Enumerate and describe the types of Reed Sternberg cells with well labelled diagram 2nd yr mbbs refer harsh mohan
Reading File
Finding Sources
Finding Sources
Searching Images
Reed Sternberg cells types Hodgkin lymphoma
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Searching Images
lymphocytic histiocytic L&H popcorn cells lymphocyte predominance Hodgkin
Finding Sources
Loading Image
Reading File
Loading Image
Excellent! I now have the key textbook figure (Fig. 13.25 from Robbins) and all the information needed. Let me now compile a comprehensive, exam-ready answer for a 2nd year MBBS student in the style of Harsh Mohan's Textbook of Pathology.
Reed-Sternberg (RS) Cells — Types and Descriptions
(Reference: Harsh Mohan, Textbook of Pathology, 8th ed.; Robbins & Cotran Pathologic Basis of Disease)
What is a Reed-Sternberg Cell?
Reed-Sternberg (RS) cells are the pathognomonic neoplastic cells of Hodgkin Lymphoma (HL). They are derived from germinal centre B lymphocytes (confirmed by clonal IGH gene rearrangements and somatic hypermutation).
Basic features of classic RS cells:
- Large cells (~45 μm in diameter)
- Binucleated or bilobed nucleus, with mirror-image appearance
- Each nucleus contains a large, eosinophilic, inclusion-like nucleolus (5–7 μm — size of a small lymphocyte)
- Surrounded by a clear halo → "Owl-eye appearance" (the hallmark)
- Abundant pale cytoplasm
- Set against a background of lymphocytes, eosinophils, plasma cells, and macrophages
Immunophenotype (classic HL): CD30⁺, CD15⁺, PAX5 (weak)+, CD45⁻, CD20⁻
Types / Variants of Reed-Sternberg Cells
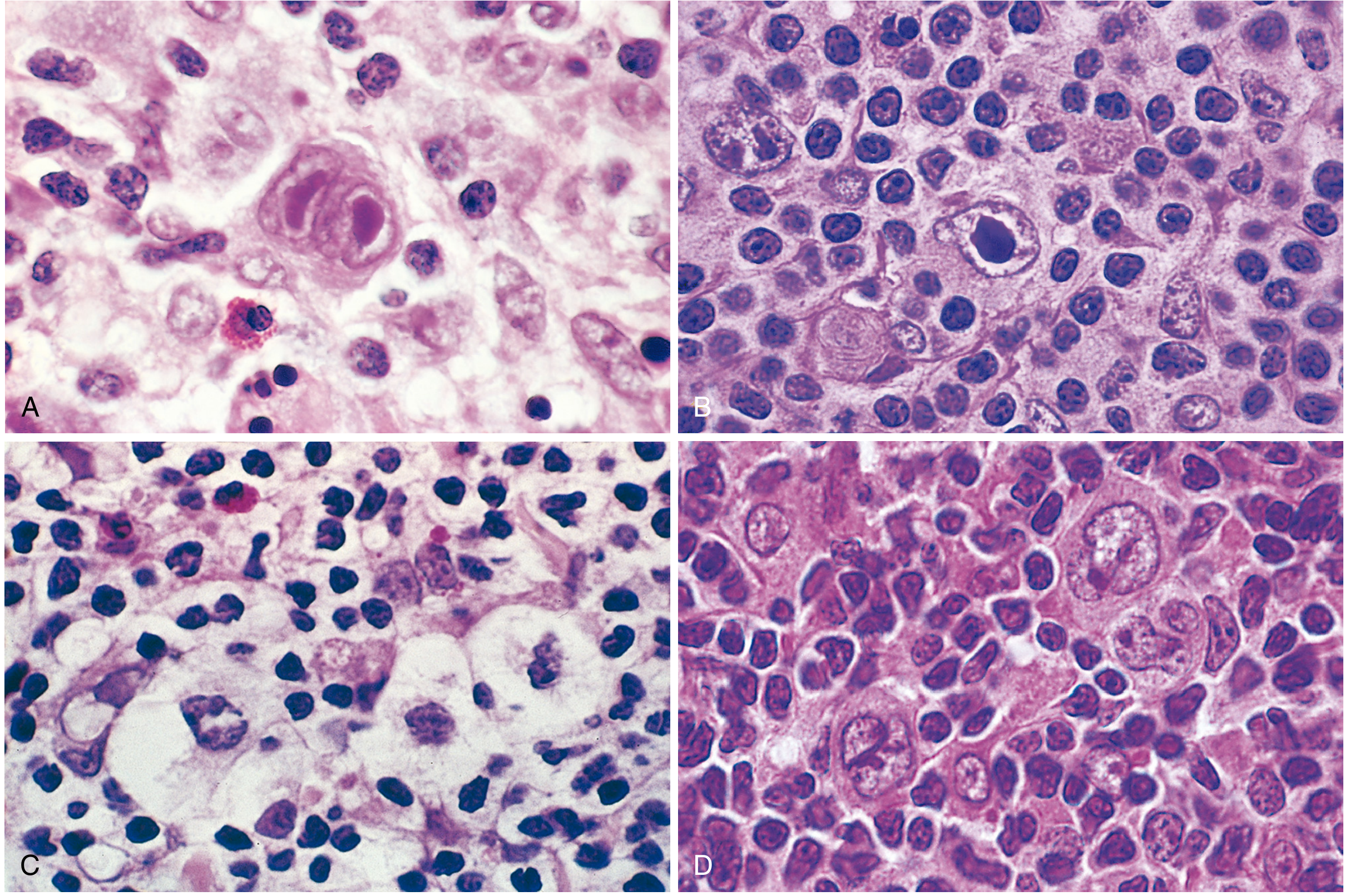
Fig. 13.25 (Robbins) — RS cells and variants. (A) Diagnostic RS cell (owl-eye, binucleate). (B) Mononuclear variant. (C) Lacunar variant (cell sitting in empty space/lacuna). (D) Lymphohistiocytic (L&H / popcorn) variants with multilobated nuclei and small nucleoli.
