Understood - no self-made tables, only use tables that actually appear in Park's textbook. Here are both answers rewritten:
PART 1: National Mental Health Programme (NMHP) & Mental Healthcare Act 2017
Park's Textbook of PSM - 6 Marks
National Mental Health Programme (NMHP)
Launched: 1982, Ministry of Health and Family Welfare, Government of India
Purpose: To ensure availability of Mental Health Care Services for all, especially the community at risk and underprivileged section of the population, to encourage application of mental health knowledge in general health care and social development.
A National Advisory Group on mental health was constituted under the Chairmanship of the Secretary, Ministry of Health and Family Welfare for the effective implementation of the programme.
11 institutions have been identified for imparting training in basic knowledge and skills in the field of mental health to the primary health care physicians and para-medical personnel.
At present this programme covers 517 districts in 36 states.
AIMS of NMHP
(a) Prevention and treatment of mental and neurological disorders and their associated disabilities
(b) Use of mental health technology to improve general health services
(c) Application of mental health principles in total national development to improve quality of life
OBJECTIVES of NMHP
1. To ensure availability and accessibility of minimum mental health care for all in the foreseeable future, particularly to the most vulnerable and underprivileged sections of population.
2. To encourage application of mental health knowledge in general health care and in the social development.
3. To promote community participation in the mental health services development, and to stimulate efforts towards self-help in the community.
PROGRAMME STRATEGIES
1. Integration of mental health with primary health care through the NMHP
2. Provision of tertiary care institutions for treatment of mental disorders
3. Eradicating stigmatization of mentally ill patients and protecting their rights through regulatory institutions like the Central Mental Health Authority and State Mental Health Authority
DISTRICT MENTAL HEALTH PROGRAMME (DMHP) - Components
(a) Training programmes of all workers in the mental health team at the identified nodal institute in the state
(b) Public education in mental health to increase awareness and to reduce stigma
(c) For early detection and treatment, the OPD and indoor services are provided
(d) Providing valuable data and experience at the level of community to the state and centre for future planning, improvement in service and research
DMHP - Promotive & Preventive Activities (Added in Recent Years)
- School mental health services: Life skills education in schools, counselling services
- College counselling services: Through trained teachers/counsellors
- Workplace stress management: Formal & informal sectors, including farmers, women etc.
- Suicide prevention services: Counselling centre at district level, sensitization workshops, IEC, help lines etc.
THRUST AREAS of NMHP
1. District mental health programme in an enlarged and more effective form covering the entire country
2. Streamlining/modernization of mental hospitals in order to modify their present custodial role
3. Upgrading department of psychiatry in medical colleges and enhancing the psychiatric content of the medical curriculum at the undergraduate as well as postgraduate level
4. Strengthening the central and state mental health authorities with a permanent secretariat; appointment of medical officers at state headquarters in order to make the monitoring role more effective
5. Research and training in the field of community mental health, substance abuse and child-adolescent psychiatric clinics
The Mental Healthcare Act, 2017 (HIGH YIELD)
The United Nations convention on the rights of persons with disabilities was ratified by the Government of India, making it obligatory on the Government to align the policies and laws of the country with the convention.
The Mental Healthcare Bill, 2013 was introduced in Parliament in order to:
- Protect and promote the rights of persons with mental illness during delivery of health care
- Ensure treatment and rehabilitation of persons with mental illness in the least restrictive environment possible
- Regulate the public and private mental health sectors within a rights framework
- Achieve the greatest public health good and promote principles of equity, efficiency and active participation of all stakeholders in decision making
The bill received assent of the President of India on 07.04.2017.
KEY HIGH-YIELD POINT: Suicide has been DECRIMINALIZED under the Act.
The NMHP essential services include: (a) Early identification (diagnosis) and treatment of mental illness in the community; (b) Basic services: Diagnosis and treatment of common mental disorders such as psychosis, depression, anxiety disorders and epilepsy, and referral; and (c) IEC activities for prevention, stigma removal, early detection of mental disorders and greater participation/role of community for primary prevention of mental disorders.
PART 2: Community Mental Health Problems
Park's Textbook of PSM - 6 Marks
Magnitude - National Mental Health Survey (NMHS) 2015
Survey was done in 12 states: Kerala, Tamil Nadu, Gujarat, Rajasthan, West Bengal, Jharkhand, Chhattisgarh, Madhya Pradesh, Assam and Manipur.
Key findings of the survey:
1. NMHS indicates that nearly 150 million Indians aged 13 and above are likely to be suffering from one or more mental health problems and are in need of services.
