Show me the 10 most common heart disease with ecg pattern
ECG patterns common heart diseases electrocardiogram
ST elevation myocardial infarction STEMI ECG leads
atrial fibrillation ECG irregular rhythm no P waves
heart block complete AV block third degree ECG bradycardia
left ventricular hypertrophy ECG voltage criteria Sokolow
ventricular tachycardia wide QRS tachycardia ECG
pericarditis saddle-shaped ST elevation diffuse ECG
hypertrophic cardiomyopathy ECG deep Q waves LVH
pulmonary embolism ECG S1Q3T3 right heart strain sinus tachycardia
Wolff-Parkinson-White WPW delta wave short PR ECG pre-excitation
10 Common Heart Diseases & Their ECG Patterns
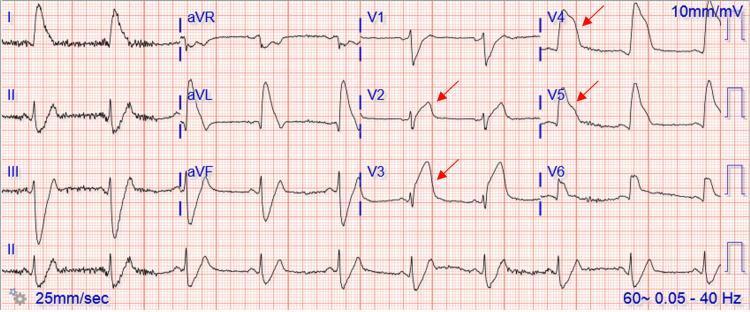
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
- ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads
- Hyperacute T waves (tall, peaked) in early phase
- Pathological Q waves (>40 ms wide, >25% of R-wave height) in evolved MI
- Reciprocal ST depression in opposing leads
- "Tombstone" morphology in severe proximal LAD occlusion
| Territory | Leads with ST Elevation | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | ST depression V1–V2 + tall R | RCA/LCx |
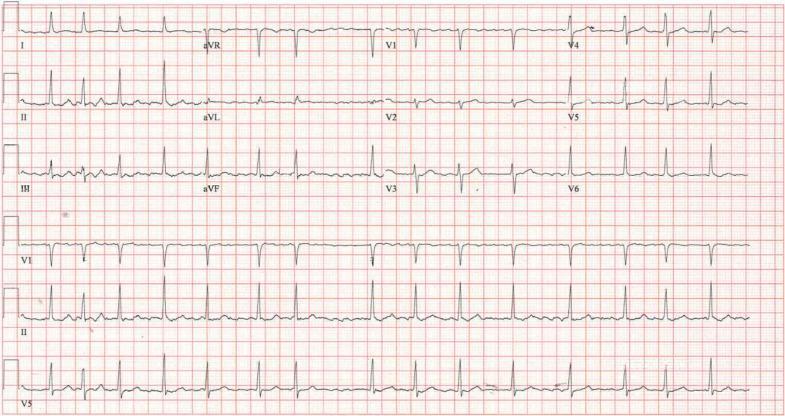
2. 🫀 Atrial Fibrillation (AF)
- Irregularly irregular R-R intervals — the hallmark
- Absent P waves replaced by fine/coarse fibrillatory (f) waves (best seen in V1)
- Narrow QRS complexes (unless aberrant conduction or bundle branch block)
- Rapid ventricular response if uncontrolled (>100 bpm)
3. 🫀 Complete (3rd-Degree) AV Heart Block
- AV dissociation — P waves and QRS complexes fire completely independently
- Atrial rate faster than ventricular rate
- Regular, slow ventricular escape rhythm (~20–40 bpm)
- Narrow QRS = nodal escape; Wide QRS = ventricular/infranodal escape
- No fixed PR interval
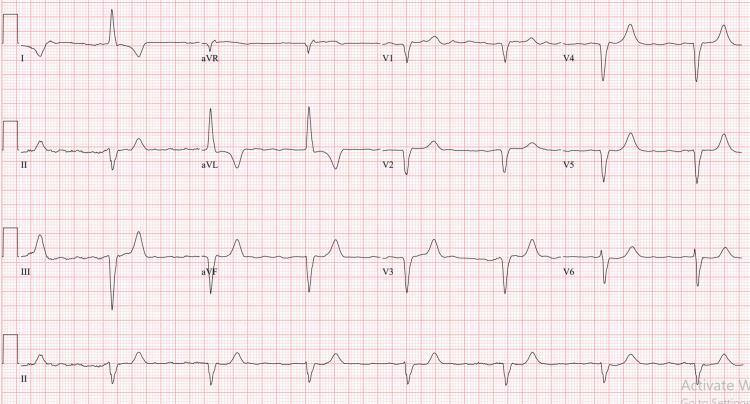
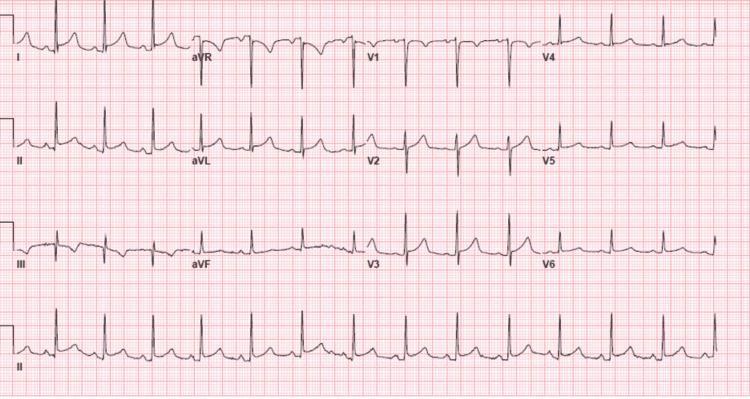