1. Classic (Diagnostic) RS Cell
| Feature | Detail |
|---|---|
| Nucleus | Binucleate or bilobed; mirror-image |
| Nucleolus | Large, prominent, eosinophilic — "inclusion-like" (5–7 μm); one per lobe → "Owl-eye" appearance |
| Cytoplasm | Abundant, pale eosinophilic |
| Size | ~45 μm |
| Background | Lymphocytes, eosinophils, plasma cells, macrophages |
| Subtype | Required for diagnosis in all classic HL subtypes |
| IHC | CD15⁺, CD30⁺, PAX5 weak+, CD45⁻ |
Key fact (Harsh Mohan): The classic RS cell is the sine qua non for diagnosing Hodgkin lymphoma. Its identification in an appropriate cellular background is mandatory for diagnosis.
2. Mononuclear Variant (Hodgkin Cell)
| Feature | Detail |
|---|---|
| Nucleus | Single nucleus (instead of two) |
| Nucleolus | One large, prominent, eosinophilic, inclusion-like nucleolus |
| Cytoplasm | Abundant |
| Morphology | Essentially half of a classic RS cell |
| Subtype | Common in Mixed Cellularity and Lymphocyte-Rich subtypes |
| Note | Also called "Hodgkin cell" |
3. Lacunar Variant
| Feature | Detail |
|---|---|
| Nucleus | Multilobated/folded; delicate nuclear membranes |
| Nucleolus | Small to inconspicuous (multiple small ones) |
| Cytoplasm | Abundant pale cytoplasm that retracts during formalin fixation, leaving the nucleus in an empty clear space = lacuna |
| Artifact | The "lacuna" (empty space) is a fixation artifact — NOT seen in B5-fixed specimens |
| Subtype | Characteristic of Nodular Sclerosis HL (most common subtype, 65–70%) |
| IHC | CD15⁺, CD30⁺ |
Mnemnonic tip: "Lacunar = Nodular Sclerosis" — the lacunar cell + collagen bands = nodular sclerosis pattern.
