glaucoma management for ophthalmology resident doctor
Reading File
Finding Sources
Searching PubMed
"glaucoma"[MeSH Terms] AND "management"[tiab]
Finding Sources
Searching PubMed
"open angle glaucoma"[MeSH Terms] AND "intraocular pressure"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive material to write a thorough, resident-level glaucoma management guide. Let me compile it.
Glaucoma Management - Ophthalmology Resident Guide
Based primarily on Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
1. Definition and Goal of Treatment
Glaucoma is a group of conditions sharing a chronic progressive optic neuropathy characterized by retinal ganglion cell death, retinal nerve fibre layer (RNFL) thinning, structural optic nerve head changes, and characteristic visual field loss. IOP is the key modifiable risk factor.
The goal of glaucoma treatment is to slow the rate of progression throughout a patient's lifetime in order to maintain visual function and related quality of life, at a sustainable cost. Treatment does not cure - it arrests or delays further damage.
2. Classification
| Category | Examples |
|---|---|
| Primary open-angle | POAG, NTG |
| Primary angle-closure | PAC suspect, PAC, PACG |
| Secondary open-angle | Pseudoexfoliation, pigmentary, steroid-induced, neovascular (pre-trabecular) |
| Secondary angle-closure | Neovascular (post-trabecular), uveitic, phacomorphic, malignant |
| Developmental | Primary congenital, secondary (aniridia, Sturge-Weber) |
3. Primary Open-Angle Glaucoma (POAG)
Risk Factors
- IOP: The higher the IOP, the greater the risk. Asymmetry ≥4 mmHg is significant.
- Age: More common with advancing age.
- Race: 4x more prevalent in Black individuals; earlier onset and harder to control.
- Family history: 4x risk to siblings, 2x risk to offspring.
- Myopia: Associated with increased incidence and susceptibility.
- CCT: Thin central corneal thickness is an independent risk factor.
- Optic disc area: Larger discs are more vulnerable.
- Anti-VEGF therapy: Recurrent intravitreal injections (especially bevacizumab) may cause sustained IOP elevation.
- Genetics: MYOC gene (myocilin) and OPTN gene (optineurin) mutations; polygenic risk scoring is emerging.
Pathogenesis of Optic Neuropathy
Retinal ganglion cell death occurs predominantly via apoptosis (not necrosis). The preterminal event is calcium ion influx with increased intracellular nitric oxide. Glutamine metabolism dysregulation and local ischaemia at the lamina cribrosa are central. Damage occurs at the optic nerve head level.
Natural History (EMGT Data)
Without treatment, mean annual VF deterioration:
- High-tension glaucoma (HTG): -1.31 dB/year
- Normal-tension glaucoma (NTG): -0.36 dB/year
- Pseudoexfoliation glaucoma: -3.13 dB/year (most aggressive)
On average, untreated glaucoma progresses from normal to blindness over ~25 years, but individual variation is large.
4. Optic Disc Assessment
Glaucomatous Disc Changes
Classic structural subtypes:
- Focal ischaemic - inferior notch (most common)
- Myopic - temporal crescent with inferior NRR loss
- Sclerotic - superior shelving and inferior notching
- Concentric - deep uniform cup enlargement
ISNT Rule: Normal rim follows Inferior > Superior > Nasal > Temporal thickness. Violation suggests glaucoma.
Neuroretinal rim (NRR) changes:
- Notching (focal thinning) - most significant
- Thinning of inferior or superior poles first
- Vertical C/D ratio enlargement (C/D >0.7 or asymmetry >0.2 is suspicious)
Non-specific signs:
- Disc haemorrhage (Drance haemorrhage) - risk factor for progression; don't miss it without magnification
- Baring of circumlinear vessels - early NRR thinning
- Bayoneting of vessels - double angulation from NRR loss
- Laminar dot sign - exposed lamina cribrosa fenestrations in advancing glaucoma
- RNFL defects - wedge-shaped, best seen by red-free photography
5. Visual Field Defects
Standard automated perimetry (SAP) with 24-2 or 30-2 pattern is routine. Use 10-2 for central field monitoring in advanced disease.