4. 🫀 Left Ventricular Hypertrophy (LVH) — Hypertensive Heart Disease
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men), >20 mm (women)
- LV strain pattern: ST depression + T-wave inversion in I, aVL, V5–V6
- Left axis deviation
- Broadened QRS (not always frank LBBB)
5. 🫀 Ventricular Tachycardia (VT)
- Wide QRS tachycardia (QRS >120 ms) at rate ≥100 bpm
- Regular or slightly irregular rhythm
- AV dissociation (P waves independent of QRS)
- Fusion beats and capture beats (pathognomonic)
- Concordance in precordial leads (all positive or all negative)
- Northwest/superior axis deviation
| Feature | Points toward VT |
|---|---|
| QRS >160 ms | ✓ |
| Positive concordance V1–V6 | ✓ |
| AV dissociation | ✓ (pathognomonic) |
| Brugada/Wellens criteria | ✓ |

6. 🫀 Acute Pericarditis
- Stage 1: Diffuse saddle-shaped (concave) ST elevation in almost all leads; PR depression; ST elevation in aVR absent or with PR elevation
- Stage 2: ST normalizes, T waves flatten
- Stage 3: Diffuse T-wave inversions
- Stage 4: Normalization
- Key differentiator from STEMI: Diffuse (not localised), no reciprocal changes except aVR, PR segment depression
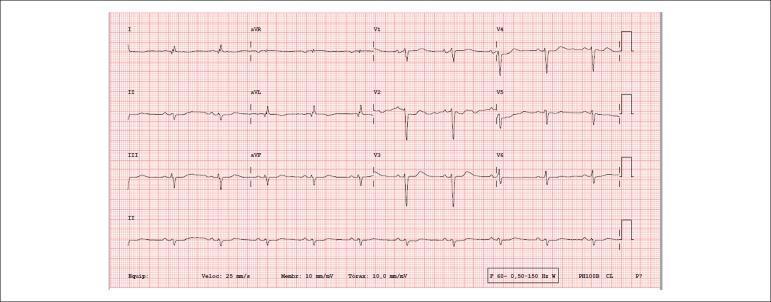
7. 🫀 Pulmonary Embolism (PE)
- Most common: Sinus tachycardia (non-specific)
- Classic S₁Q₃T₃ pattern: Deep S in I, Q wave in III, inverted T in III
- Right bundle branch block (complete or incomplete)
- T-wave inversions in V1–V4 (right ventricular strain)
- Right axis deviation
- P pulmonale (peaked P waves in II ≥2.5 mm)
- New AF in massive PE

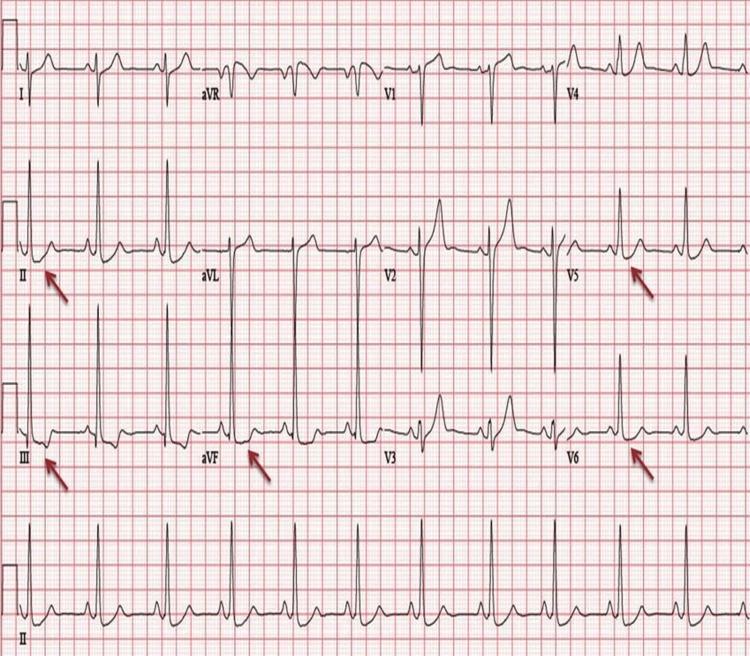
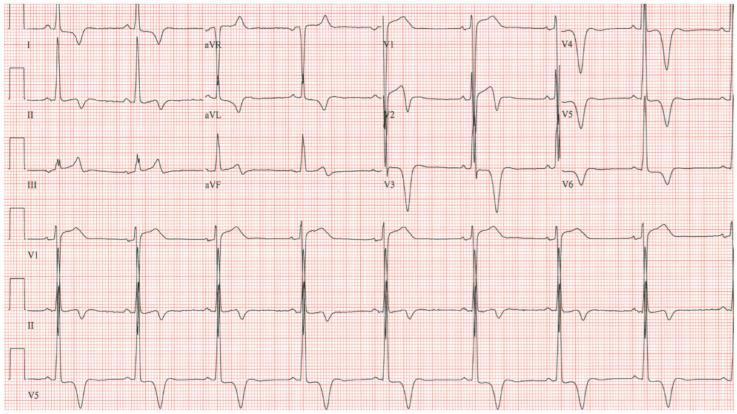
8. 🫀 Hypertrophic Cardiomyopathy (HCM)
- LVH voltage criteria (tall R in lateral leads, deep S in right leads)
- Deep narrow Q waves in lateral (I, aVL, V5–V6) and inferior leads — due to septal hypertrophy
- Apical HCM (Yamaguchi): Giant deep symmetric T-wave inversions in V3–V5 (≥10 mm depth)