4. Lymphohistiocytic (L&H) Variant — "Popcorn Cell"
| Feature | Detail |
|---|---|
| Nucleus | Multilobated, polypoid/folded — resembles popcorn |
| Nucleolus | Multiple, small, basophilic (not the large eosinophilic nucleolus of classic RS) |
| Chromatin | Fine, vesicular |
| Cytoplasm | Moderately abundant, pale |
| Subtype | Characteristic of Nodular Lymphocyte-Predominant HL (NLPHL) |
| IHC | CD20⁺, CD45⁺, CD15⁻, CD30⁻ (opposite to classic HL!) |
| Background | B-cell rich nodules with follicular dendritic cells; T cells form rosettes around LP cells |
Key distinction: L&H cells express B-cell markers (CD20+) and are CD15⁻/CD30⁻, unlike all other RS variants. NLPHL has an indolent course and excellent prognosis.
5. "Mummified" (Pyknotic) RS Cell
| Feature | Detail |
|---|---|
| Nucleus | Pyknotic, shrunken, condensed chromatin |
| Cytoplasm | Deeply eosinophilic |
| Mechanism | A peculiar form of cell death seen in classic HL subtypes |
| Significance | Seen especially in Lymphocyte-Depleted HL |
Summary Table
| RS Cell Variant | Also Called | Nucleus | Nucleolus | Associated HL Subtype | CD15 | CD30 | CD20 |
|---|---|---|---|---|---|---|---|
| Classic RS cell | Diagnostic RS cell | Binucleate, owl-eye | Large, eosinophilic (×2) | All classic HL subtypes | ⊕ | ⊕ | ⊖ |
| Mononuclear | Hodgkin cell | Single nucleus | Large, eosinophilic (×1) | Mixed Cellularity, Lymphocyte-Rich | ⊕ | ⊕ | ⊖ |
| Lacunar | — | Multilobated, folded | Small/multiple | Nodular Sclerosis | ⊕ | ⊕ | ⊖ |
| L&H / Popcorn | Lymphohistiocytic | Polypoid, multifolded | Small, basophilic | Nodular Lymphocyte-Predominant | ⊖ | ⊖ | ⊕ |
| Mummified | Pyknotic RS cell | Pyknotic, condensed | Absent | Lymphocyte-Depleted | ⊕ | ⊕ | ⊖ |
Diagnostic Rule (Harsh Mohan)
Classic RS cells are necessary but NOT sufficient for diagnosis. They must be found in an appropriate reactive cellular background (lymphocytes, eosinophils, plasma cells). RS-like cells occur in:
- Infectious mononucleosis
- Non-Hodgkin lymphomas (especially ALCL)
- Solid tissue carcinomas (mimics)
Immunohistochemistry (CD15, CD30, CD20, CD45, PAX5) is used to confirm when morphology is uncertain.
Sources: Robbins, Cotran & Kumar — Pathologic Basis of Disease, Fig. 13.25 & Table 13.8 (corresponds to Harsh Mohan's classification of RS cell types in the Lymph Nodes chapter).