Sequence of VF loss:
- Early: Small paracentral scotomas (often superonasal), increased response variability
- Nasal step - sensitivity difference above/below horizontal midline (bounded by the horizontal raphe)
- Temporal wedge (less common)
- Arcuate defect - coalescence of paracentral scotomas, 10-20° from fixation
- Ring scotoma - superior and inferior arcuates become continuous
- End-stage - small central island + temporal island
Hodapp-Parrish-Anderson minimal criteria (2 of 3 on consecutive tests):
- GHT (Glaucoma Hemifield Test) outside normal limits
- ≥3 non-edge points depressed on PSD at P<5%, at least one at P<1%
- Corrected PSD occurring in <5% of normal individuals
Staging: Early <-6 dB MD | Moderate -6 to -12 dB | Severe >-12 dB
6. Imaging in Glaucoma
- OCT (Optical Coherence Tomography): RNFL thickness, optic nerve head parameters, macular ganglion cell complex - essential for structural monitoring. Detects pre-perimetric loss.
- HRT (Heidelberg Retinal Tomography): 3D optic disc topography; Moorfields Regression Analysis
- GDx (Nerve Fibre Analyser): Scanning laser polarimetry for RNFL
- OCT Angiography: Emerging - detects reduced optic disc perfusion density in glaucoma
Serial imaging is increasingly standard of care. Pre-perimetric glaucoma = structural damage on imaging before VF loss develops.
7. IOP Measurement
- Goldmann applanation tonometry (GAT): Gold standard
- Correction for CCT: Readings are overestimated in thick corneas and underestimated in thin corneas (e.g. post-LASIK, corneal ectasia, low CCT in NTG patients)
- Diurnal curve / phasing: IOP fluctuation of >5 mmHg is significant; peak IOP often in the morning
- Target IOP: Individualized - typically aim for at least 20-30% reduction from baseline. AGIS data: <18 mmHg at all times significantly reduces progression risk.
8. Medical Therapy
Initial treatment is usually with one agent, typically a prostaglandin analogue or beta-blocker. Use lowest effective concentration and least frequent dosing.
Drug Classes
| Class | Agent | Mechanism | IOP Reduction | Key Side Effects |
|---|---|---|---|---|
| Prostaglandin analogues (PGA) | Latanoprost, bimatoprost, travoprost, tafluprost | Increase uveoscleral outflow | 25-35% | Iris hyperpigmentation, hypertrichosis, periocular fat atrophy (DUES), reactivate HSV keratitis |
| Beta-blockers | Timolol (non-selective), betaxolol (selective β1) | Reduce aqueous production | 20-25% | Bradycardia, bronchospasm (avoid in asthma/COPD); betaxolol preferred in NTG (some neuroprotective effect) |
| Alpha-2 agonists | Brimonidine, apraclonidine | Reduce aqueous production + increase uveoscleral outflow | 20-25% | Allergy (up to 20% with apraclonidine), CNS depression in infants (contraindicated <2 years), dry mouth, fatigue |
| Carbonic anhydrase inhibitors (topical) | Dorzolamide, brinzolamide | Reduce aqueous production | 15-20% | Bitter taste, sulfonamide allergy |
| CAIs (systemic) | Acetazolamide | Reduce aqueous production | 25-30% | Metabolic acidosis, renal stones, sulfonamide allergy, Steven-Johnson syndrome |
| Miotics | Pilocarpine | Open trabecular meshwork via ciliary muscle contraction | 15-25% | Miosis, brow ache, myopia, rarely retinal detachment |
| Rho kinase inhibitor | Netarsudil | Increase trabecular outflow + reduce episcleral venous pressure | 15-20% | Conjunctival hyperaemia, cornea verticillata |
| Fixed combinations | Xalacom (latanoprost/timolol), Cosopt (dorzolamide/timolol), etc. | Dual mechanism | Additive | Improves adherence |
Brimonidine: May have a neuroprotective effect beyond IOP reduction - relevant in NTG management.
PGAs are first-line for most patients (once-daily dosing, best IOP reduction). Beta-blockers are second-line or combined.