- ST depression in lateral leads
- Left axis deviation
- AF occurs in 20–25% of patients
9. 🫀 Wolff-Parkinson-White (WPW) Syndrome
- Short PR interval (<120 ms)
- Delta wave — slurred initial upstroke of QRS
- Widened QRS (>120 ms) due to pre-excitation
- Secondary ST-T changes discordant with delta wave direction
- Risk: can precipitate AF → rapid conduction via accessory pathway → VF
| Pathway Location | Delta Polarity |
|---|---|
| Left lateral | Negative in V1, positive in I |
| Posteroseptal | Negative in II, III, aVF |
| Anteroseptal | Positive in V1 |

10. 🫀 Dilated Cardiomyopathy (DCM)
- Left bundle branch block (LBBB) — most characteristic
- QRS ≥120 ms, broad notched R in I/aVL/V5–V6, deep S/QS in V1–V3
- Diffuse ST-T changes (secondary to LBBB or ischaemia)
- Left axis deviation
- AF is common (30–40%)
- Low voltage QRS (if severe fibrosis or pericardial effusion co-exists)
- P mitrale (broad bifid P waves in II) — left atrial enlargement
- Pseudo-infarction Q waves mimicking prior MI
Quick Reference Summary
| # | Condition | Key ECG Finding |
|---|---|---|
| 1 | STEMI | ST elevation, Q waves, reciprocal depression |
| 2 | Atrial Fibrillation | Irregularly irregular, no P waves |
| 3 | Complete Heart Block | AV dissociation, slow escape rhythm |
| 4 | LVH / HTN Heart Disease | High voltage + strain pattern |
| 5 | Ventricular Tachycardia | Wide QRS ≥120 ms, AV dissociation |
| 6 | Acute Pericarditis | Diffuse saddle ST elevation, PR depression |
| 7 | Pulmonary Embolism | Sinus tachycardia, S₁Q₃T₃, RV strain |
| 8 | Hypertrophic Cardiomyopathy | Giant T inversions, deep Q waves |
| 9 | WPW Syndrome | Short PR, delta wave, widened QRS |
| 10 | Dilated Cardiomyopathy | LBBB, AF, low voltage |
Sources: Braunwald's Heart Disease (Elsevier), ROSEN's Emergency Medicine; ECG images from peer-reviewed clinical literature via PMC.