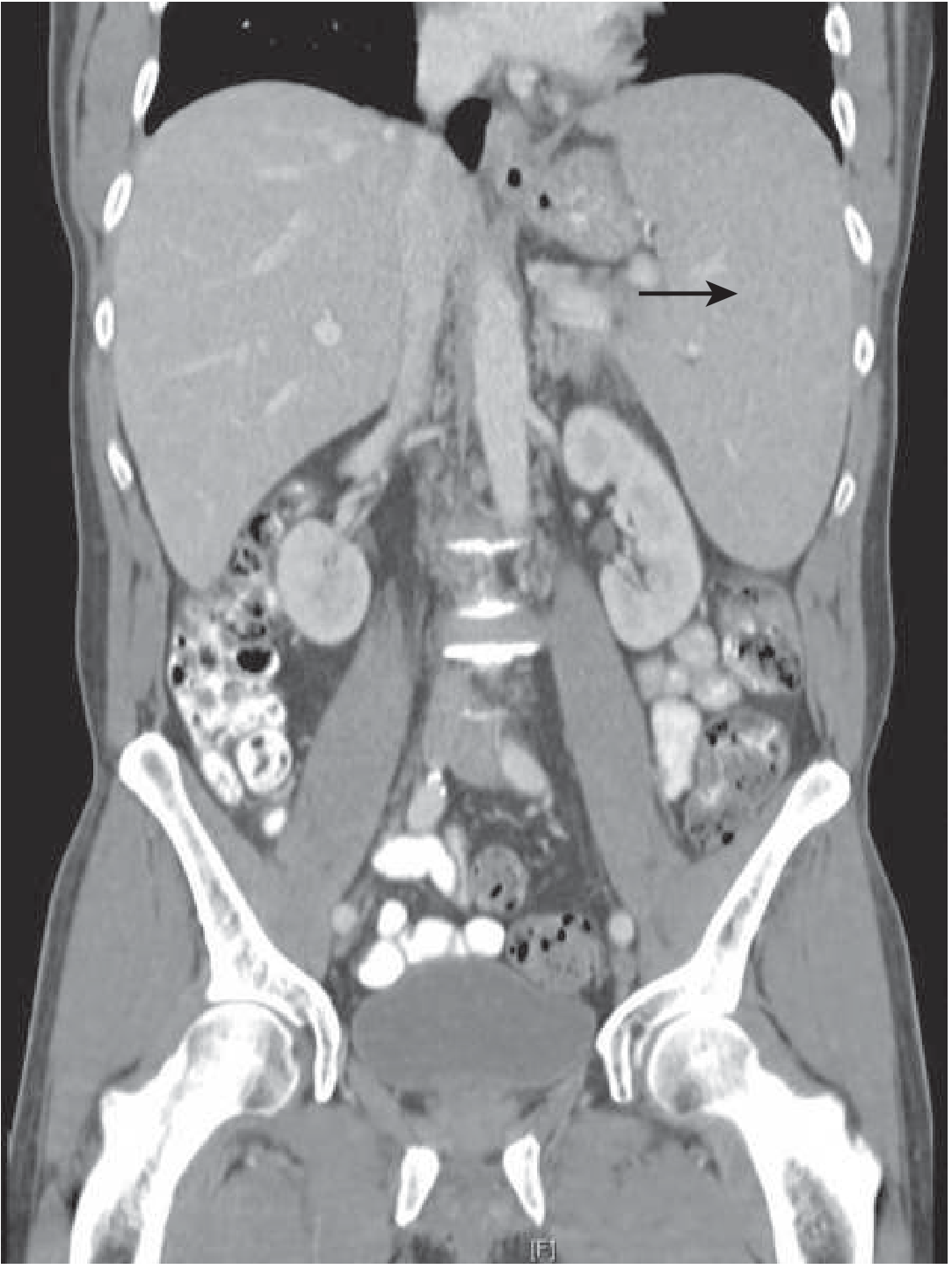
Splenomegaly
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching Images
splenomegaly gross pathology enlarged spleen
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive data from Robbins, Goldman-Cecil, and Harrison's. Let me compile the full, exam-ready answer in Harsh Mohan style.
Splenomegaly — Complete Overview
(Refs: Harsh Mohan Textbook of Pathology; Robbins & Cotran Pathologic Basis of Disease; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine)
Definition
Splenomegaly = enlargement of the spleen beyond its normal weight (>250 g in adults; normal 150 g). The spleen is the largest lymphoid organ in the body and functions as a filter, immune organ, and blood reservoir.