Review Protocol
- First review after starting: 4-8 weeks
- If satisfactory: reassess at 3-6 months
- If no response: switch the drug
- If partial response: add a second agent
- Leave 5 minutes between drops (prevent washout)
Causes of Treatment Failure
- Inappropriate (too high) target pressure
- Poor adherence (≥25% of patients)
- Wide diurnal IOP fluctuations
- Check that morning drops were taken before clinic visit
9. Laser Treatment
Selective Laser Trabeculoplasty (SLT)
- Selective photothermolysis of trabecular meshwork pigmented cells
- Suitable as first-line alternative to drops (LiGHT trial showed non-inferiority to medication as initial treatment)
- IOP reduction ~25-30%
- Repeatable (unlike ALT)
- Side effects: transient IOP spike, mild anterior uveitis
Argon Laser Trabeculoplasty (ALT)
- Thermal coagulation of trabecular meshwork
- Largely replaced by SLT
- Not easily repeatable
Laser Peripheral Iridotomy (LPI)
- Standard treatment for primary angle closure and prevention in fellow eye after APAC
- Creates alternative aqueous drainage route, bypasses pupillary block
- Nd:YAG laser (sometimes preceded by argon for pigmented irides)
- Prophylactic LPI in PAC suspects with narrow angles
Laser Iridoplasty (ALPI - Argon Laser Peripheral Iridoplasty)
- For plateau iris syndrome after LPI
- Burns peripheral iris stroma, contracting it away from trabeculum
Cyclodiode / Cyclophotocoagulation
- Destroys ciliary body epithelium to reduce aqueous production
- Used in refractory glaucoma, painful blind eyes, poor surgical candidates
- Risk: hypotony, phthisis bulbi
10. Surgical Treatment
Trabeculectomy
- Guarded filtration surgery - creates a fistula with scleral flap
- First-choice incisional procedure for POAG
- Antimetabolites: Mitomycin C (MMC) or 5-FU applied intraoperatively to reduce scarring (essential in higher-risk eyes)
- Target IOP post-op: typically low teens
Complications:
- Early: shallow AC, hypotony, choroidal effusion, bleb leak, encapsulated bleb
- Late: bleb-related endophthalmitis (0.5-1.5% lifetime risk), cataract, hypotony maculopathy, dysesthetic bleb
Recent evidence (PMID: 40404077, 2025): Trabeculectomy augmented with anti-VEGF improves surgical outcomes.
Glaucoma Drainage Devices (GDDs/Tubes)
- Tube shunts (Ahmed, Baerveldt, Molteno)
- Indicated when trabeculectomy has failed or is likely to fail (uveitic glaucoma, NVG, aniridic glaucoma, failed conjunctiva)
- Provide best long-term IOP control in complex cases
- Tube-Versus-Trabeculectomy (TVT) Study: similar efficacy at 5 years, tubes had fewer re-operations
Minimally Invasive Glaucoma Surgery (MIGS)
- iStent, iStent Inject, Hydrus Microstent (Schlemm's canal)
- Kahook Dual Blade goniotomy, OMNI (ab interno trabeculotomy)
- XEN Gel Stent (subconjunctival drainage)
- CyPass Micro-Stent (supraciliary) - withdrawn due to corneal endothelial loss
- Best suited for mild-moderate glaucoma, often combined with cataract surgery
- Lower complication profile than trabeculectomy; more modest IOP reduction
11. Normal-Tension Glaucoma (NTG)
Definition
IOP consistently ≤21 mmHg on diurnal testing, with characteristic glaucomatous optic nerve damage and VF loss.