Convert this information into pdf
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not foun…
mkdir -p /home/daytona/workspace/ecg-guide && python3 -c "from reportlab.lib.pag…
~/ecg-guide/generate_pdf.py
import requests
import os
from io import BytesIO
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm, cm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Image, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.platypus.flowables import BalancedColumns
from reportlab.graphics.shapes import Drawing, Rect
from reportlab.pdfgen import canvas
OUTPUT_PATH = "/home/daytona/workspace/ecg-guide/Heart_Diseases_ECG_Guide.pdf"
# ─── Colour palette ────────────────────────────────────────────────────────────
DARK_RED = colors.HexColor("#8B0000")
MED_RED = colors.HexColor("#C0392B")
LIGHT_RED = colors.HexColor("#FADBD8")
DARK_GREY = colors.HexColor("#2C3E50")
MID_GREY = colors.HexColor("#5D6D7E")
LIGHT_GREY = colors.HexColor("#EAF0FB")
TABLE_HDR = colors.HexColor("#1A3A5C")
TABLE_ALT = colors.HexColor("#EBF5FB")
WHITE = colors.white
BLACK = colors.black
# ─── ECG Data ──────────────────────────────────────────────────────────────────
DISEASES = [
{
"num": 1,
"name": "ST-Elevation Myocardial Infarction (STEMI)",
"icon": "❤",
"key_findings": [
"ST elevation ≥1 mm in ≥2 contiguous limb leads; ≥2 mm in precordial leads",
"Hyperacute T waves (tall, peaked) in early phase",
"Pathological Q waves (>40 ms, >25% R height) in evolved MI",
"Reciprocal ST depression in opposing leads",
'"Tombstone" morphology in proximal LAD occlusion',
],
"table": {
"headers": ["Territory", "Leads", "Artery"],
"rows": [
["Anterior", "V1–V4", "LAD"],
["Inferior", "II, III, aVF", "RCA"],
["Lateral", "I, aVL, V5–V6", "LCx"],
["Posterior", "ST↓ V1–V2 + tall R", "RCA/LCx"],
]
},
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_0f5964997b5f333f6a7b13ecdc70a73ef6e81127eaee03ef38d9c724b26bbf31.jpg",
"img_caption": "Anterior STEMI — tombstone ST elevation V2–V5 with reciprocal inferior depression",
},
{
"num": 2,
"name": "Atrial Fibrillation (AF)",
"icon": "❤",
"key_findings": [
"Irregularly irregular R-R intervals — the hallmark",
"Absent P waves replaced by fine/coarse fibrillatory (f) waves (best in V1)",
"Narrow QRS complexes unless aberrant conduction or BBB",
"Rapid ventricular response if uncontrolled (>100 bpm)",
],
"table": None,
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_a8e7a35a18d282cc6de8c169a0213a6712f9fe9e4a7253f7828e22c867033097.jpg",
"img_caption": "AF — irregularly irregular rhythm, absent P waves, fine fibrillatory baseline",
},
{
"num": 3,
"name": "Complete (3rd-Degree) AV Heart Block",
"icon": "❤",
"key_findings": [
"AV dissociation — P waves and QRS complexes fire independently",
"Atrial rate faster than ventricular rate",
"Regular, slow ventricular escape rhythm (~20–40 bpm)",
"Narrow QRS = nodal escape; Wide QRS = ventricular/infranodal escape",
"No fixed PR interval",
],
"table": None,
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_c76f7d8cf3869000720e9ce457857cf031f9b360704aa4236ad85275ba26169e.jpg",
"img_caption": "3rd-degree AV block — P waves march through independently of slow wide QRS escape",
},
{
"num": 4,
"name": "Left Ventricular Hypertrophy (LVH) — Hypertensive Heart Disease",
"icon": "❤",
"key_findings": [
"Sokolow-Lyon: S in V1 + R in V5/V6 ≥35 mm",
"Cornell: R in aVL + S in V3 >28 mm (men), >20 mm (women)",
"LV strain pattern: ST depression + T-wave inversion in I, aVL, V5–V6",
"Left axis deviation",
"Broadened QRS (not always frank LBBB)",
],
"table": None,
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_03152b722b1cb86ef1d57f4d755aa687989488df7da9defa36d7d35f9ab80e28.jpg",
"img_caption": "LVH with strain pattern — high voltage laterally with ST depression and T-wave inversions",
},
{
"num": 5,
"name": "Ventricular Tachycardia (VT)",
"icon": "❤",