2. Mental health problems are comparatively more prevalent in urban areas.
3. The proportion of those with a mental health disorder in young adolescents was 7.3%
4. Neurosis and stress-related disorders (phobias and anxiety disorders) affected twice as many women compared to men.
5. Alcohol use disorder in men was 4.6% amongst the 18+ population while illicit substance use disorders (dependence + abuse) was 0.6%
6. Less than 2% had a severe mental illness like psychosis or bipolar disorder. Amongst those with the disorder, nearly 50% had moderate to severe disability.
7. A growing concern has been the risk of suicide - 0.9% are at a high risk of suicide.
8. The economic impact of mental disorder is huge as the median monthly expenditure ranged between INR 1000 to 2500 and varied across conditions.
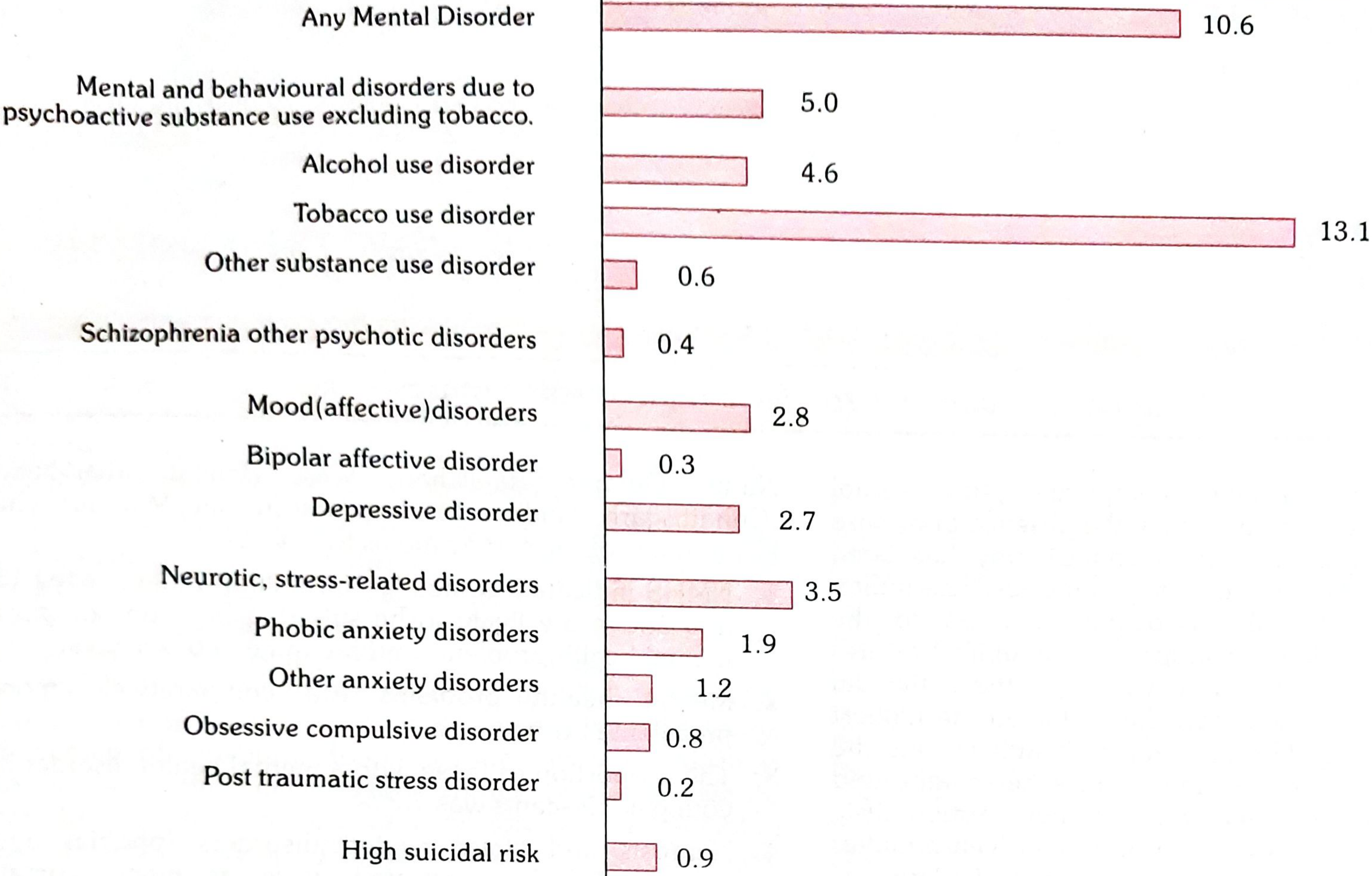
Based on uniform and standardized data collection procedures, mental morbidity of individuals above 18 years currently was 10.6%. The lifetime prevalence was 13.7%.
DIAGRAM - Prevalence of Mental Disorders in India (Park's Fig. 1)
Types of Mental Illness
Mental illness is a vast subject, broad in its limits and difficult to define precisely. There are major and minor illnesses.