Key Differences from POAG
- IOP-independent vascular mechanisms are relatively more important
- Disc haemorrhages more frequent and associated with greater progression risk
- VF defects tend to be closer to fixation, deeper, steeper, and more localized
- More common in Japanese patients; more common in females; associated with migraine, Raynaud phenomenon, systemic hypotension
- Lower CCT on average than POAG
Treatment
- Prostaglandins are first-line
- Brimonidine may provide neuroprotection beyond IOP reduction (preferred over beta-blockers in NTG)
- Betaxolol (selective β1-blocker) preferred over timolol to avoid nocturnal BP dips
- SLT is a reasonable initial option
- Surgery when progression occurs despite IOP in low teens
- Control systemic vascular risk factors (diabetes, HTN, hyperlipidaemia)
- Systemic calcium-channel blockers to address vasospasm in selected cases
- Nocturnal hypotension: Reduce antihypertensive dose if large nocturnal BP dips detected; advise sleeping head-up 30° (reduces IOP ~20% in flat vs. 30° position in a third of patients)
- The Collaborative Normal-Tension Glaucoma Study showed 30% IOP reduction reduced progression rate
12. Primary Angle-Closure Glaucoma (PACG)
Gonioscopy - Shaffer Grading
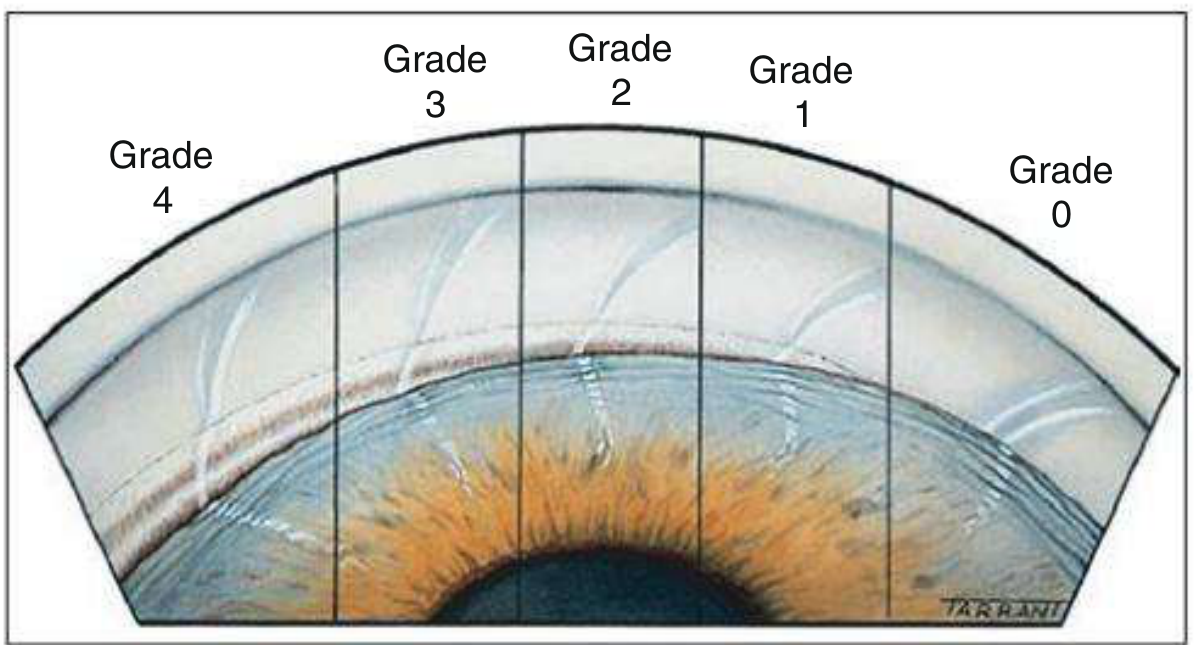
Fig. 11.31 - Shaffer grading of angle width (Kanski's Clinical Ophthalmology 10e)
| Grade | Degrees | Structures Visible | Risk |
|---|---|---|---|
| 4 | 35-45° | Ciliary body without lens tilt | Open |
| 3 | 25-35° | Scleral spur visible | Open |
| 2 | 20° | Trabeculum, no scleral spur | Potentially closeable |
| 1 | 10° | Schwalbe line ± top of trabeculum | Very narrow, high risk |
| 0 | 0° | Closed | Closed |
Van Herick method: Slit lamp estimate of AC depth vs. corneal thickness (ratio <1:4 = very narrow angle).
Classification
- PAC Suspect (PACS): Narrow angle on gonioscopy, no ITC, no PAS, normal IOP and disc
- Primary Angle Closure (PAC): ITC present, ± PAS or raised IOP, but no optic nerve damage
- Primary Angle-Closure Glaucoma (PACG): All of above + optic nerve/VF damage
Mechanisms
- Pupillary block (most common) - relative block at pupillary margin, aqueous diverts posteriorly, forward bowing of iris
- Plateau iris - anteriorly rotated ciliary processes, angle occlusion even after patent LPI
- Phacomorphic - large/intumescent lens pushes iris-lens diaphragm forward
- Malignant glaucoma (ciliolenticular block) - aqueous misdirected into vitreous cavity
Risk Factors
- Female sex, age ~62 at presentation
- Asian ethnicity (especially Far Eastern and South Asian)
- Hypermetropia, short axial length
- Positive family history
- Precipitants of acute attack: dim lighting, pharmacological mydriasis, parasympathetic antagonists, topiramate/sulfa drugs (ciliary body effusion), semi-prone position
Acute Primary Angle Closure (APAC) - Emergency Management
Symptoms: Severe unilateral eye pain, periocular headache, blurred vision, rainbow halos around lights, nausea/vomiting, abdominal pain.