"key_findings": [
"Wide QRS tachycardia (QRS >120 ms) at rate ≥100 bpm",
"Regular or slightly irregular rhythm",
"AV dissociation (P waves independent of QRS)",
"Fusion beats and capture beats (pathognomonic)",
"Concordance in precordial leads (all positive or all negative)",
"Northwest/superior axis deviation",
],
"table": {
"headers": ["Feature", "Points toward VT"],
"rows": [
["QRS >160 ms", "✓"],
["Positive concordance V1–V6", "✓"],
["AV dissociation", "✓ (pathognomonic)"],
["Brugada/Wellens criteria", "✓"],
]
},
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_d15a92de4e89b46f273b22d254d1e30fcd6a190c6d581b193e6dd338338c6bb6.jpg",
"img_caption": "Monomorphic VT — wide complex tachycardia with positive concordance, no P waves",
},
{
"num": 6,
"name": "Acute Pericarditis",
"icon": "❤",
"key_findings": [
"Stage 1: Diffuse saddle-shaped (concave) ST elevation + PR depression",
"Stage 2: ST normalises, T waves flatten",
"Stage 3: Diffuse T-wave inversions",
"Stage 4: Full normalisation",
"Key differentiator from STEMI: diffuse, no territory, PR depression present",
],
"table": None,
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_0be5b02bdb0710f3bd3fcdbdc88b2944c0c2c3f7e84ae335cad7b36d24ffb97c.jpg",
"img_caption": "Acute pericarditis — diffuse saddle-shaped ST elevation + PR depression across multiple leads",
},
{
"num": 7,
"name": "Pulmonary Embolism (PE)",
"icon": "❤",
"key_findings": [
"Most common: Sinus tachycardia (non-specific but sensitive)",
"Classic S₁Q₃T₃ pattern: deep S in I, Q wave in III, inverted T in III",
"Right bundle branch block (complete or incomplete)",
"T-wave inversions in V1–V4 (right ventricular strain)",
"Right axis deviation; P pulmonale (peaked P ≥2.5 mm in II)",
"New AF in massive PE",
],
"table": None,
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_7cfb4819f88c84d02f863ca2f948165b6f4f6fafd405ca0b0a7df41e2d8d8e2a.jpg",
"img_caption": "Pulmonary embolism — sinus tachycardia, S1Q3T3 pattern, RV strain T inversions V1–V3",
},
{
"num": 8,
"name": "Hypertrophic Cardiomyopathy (HCM)",
"icon": "❤",
"key_findings": [
"LVH voltage criteria (tall R laterally, deep S right leads)",
"Deep narrow Q waves in lateral (I, aVL, V5–V6) and inferior leads",
"Apical HCM (Yamaguchi): giant deep symmetric T inversions in V3–V5 (≥10 mm)",
"ST depression in lateral leads",
"Left axis deviation; AF in 20–25% of patients",
],
"table": None,
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_3d2687643839a530919d460d4461031928da6585c23315b742b24d71296327a0.jpg",
"img_caption": "Apical HCM (Yamaguchi) — giant symmetric T-wave inversions reaching 15 mm depth in V2–V4",
},
{
"num": 9,
"name": "Wolff-Parkinson-White (WPW) Syndrome",
"icon": "❤",
"key_findings": [
"Short PR interval (<120 ms)",
"Delta wave — slurred initial upstroke of the QRS",
"Widened QRS (>120 ms) due to ventricular pre-excitation",
"Secondary ST-T changes discordant with delta wave direction",
"Risk: AF → rapid accessory pathway conduction → VF",
],
"table": {
"headers": ["Pathway Location", "Delta Polarity"],
"rows": [
["Left lateral", "Negative in V1, positive in I"],
["Posteroseptal", "Negative in II, III, aVF"],
["Anteroseptal", "Positive in V1"],
]
},
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_fd0d58cc1913acd56cbc62cbf42657e4a465f052a9bb2ea0d3893584ef6f70e6.jpg",
"img_caption": "WPW syndrome — short PR interval, prominent delta waves, widened QRS complexes",
},
{
"num": 10,
"name": "Dilated Cardiomyopathy (DCM)",
"icon": "❤",
"key_findings": [
"Left bundle branch block (LBBB) — most characteristic (QRS ≥120 ms)",
"Broad notched R in I/aVL/V5–V6; deep QS in V1–V3",
"Diffuse ST-T changes secondary to LBBB",
"Left axis deviation; AF common (30–40%)",
"Low voltage QRS (if fibrosis or pericardial effusion)",
"Pseudo-infarction Q waves mimicking prior MI",
],
"table": None,