Normal Spleen at a Glance
| Parameter | Normal |
|---|---|
| Weight | ~150 g (range 100–250 g) |
| Size (USG) | < 13 cm length, < 5 cm thickness |
| Enlarged on USG | ≥13 cm length OR ≥5 cm thickness |
Classification / Causes of Splenomegaly
Splenomegaly can be classified by mechanism (as per Harsh Mohan) or by aetiology:
A. By Mechanism
| Mechanism | Examples |
|---|---|
| 1. Hyperplasia of lymphoid/phagocytic cells | Infections, haemolytic anaemias, immune disorders |
| 2. Congestion (vascular) | Portal hypertension (cirrhosis), cardiac failure, portal/splenic vein thrombosis |
| 3. Infiltration | Leukaemia, lymphoma, myeloproliferative disorders, storage diseases |
| 4. Extramedullary haematopoiesis | Myelofibrosis, thalassaemia major |
| 5. Space-occupying lesions | Cysts, abscesses, haemangiomas |
B. By Aetiology (Table — Robbins Table 13.12 / Goldman-Cecil Table 154-5)
🔴 Infections
| Category | Specific Causes |
|---|---|
| Bacterial | Infective endocarditis, typhoid fever, brucellosis, tuberculosis, syphilis |
| Viral | Infectious mononucleosis (EBV) ← most common acute cause in young adults; CMV, HIV |
| Parasitic | Malaria ← most common cause worldwide; Kala-azar (Leishmaniasis) ← massive splenomegaly; schistosomiasis, trypanosomiasis, toxoplasmosis |
| Fungal | Histoplasmosis |
🔵 Congestive (Portal Hypertension)
- Cirrhosis of liver ← commonest cause of massive congestive splenomegaly (Banti's syndrome)
- Portal vein thrombosis / pylephlebitis
- Splenic vein thrombosis (carcinoma stomach/pancreas)
- Cardiac failure (tricuspid/pulmonary valve disease, cor pulmonale)
- Schistosomiasis ("pipestem" hepatic fibrosis)
🟡 Lympho-haematogenous Disorders
- Hodgkin lymphoma, Non-Hodgkin lymphomas
- CLL, CML, ALL, AML
- Hairy cell leukaemia
- Multiple myeloma
- Myeloproliferative neoplasms (polycythaemia vera, essential thrombocythaemia, myelofibrosis — classically massive)
- Haemolytic anaemias: hereditary spherocytosis, sickle cell disease (early), thalassaemia
🟢 Immune-mediated / Autoimmune
- Rheumatoid arthritis (Felty syndrome)
- SLE
- Autoimmune haemolytic anaemia
- Drug reaction (e.g. phenytoin)
🟣 Storage & Infiltrative Disorders
- Gaucher disease ← most common storage disorder causing splenomegaly
- Niemann-Pick disease
- Amyloidosis
- Sarcoidosis
- Thyrotoxicosis
⚫ Other / Structural
- Splenic cysts (primary/echinococcal)
- Haemangioma (most common primary splenic tumour)
Grades of Splenomegaly (Clinical / Harsh Mohan)
| Grade | Palpability | Common Causes |
|---|---|---|
| Mild | Just palpable to 4 cm below costal margin | Infections (EBV, typhoid), cardiac failure |
| Moderate | 4–8 cm below costal margin | Cirrhosis, haematological disorders |
| Massive (Giant) | Crossing midline / into pelvis | Kala-azar, CML, Myelofibrosis, Malaria (hyperreactive), Gaucher disease, Schistosomiasis |
Massive splenomegaly mnemonic — "KMMGS": Kala-azar, Malaria (tropical/hyperreactive), Myelofibrosis, Gaucher disease, Schistosomiasis (+ CML, thalassaemia major)
Pathology / Morphology
1. Nonspecific Acute Splenitis (Infections)
- Gross: Enlarged (200–400 g), soft, congested (tense capsule)
- Micro: Acute congestion of red pulp; encroachment on white pulp follicles; neutrophils, plasma cells, eosinophils; rarely abscess formation
- Can occur with any blood-borne infection

2. Congestive Splenomegaly (Banti's Syndrome)
- Gross: Markedly enlarged (1000–5000 g); firm; thickened fibrous capsule
- Micro (early): Red pulp congestion
