 50% of cases; associated with poor prognosis
Genetic syndromes associated: Li-Fraumeni syndrome (germline TP53), hereditary retinoblastoma (germline RB1), Rothmund-Thomson syndrome.
Clinical Presentation
- Pain - progressive, initially mild, may be misattributed to sports injury; later becomes severe; ~25% have night pain
- Palpable mass - progressively enlarging
- Pathologic fracture - may be the initial presentation
- Average diagnostic delay: ~15 weeks (patient delay 6 weeks + physician delay 9 weeks)
- Low-grade surface lesions may present with a painless mass
Imaging
Plain Radiograph (most valuable first-line tool)
The classic appearance is an aggressive metaphyseal lesion with:
- Mixed lytic and sclerotic pattern (spectrum from entirely lytic 13% to entirely sclerotic)
- Permeative, ill-defined borders
- Cortical destruction and eccentric extra-osseous soft-tissue mass
- Codman triangle - triangular shell of reactive periosteal bone at tumor margin (indicates aggressive tumor, not pathognomonic)
- Sunburst / hair-on-end periosteal reaction
- Onion-skin (lamellated) periosteal reaction

MRI (mandatory for local staging)
- Best modality to define intramedullary extent and soft tissue involvement
- Must image the whole affected bone to identify skip metastases (intraosseous foci separate from main tumor; ~5% of cases)
- Dynamic contrast-enhanced MRI assesses chemotherapy response
Other imaging
- CT chest - for pulmonary metastases (most common metastatic site)
- Bone scan - for skeletal metastases
- FDG-PET-CT - superior to bone scan for bone metastases; established role in evaluating chemotherapy response and detecting recurrence
- Pulmonary metastases may be mineralized and visible on bone scintigraphy; rarely cause pneumothorax
Morphology (Gross & Histology)
Gross: Bulky, gritty, tan-white tumor. Areas of hemorrhage and necrosis. Cortical destruction with soft tissue extension. Extensive intramedullary spread. Rarely crosses the growth plate into the epiphysis.
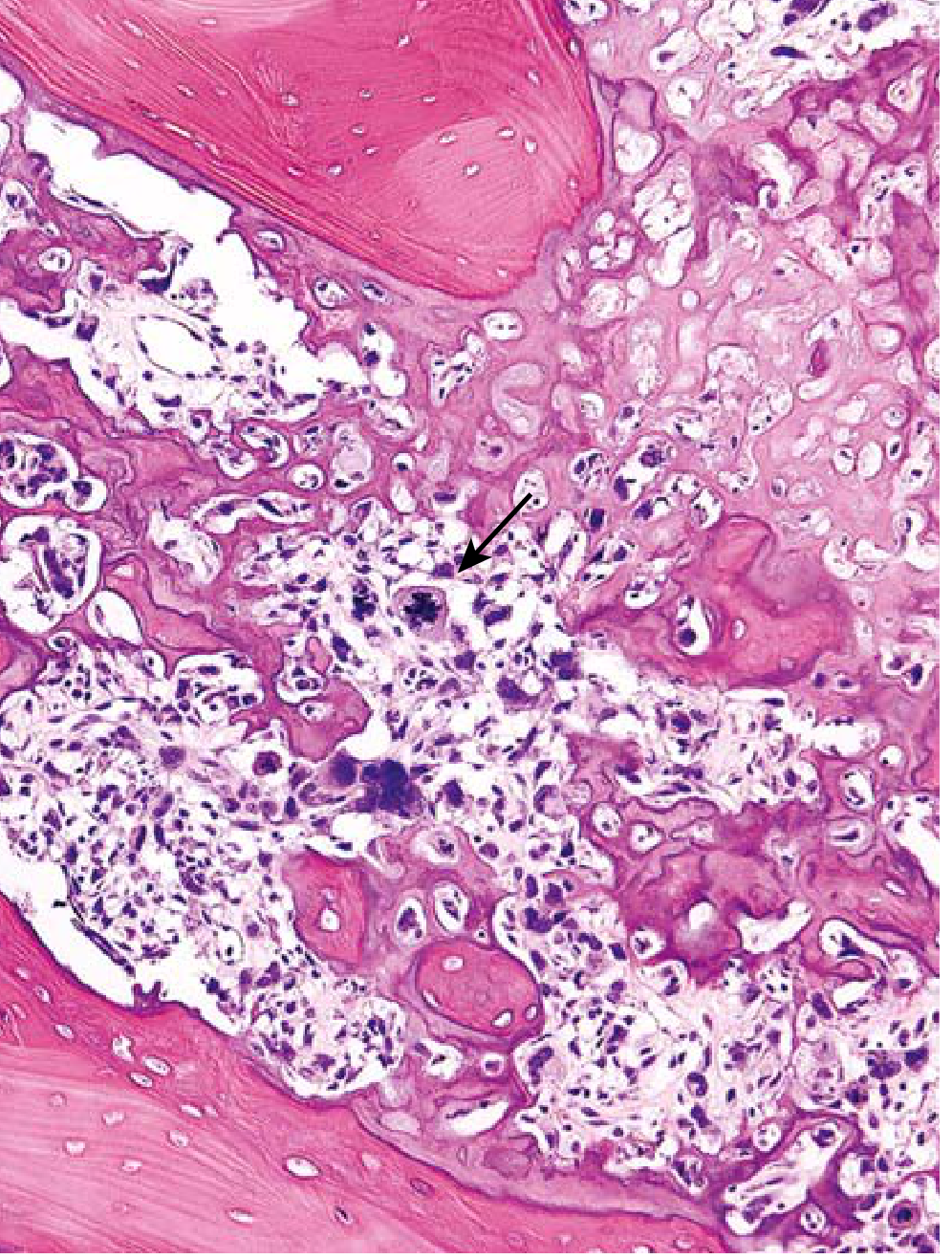
Histology:
- Mandatory diagnostic criterion: Malignant tumor cells producing unmineralized osteoid or mineralized bone (fine lacelike osteoid, or broad sheets/primitive trabeculae)
- Pleomorphic cells with large hyperchromatic nuclei
- Bizarre tumor giant cells
- Abundant mitoses including abnormal forms (e.g., bipolar mitoses)
- Extensive necrosis and intravascular invasion
Variant Subtypes - Key Points
| Subtype | Key Feature |
|---|---|
| Conventional | Most common; high-grade; metaphyseal long bone |
| Telangiectatic | Purely lytic; blood-filled cavities; mimics ABC on imaging and histology; frankly malignant cells in septa on high power |
| Parosteal | Low grade; posterior distal femur surface; ossification more central (vs. peripheral in myositis ossificans); no medullary involvement early; more common in females; no chemo needed |
| Periosteal | Intermediate grade; diaphyseal surface femur/tibia; spindle cells + cartilage lobules |
| Small cell | High grade; small blue cells; mimics Ewing sarcoma/lymphoma; needs cytogenetics/IHC to differentiate |
| Low-grade central | Indolent; mimics fibrous dysplasia or osteoblastoma; slightly atypical spindle cells |
| Secondary | Age >40-50; Paget disease or prior radiation; pelvis most common site for Paget-associated |