"img_url": "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_3adea767053955d22dff275d5b4935c292277e5153fb88fae914ccff7abedb82.jpg",
"img_caption": "DCM/LBBB pattern — low voltage QRS, broad notched morphology, secondary ST-T changes",
},
]
SUMMARY_ROWS = [
["1", "STEMI", "ST elevation, Q waves, reciprocal depression"],
["2", "Atrial Fibrillation", "Irregularly irregular, no P waves"],
["3", "Complete Heart Block", "AV dissociation, slow escape rhythm"],
["4", "LVH / HTN Heart Disease", "High voltage + lateral strain pattern"],
["5", "Ventricular Tachycardia", "Wide QRS ≥120 ms, AV dissociation"],
["6", "Acute Pericarditis", "Diffuse saddle ST elevation, PR depression"],
["7", "Pulmonary Embolism", "Sinus tachycardia, S₁Q₃T₃, RV strain"],
["8", "Hypertrophic Cardiomyopathy", "Giant T inversions, deep Q waves"],
["9", "WPW Syndrome", "Short PR, delta wave, widened QRS"],
["10", "Dilated Cardiomyopathy", "LBBB, AF, low voltage"],
]
# ─── Helper: download image ─────────────────────────────────────────────────
def fetch_image_bytes(url, timeout=15):
try:
r = requests.get(url, timeout=timeout)
r.raise_for_status()
return BytesIO(r.content)
except Exception as e:
print(f" [WARN] Could not fetch {url}: {e}")
return None
# ─── Page template with header/footer ──────────────────────────────────────
def make_canvas_callback(title_text):
def on_page(canv, doc):
canv.saveState()
w, h = A4
# Header bar
canv.setFillColor(DARK_RED)
canv.rect(0, h - 22*mm, w, 22*mm, fill=1, stroke=0)
canv.setFont("Helvetica-Bold", 11)
canv.setFillColor(WHITE)
canv.drawString(15*mm, h - 14*mm, title_text)
canv.setFont("Helvetica", 9)
canv.drawRightString(w - 15*mm, h - 14*mm, "Clinical ECG Reference Guide")
# Footer bar
canv.setFillColor(DARK_GREY)
canv.rect(0, 0, w, 12*mm, fill=1, stroke=0)
canv.setFont("Helvetica", 8)
canv.setFillColor(WHITE)
canv.drawString(15*mm, 4*mm, "Source: Braunwald's Heart Disease | ROSEN's Emergency Medicine")
canv.drawRightString(w - 15*mm, 4*mm, f"Page {doc.page}")
canv.restoreState()
return on_page
# ─── Styles ─────────────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
title_style = ParagraphStyle(
"MainTitle", fontSize=28, fontName="Helvetica-Bold",
textColor=WHITE, alignment=TA_CENTER, spaceAfter=6
)
subtitle_style = ParagraphStyle(
"Subtitle", fontSize=14, fontName="Helvetica",
textColor=colors.HexColor("#FADBD8"), alignment=TA_CENTER, spaceAfter=4
)
disease_title_style = ParagraphStyle(
"DiseaseTitle", fontSize=15, fontName="Helvetica-Bold",
textColor=WHITE, alignment=TA_LEFT, spaceAfter=0, leading=18
)
section_num_style = ParagraphStyle(
"SectionNum", fontSize=30, fontName="Helvetica-Bold",
textColor=colors.HexColor("#FADBD8"), alignment=TA_LEFT
)
bullet_style = ParagraphStyle(
"Bullet", fontSize=9.5, fontName="Helvetica",
textColor=DARK_GREY, leftIndent=12, bulletIndent=0,
spaceAfter=3, leading=13
)
caption_style = ParagraphStyle(
"Caption", fontSize=8, fontName="Helvetica-Oblique",
textColor=MID_GREY, alignment=TA_CENTER, spaceAfter=4
)
body_style = ParagraphStyle(
"Body", fontSize=9.5, fontName="Helvetica",
textColor=DARK_GREY, spaceAfter=4, leading=13
)
table_hdr_style = ParagraphStyle(
"TblHdr", fontSize=9, fontName="Helvetica-Bold",
textColor=WHITE, alignment=TA_CENTER
)
table_cell_style = ParagraphStyle(
"TblCell", fontSize=9, fontName="Helvetica",
textColor=DARK_GREY, alignment=TA_LEFT
)
summary_hdr_style = ParagraphStyle(
"SumHdr", fontSize=10, fontName="Helvetica-Bold",
textColor=WHITE, alignment=TA_CENTER
)
summary_cell_style = ParagraphStyle(
"SumCell", fontSize=9, fontName="Helvetica",
textColor=DARK_GREY
)
# ─── Build ───────────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUTPUT_PATH,
pagesize=A4,
leftMargin=18*mm, rightMargin=18*mm,
topMargin=30*mm, bottomMargin=20*mm,
title="10 Common Heart Diseases & ECG Patterns",
author="Orris Medical Reference",
)
story = []