- Micro (late): Progressive fibrosis; collagen deposited in sinusoidal walls; sinusoids appear dilated and rigid; Gamma-Gandy bodies (haemosiderin + calcium + fibrous tissue deposits = "siderotic nodules") — characteristic
- Prolonged exposure of blood cells to macrophages → hypersplenism
3. Splenic Infarcts
- Pale, wedge-shaped, subcapsular infarcts
- Overlying fibrinous capsular exudate
- Septic infarcts (suppurative necrosis) in infective endocarditis

Clinical Features
| Symptom/Sign | Mechanism |
|---|---|
| Dragging sensation / LUQ discomfort | Direct mass effect |
| Early satiety | Gastric compression |
| Left shoulder pain | Diaphragmatic irritation (splenic infarct / perisplenitis) |
| Anaemia, leucopenia, thrombocytopenia | Hypersplenism (sequestration + phagocytosis) |
| Spontaneous rupture | Massive enlargement (CML, EBV mononucleosis) |
| Palpable mass — LUQ | Enlarges downward and medially, notch palpable |
Distinguishing Splenic Mass from Other Masses
- Enlarges downward and to the right (toward right iliac fossa)
- Has a notch on medial/inferior border
- Cannot get above the mass (not bimanually palpable like kidney)
- Moves with respiration
- Dull to percussion (unlike retroperitoneal masses)
Hypersplenism
A clinical syndrome that may complicate any cause of splenomegaly:
| Criteria (all 4 required) |
|---|
| 1. Splenomegaly |
| 2. Cytopenia (anaemia ± thrombocytopenia ± leucopenia) |
| 3. Compensatory bone marrow hyperplasia |
| 4. Correction after splenectomy |
Mechanism: Sequestration + prolonged red pulp transit → phagocytosis of formed elements by macrophages.
Investigations
| Investigation | Purpose |
|---|---|
| USG abdomen | First-line; measures size; ≥13 cm = enlarged |
| CT abdomen | Detailed anatomy; detects diffuse vs nodular enlargement; portal vein assessment |
| CBC + peripheral smear | Cytopenias (hypersplenism); abnormal lymphocytes (lymphoma/leukaemia); malarial parasites; Howell-Jolly bodies (splenic dysfunction) |
| LFTs + coagulation profile | Liver disease / portal hypertension |
| Bone marrow biopsy | Haematological malignancies, myelofibrosis, storage diseases |
| Flow cytometry | Lymphoma/leukaemia immunophenotyping |
| Serology / cultures | Infectious causes (EBV, Leishmania, malaria thick smear) |
| LDH, uric acid | Lymphoma (Burkitt's, DLBCL) |
| FDG-PET | Limited role — does NOT distinguish causes |
| Splenic biopsy / splenectomy | Last resort (high bleeding risk) |
Summary Box (Exam-Ready)
| Feature | Detail |
|---|---|
| Normal weight | 150 g |
| Enlarged | >250 g (USG: >13 cm) |
| Commonest worldwide | Malaria |
| Commonest in India | Malaria / Kala-azar |
| Massive splenomegaly | Kala-azar, CML, Myelofibrosis, Gaucher, Schistosomiasis, Malaria |
| Congestive — #1 cause | Cirrhosis (Banti's syndrome) |
| Characteristic micro finding in congestion | Gamma-Gandy bodies (siderotic nodules) |
| Complication of any splenomegaly | Hypersplenism → pancytopenia |
| Acute splenitis weight | 200–400 g, soft |
| Massive congestive splenomegaly weight | 1000–5000 g, firm |
Sources: Robbins & Cotran Pathologic Basis of Disease, Table 13.12, pp. 573–574; Goldman-Cecil Medicine, Table 154-5; Harrison's Principles of Internal Medicine, 22e; Harsh Mohan — Textbook of Pathology, Chapter on Lymph Nodes and Spleen.
Sle
Finding Sources
Finding Sources
Searching Images
systemic lupus erythematosus butterfly rash malar rash clinical features
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.