Staging & Spread
- All high-grade osteosarcomas are assumed to have occult micrometastases at presentation
- Spread is hematogenous - lungs are the primary site (peripheral, may mineralize)
- Skip metastases occur in ~5% within the same bone
- Lymph node spread is uncommon
- Before chemotherapy era: 80% of patients with apparently localized disease died of distant metastases within 2 years
Treatment
Standard Protocol (High-Grade Osteosarcoma)
- Neoadjuvant chemotherapy (pre-operative) - MAP regimen: Methotrexate (high-dose), Doxorubicin (Adriamycin), Cisplatin (Platinum)
- Wide surgical resection (limb-salvage surgery in most patients) OR amputation
- Adjuvant chemotherapy (post-operative)
- Pulmonary metastases resected if feasible (thoracotomy preferred over thoracoscopy as CT underestimates lesion count)
Histological Response to Neoadjuvant Chemotherapy
- >90% tumor necrosis = excellent response = very good prognosis
- Histologic response is the strongest predictor of long-term survival
- Dynamic MRI can assess response pre-operatively
Low-Grade Osteosarcoma
- Wide resection or amputation alone, no chemotherapy required
Limb Salvage vs. Amputation
- Limb salvage has become standard in the majority (~90%) of extremity tumors
- Pathologic fracture does not necessarily mandate amputation - limb salvage remains viable in select cases, though fracture worsens overall survival and metastasis risk
- Local recurrence after wide resection (~10%) carries very poor prognosis; usually requires radical amputation
Prognosis
| Situation | Survival |
|---|---|
| Non-metastatic high-grade (with modern chemotherapy) | 60-75% long-term survival |
| Pre-chemotherapy era | ~20% (80% mortality) |
| Relapsed/metastatic | Poor; ~30% with complete pulmonary resection |
Favorable prognostic factors:
-
90% tumor necrosis after neoadjuvant chemotherapy
- Non-metastatic at presentation
- Small, peripheral, ipsilateral pulmonary metastases
- Disease-free interval >1 year before relapse
- Complete surgical resection achievable
Poor prognostic factors:
- Metastases at presentation
- Axial skeleton or pelvic primary
- Large tumor size
- Poor neoadjuvant chemo response (<90% necrosis)
- MYC amplification
- Rapid relapse; >8 nodules; nodules >3 cm; unresectable disease
Summary Mnemonic: "OSTEOSARCOMA"
- O - Osteoid production by malignant cells (defining feature)
- S - Second decade of life (peak)
- T - Tumor in metaphysis of long bones (distal femur #1)
- E - Extensive intramedullary spread
- O - Occult micrometastases assumed at presentation
- S - Sunburst / Codman triangle on X-ray
- A - Adolescent growth spurt (pathogenesis)
- R - RB and TP53 mutations (genetics)
- C - Chemotherapy (MAP) + surgery standard
- O - >90% necrosis = good prognostic response
- M - Metastases to lung (hematogenous)
- A - Amputation if wide excision not feasible
Sources:
- Robbins & Kumar Basic Pathology, pp. 782-783
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 1211-1215
- Grainger & Allison's Diagnostic Radiology, pp. 1048-1049
- Recent systematic review: Prognostic factors in relapsed high-grade osteosarcoma (Br J Cancer, 2025 - PMID 40731087)
This is a shared conversation. Sign in to Orris to start your own chat.