PAGE_W = A4[0] - 36*mm # usable width
# ════════════════════ COVER PAGE ════════════════════════════════════════════
# Big coloured cover block drawn via a custom flowable trick —
# we use a table with coloured background instead.
cover_title_style = ParagraphStyle(
"CoverTitle", fontSize=32, fontName="Helvetica-Bold",
textColor=WHITE, alignment=TA_CENTER, leading=38, spaceAfter=8
)
cover_sub_style = ParagraphStyle(
"CoverSub", fontSize=14, fontName="Helvetica",
textColor=colors.HexColor("#FADBD8"), alignment=TA_CENTER, spaceAfter=6
)
cover_body_style = ParagraphStyle(
"CoverBody", fontSize=11, fontName="Helvetica",
textColor=colors.HexColor("#D5E8F5"), alignment=TA_CENTER, spaceAfter=4
)
cover_content = [
[Paragraph("10 Common Heart Diseases", cover_title_style)],
[Paragraph("& Their ECG Patterns", cover_title_style)],
[Spacer(1, 8*mm)],
[Paragraph("A Clinical Reference Guide", cover_sub_style)],
[Spacer(1, 6*mm)],
[Paragraph(
"STEMI • Atrial Fibrillation • Heart Block • LVH • VT<br/>"
"Pericarditis • Pulmonary Embolism • HCM • WPW • DCM",
cover_body_style)],
[Spacer(1, 10*mm)],
[Paragraph("Source: Braunwald's Heart Disease | ROSEN's Emergency Medicine", ParagraphStyle(
"src", fontSize=9, textColor=colors.HexColor("#A9CCE3"), alignment=TA_CENTER
))],
]
cover_table = Table(cover_content, colWidths=[PAGE_W])
cover_table.setStyle(TableStyle([
("BACKGROUND", (0, 0), (-1, -1), DARK_RED),
("TOPPADDING", (0, 0), (-1, -1), 8),
("BOTTOMPADDING", (0, 0), (-1, -1), 8),
("LEFTPADDING", (0, 0), (-1, -1), 20),
("RIGHTPADDING", (0, 0), (-1, -1), 20),
("VALIGN", (0, 0), (-1, -1), "MIDDLE"),
("ROWBACKGROUNDS",(0, 0), (-1, -1), [DARK_RED]),
]))
# Outer wrapper to add a red box that fills most of the page
story.append(Spacer(1, 25*mm))
story.append(cover_table)
story.append(Spacer(1, 12*mm))
intro_style = ParagraphStyle(
"Intro", fontSize=10, fontName="Helvetica",
textColor=DARK_GREY, alignment=TA_JUSTIFY, leading=15
)
story.append(Paragraph(
"Electrocardiography remains the fastest, most accessible, and most widely used tool in cardiovascular "
"diagnosis. This guide presents the 10 most clinically encountered heart diseases alongside their "
"characteristic ECG patterns, diagnostic criteria, and representative tracings sourced from peer-reviewed "
"clinical literature. Each section includes key findings, localisation tables where applicable, and an "
"annotated 12-lead ECG image.",
intro_style
))
story.append(PageBreak())
# ════════════════════ DISEASE SECTIONS ══════════════════════════════════════
for d in DISEASES:
print(f"Building section {d['num']}: {d['name']} ...")
# ── Section header bar ──────────────────────────────────────────────────
num_para = Paragraph(f"{d['num']:02d}", ParagraphStyle(
"Num", fontSize=36, fontName="Helvetica-Bold",
textColor=colors.HexColor("#FADBD8"), alignment=TA_LEFT
))
name_para = Paragraph(d["name"], disease_title_style)
header_data = [[num_para, name_para]]
header_table = Table(header_data, colWidths=[22*mm, PAGE_W - 22*mm])
header_table.setStyle(TableStyle([
("BACKGROUND", (0, 0), (-1, -1), DARK_RED),
("VALIGN", (0, 0), (-1, -1), "MIDDLE"),
("LEFTPADDING", (0, 0), (0, 0), 6),
("LEFTPADDING", (1, 0), (1, 0), 4),
("RIGHTPADDING", (0, 0), (-1, -1), 8),
("TOPPADDING", (0, 0), (-1, -1), 6),
("BOTTOMPADDING", (0, 0), (-1, -1), 6),
("ROUNDEDCORNERS",(0, 0), (-1, -1), [4, 4, 4, 4]),
]))
# ── Key findings ────────────────────────────────────────────────────────
findings_paras = [Paragraph("<b>Key ECG Findings</b>", ParagraphStyle(
"FH", fontSize=10, fontName="Helvetica-Bold",
textColor=DARK_RED, spaceAfter=4
))]
for f in d["key_findings"]:
findings_paras.append(Paragraph(f"• {f}", bullet_style))
# ── Optional table ──────────────────────────────────────────────────────
tbl_element = None
if d["table"]:
td = d["table"]
t_data = [[Paragraph(h, table_hdr_style) for h in td["headers"]]]
for i, row in enumerate(td["rows"]):
bg = TABLE_ALT if i % 2 == 0 else WHITE
t_data.append([Paragraph(cell, table_cell_style) for cell in row])
col_count = len(td["headers"])
col_w = PAGE_W / col_count