Signs:
- IOP markedly elevated (often 50-80 mmHg)
- Conjunctival injection, corneal epithelial oedema
- Shallow AC, mid-dilated fixed pupil
- Glaukomflecken (anterior lens opacities)
Management Protocol:
- Patient lies supine (gravity encourages lens to shift posteriorly)
- Acetazolamide 500 mg IV if IOP >50 mmHg; oral if <50 mmHg (contraindicated: sulfonamide allergy, topiramate-induced attack)
- Single drops of: apraclonidine 0.5-1% + timolol 0.5% + prednisolone 1% / dexamethasone 0.1% (3-5 min apart)
- Pilocarpine 2% × 1-2 drops to affected eye (NOT if IOP >40 mmHg - ischaemia impairs action; also 1% to fellow eye prophylactically)
- Analgesia + antiemetic as needed
If resistant (IOP still high):
- Central corneal indentation with squint hook or goniolens (forces aqueous into angle)
- 50% topical glycerol to clear corneal oedema first
- IV mannitol 20% (1-2 g/kg over 1 hour) or oral glycerol 50% (1 g/kg) or oral isosorbide
- Early Nd:YAG iridotomy after clearing oedema (iridoplasty as alternative)
- Paracentesis as last resort
Definitive treatment: Bilateral laser peripheral iridotomy (fellow eye is at ~50% lifetime risk of APAC; prophylactic LPI recommended)
Post-attack signs: Residual corneal oedema, Descemet folds, glaukomflecken, spiral-shaped iris atrophy, dilated pupil, posterior synechiae, optic atrophy.
13. Secondary Glaucomas
Pseudoexfoliation Glaucoma (PXG)
- Most common secondary open-angle glaucoma worldwide
- PXF material (abnormal extracellular fibrillar material) clogs the TM
- Higher IOP, worse diurnal fluctuation, faster progression than POAG
- Responds well to SLT
- Associated with increased surgical complication risk (weak zonules - phacodonesis, capsular complications)
- Systemic: cardiovascular disease, dementia associations
Pigmentary Glaucoma
- Young myopic males
- Iris pigment (Krukenberg spindle on corneal endothelium) and heavy trabecular pigmentation
- Exercise or pupillary dilation can acutely spike IOP
- May spontaneously "burn out" as iris pigment depletes with age
- Laser iridotomy may reduce pigment dispersion (controversial)
- SLT very effective
Neovascular Glaucoma (NVG) - "100-Day Glaucoma"
- Caused by rubeosis iridis (iris neovascularization) from retinal ischaemia
- Main causes: ischaemic CRVO (35-50%), diabetes (10-15%), CRAO, ocular ischaemic syndrome
- Vessels at pupillary margin → iris surface → angle → fibrovascular membrane → angle closure
- Management:
- Anti-VEGF (intravitreal): Rapidly reduces neovascularization, buys time for definitive treatment
- Panretinal photocoagulation (PRP): Addresses ischaemic drive (definitive)
- IOP-lowering drops (cyclodestructive procedures or GDD when refractory)
- Trabeculectomy has poor outcomes; GDD preferred for surgical management
Steroid-Induced Glaucoma
- Topical > periocular > systemic > inhaled
- Posterior sub-Tenon's injections: prolonged risk (weeks-months after injection)
- Open-angle mechanism: steroid receptor activation reduces aqueous outflow through TM
- Managed by cessation/switching of steroid + standard IOP-lowering treatment
- May require surgery in resistant cases
Inflammatory (Uveitic) Glaucoma
- Mechanisms: trabeculitis/TM oedema (open-angle), PAS (angle-closure), seclusio pupillae and iris bombé (pupillary block), steroid effect
- Ciliary body shutdown in acute uveitis may mask underlying high IOP tendency
- Management: aggressive treatment of uveitis; use topical CAI or alpha-agonist (avoid prostaglandins - may worsen inflammation and CMO); cycloplegic to break posterior synechiae; LPI for iris bombé; surgery (trabeculectomy ± MMC or GDD) in refractory cases
Lens-Related Glaucoma
| Type | Mechanism |
|---|---|
| Phacolytic | Mature/hypermature cataract leaks high-MW proteins → TM macrophage clogging |
| Phacomorphic | Intumescent lens → pupillary block and angle closure |
| Phacoanaphylactic | Lens protein hypersensitivity |
| Lens particle | Fragments after trauma/surgery clog TM |
Treatment: Remove the lens (± LPI for phacomorphic).