The major illnesses are called PSYCHOSES. Here, the person is "insane" and out of touch with reality. There are three major illnesses:
(1) SCHIZOPHRENIA (split personality) - the patient lives in a dream world of his own.
(2) MANIC DEPRESSIVE PSYCHOSIS - symptoms vary from heights of excitement to depths of depression.
(3) PARANOIA - associated with undue and extreme suspicion and a progressive tendency to regard the whole world in a framework of delusions.
The minor illnesses are of two groups:
(a) NEUROSIS OR PSYCHONEUROSIS: The patient is unable to react normally to life situations. He is not considered "insane" by his associates, but nevertheless exhibits certain peculiar symptoms such as morbid fears, compulsions and obsessions.
(b) PERSONALITY AND CHARACTER DISORDERS: This group of disorders are the legacy of unfortunate childhood experiences and perceptions.
ICD-10 Classification of Mental & Behavioural Disorders
- Organic, including symptomatic, mental disorders - e.g., dementia in Alzheimer's disease, delirium
- Mental and behavioural disorders due to psychoactive substance use - e.g., harmful use of alcohol, opioid dependence syndrome
- Schizophrenia, schizotypal and delusional disorders - e.g., paranoid schizophrenia, delusional disorders, acute and transient psychotic disorders
- Mood (affective) disorders - e.g., bipolar affective disorder, depressive episode
- Neurotic, stress-related and somatoform disorders - e.g., generalized anxiety disorders, obsessive-compulsive disorders
- Behavioural syndromes associated with physiological disturbances - e.g., eating disorders, non-organic sleep disorders
- Disorders of adult personality and behaviour - e.g., paranoid personality disorder, trans-sexualism
- Mental retardation
- Disorders of psychological development
- Behavioural and emotional disorders with onset usually occurring in childhood - hyperkinetic disorders, conduct disorders, tic disorders
Causes of Mental Ill-Health
Mental illness like physical illness is due to multiple causes. Among the known factors:
(1) ORGANIC CONDITIONS: Mental illnesses may have their origin in organic conditions such as cerebral arteriosclerosis, neoplasms, metabolic diseases, neurological diseases, endocrine diseases and chronic diseases such as tuberculosis, leprosy, epilepsy, etc.
(2) HEREDITY: Heredity may be an important factor in some cases. For example, the child of two schizophrenic parents is 40 times more likely to develop schizophrenia than the child of healthy parents.
(3) SOCIAL PATHOLOGICAL CAUSES: The social and environmental factors associated with mental ill-health comprise: worries, anxieties, emotional stress, tension, frustration, unhappy marriages, broken homes, poverty, industrialization, urbanization, changing family structure, population mobility, economic insecurity, cruelty, rejection, neglect and the like.
Environmental factors other than psychosocial ones capable of producing abnormal human behaviour are:
- (1) Toxic substances - carbon disulfide, mercury, manganese, tin, lead compounds
- (2) Psychotropic drugs - barbiturates, alcohol, griseofulvin
- (3) Nutritional factors - deficiency of thiamine, pyridoxine
- (4) Minerals - deficiency of iodine
- (5) Infective agents - infectious disease (e.g., measles, rubella) during the prenatal, perinatal and post-natal periods
- (6) Traumatic factors - road and occupational accidents
- (7) Radiation - nervous system is most sensitive to radiation during the period of neural development
Burden of Mental Illness
Mental illness accounts for 11% of all years lived with disability globally, particularly for women. A recent study estimated the cumulative global impact of mental disorders in terms of lost economic output will amount to US$ 16.3 trillion between 2011 and 2030.
Mental disorders frequently lead individuals and families into poverty. Homelessness and inappropriate incarceration are far more common for people with mental disorders. Because of stigmatization and discrimination, persons with mental disorders often have their human rights violated.
Community Mental Health Services
Mental health services in a community are concerned not only with early diagnosis and treatment, but also with the preservation and promotion of good mental health and prevention of mental illness. The mental health services comprise:
(1) Early diagnosis and treatment
(2) Rehabilitation
(3) Group and individual psychotherapy
(4) Mental health education
(5) Use of modern psychoactive drugs
(6) After-care services
Comprehensive Community Mental Health Programme
Since 95% of psychiatric cases can be treated with or without hospitalization close to their homes, the current trend is full integration of psychiatric services with other health services.
The philosophy of Community Mental Health Programme consists of the following essential elements:
(1) In-patient services (2) Out-patient services (3) Partial hospitalization (4) Emergency services (5) Diagnostic services (6) Pre-care and after-care services including foster home placement and home visiting (7) Education services (8) Training, and (9) Research and evaluation.
Source: Park's Textbook of Preventive and Social Medicine - Mental Health chapter, pp. 537-539, 933-937