tbl = Table(t_data, colWidths=[col_w] * col_count)
tbl.setStyle(TableStyle([
("BACKGROUND", (0, 0), (-1, 0), TABLE_HDR),
("ROWBACKGROUNDS",(0, 1), (-1, -1), [TABLE_ALT, WHITE]),
("GRID", (0, 0), (-1, -1), 0.5, colors.HexColor("#BFC9CA")),
("TOPPADDING", (0, 0), (-1, -1), 4),
("BOTTOMPADDING", (0, 0), (-1, -1), 4),
("LEFTPADDING", (0, 0), (-1, -1), 6),
("RIGHTPADDING", (0, 0), (-1, -1), 6),
("VALIGN", (0, 0), (-1, -1), "MIDDLE"),
]))
tbl_element = tbl
# ── ECG Image ────────────────────────────────────────────────────────────
img_bytes = fetch_image_bytes(d["img_url"])
img_element = None
if img_bytes:
img_max_w = PAGE_W
img_max_h = 55*mm
img_element = Image(img_bytes, width=img_max_w, height=img_max_h)
img_element.hAlign = "CENTER"
# ── Assemble section ────────────────────────────────────────────────────
section_parts = [
header_table,
Spacer(1, 4*mm),
]
section_parts.extend(findings_paras)
if tbl_element:
section_parts.append(Spacer(1, 3*mm))
section_parts.append(tbl_element)
if img_element:
section_parts.append(Spacer(1, 5*mm))
section_parts.append(img_element)
section_parts.append(Paragraph(d["img_caption"], caption_style))
section_parts.append(HRFlowable(width=PAGE_W, thickness=0.5, color=colors.HexColor("#BFC9CA")))
section_parts.append(Spacer(1, 6*mm))
story.extend(section_parts)
# Page break after every 2 diseases to keep layout clean
if d["num"] % 2 == 0 and d["num"] < 10:
story.append(PageBreak())
# ════════════════════ SUMMARY TABLE PAGE ════════════════════════════════════
story.append(PageBreak())
story.append(Paragraph("Quick Reference Summary", ParagraphStyle(
"SumTitle", fontSize=18, fontName="Helvetica-Bold",
textColor=DARK_RED, spaceAfter=8, alignment=TA_CENTER
)))
story.append(HRFlowable(width=PAGE_W, thickness=2, color=DARK_RED))
story.append(Spacer(1, 4*mm))
sum_data = [[
Paragraph("#", summary_hdr_style),
Paragraph("Condition", summary_hdr_style),
Paragraph("Hallmark ECG Finding", summary_hdr_style),
]]
for row in SUMMARY_ROWS:
sum_data.append([
Paragraph(row[0], ParagraphStyle("SC", fontSize=10, fontName="Helvetica-Bold",
textColor=DARK_RED, alignment=TA_CENTER)),
Paragraph(row[1], summary_cell_style),
Paragraph(row[2], summary_cell_style),
])
sum_table = Table(sum_data, colWidths=[12*mm, 65*mm, PAGE_W - 77*mm])
sum_table.setStyle(TableStyle([
("BACKGROUND", (0, 0), (-1, 0), TABLE_HDR),
("ROWBACKGROUNDS",(0, 1), (-1, -1), [TABLE_ALT, WHITE]),
("GRID", (0, 0), (-1, -1), 0.5, colors.HexColor("#BFC9CA")),
("TOPPADDING", (0, 0), (-1, -1), 6),
("BOTTOMPADDING", (0, 0), (-1, -1), 6),
("LEFTPADDING", (0, 0), (-1, -1), 8),
("RIGHTPADDING", (0, 0), (-1, -1), 8),
("VALIGN", (0, 0), (-1, -1), "MIDDLE"),
("FONTSIZE", (0, 1), (-1, -1), 9.5),
]))
story.append(sum_table)
story.append(Spacer(1, 10*mm))
story.append(Paragraph(
"<b>Sources:</b> Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine (Elsevier, 10th ed.) | "
"ROSEN's Emergency Medicine: Concepts and Clinical Practice (Elsevier) | "
"ECG images sourced from peer-reviewed PMC clinical literature.",
ParagraphStyle("Sources", fontSize=8, textColor=MID_GREY, leading=12, alignment=TA_JUSTIFY)
))
# ─── Build PDF ───────────────────────────────────────────────────────────────
doc.build(
story,
onFirstPage=make_canvas_callback("10 Common Heart Diseases & ECG Patterns"),
onLaterPages=make_canvas_callback("10 Common Heart Diseases & ECG Patterns"),
)
print(f"\n✓ PDF saved to: {OUTPUT_PATH}")
cd /home/daytona/workspace/ecg-guide && python3 generate_pdf.py 2>&1
ls -lh /home/daytona/workspace/ecg-guide/Heart_Diseases_ECG_Guide.pdf
Heart Diseases ECG Guide
PDF Document · PDF
- Cover page with title and condition list on a deep red background
- 10 individual sections, each with:
- Numbered header bar (red)
- Bullet-point key ECG findings
- Localisation/criteria table (where applicable — STEMI, VT, WPW)
- Full-width real 12-lead ECG image from peer-reviewed clinical literature
- Annotated caption describing the ECG
- Quick Reference Summary table at the end listing all 10 conditions and their hallmark ECG finding
- Running header and page footer with source attribution on every page