14. Monitoring Protocol
| Parameter | Frequency |
|---|---|
| IOP | Every visit |
| Visual field (SAP 24-2) | Every 6-12 months if stable mild/moderate disease; more frequently if suspect progression |
| Optic disc examination | Every visit (photograph disc; note haemorrhages) |
| Serial OCT imaging | Standard of care; 6-12 monthly |
| Gonioscopy | Annually (angle narrows with age) |
Definitions of progression:
- VF: MD worsening >1 dB/year OR Pointwise regression
- Structure: OCT RNFL significant thinning outside normal limits on serial comparison
- Always correlate structural and functional data
If progressing despite target IOP achieved: Lower the target IOP further. Consider surgery.
15. Special Situations
Ocular Hypertension (OHT)
- IOP >21 mmHg without structural or functional damage
- OHTS data: 5-year risk of conversion to POAG ~10% untreated; treatment reduces this by 50%
- Treatment thresholds consider: IOP level, CCT (thin CCT dramatically increases risk), disc appearance, VF, age, race
Glaucoma Suspect
- Structural changes (suspicious disc, RNFL defect, OCT outside normal) WITHOUT VF loss = pre-perimetric glaucoma - treat or monitor closely
Glaucoma in Special Populations
- Children: Suspect congenital glaucoma if buphthalmos, epiphora, photophobia, Haab striae on cornea. IOP may be normal under GA. Treat surgically (goniotomy or trabeculotomy).
- Pregnancy: Avoid acetazolamide (teratogenic) and prostaglandins. Beta-blockers are relatively safe. Timolol may cause neonatal bradycardia.
- Pseudophakia: Capsular block syndrome, alpha-2 agonist still usable; prostaglandins are safe.
16. Key Clinical Trials to Know
| Trial | Key Message |
|---|---|
| OHTS | Treating OHT reduced 5-year conversion to POAG by ~50% |
| EMGT | Each mmHg IOP reduction reduces progression risk by ~10%; provided natural history data |
| AGIS | IOP consistently <18 mmHg prevents meaningful VF progression in most patients |
| CNTGS | 30% IOP reduction halves progression rate in NTG |
| LiGHT Trial | SLT as first-line is non-inferior to drops; 74% required no drops at 3 years |
| TVT Study | Tube surgery vs. trabeculectomy: similar efficacy at 5 years; tubes had fewer re-operations |
| AGIS (race subgroup) | Blacks had better outcomes with trabeculectomy first; Whites had better outcomes with laser first |
17. Practical Tips for Residents
- Always perform gonioscopy in a darkened room - PAC is more prevalent than previously realized.
- Disc haemorrhage = red flag - risk factor for progression; magnification essential.
- CCT must be measured in every glaucoma patient - it critically affects IOP interpretation and risk stratification.
- Poor adherence is ubiquitous (≥25%) - ask about drop technique, timing, and cost at every visit.
- Never rely on IOP alone - assess structure (disc, OCT) and function (VF) together.
- In NTG, look for nocturnal BP dips - advise head-up sleeping position and avoid bedtime beta-blockers.
- Anti-VEGF for NVG before any surgery - neovessels regress dramatically within days; reduces operative bleeding.
- Pilocarpine in APAC is withheld if IOP >40 mmHg - ischaemic iris sphincter won't respond.
- MIGS is for mild-moderate glaucoma combined with phaco - don't expect trabeculectomy-level IOP reduction.
- The worse the baseline damage, the lower the target IOP - progressive loss of ganglion cells means each remaining cell counts more.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition (ISBN 9780443110993) | PMID: 40404077 (trabeculectomy + anti-VEGF meta-analysis, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.