Tell me about goitre
Reading File
Finding Sources
Searching PubMed
goiter thyroid enlargement
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive, well-sourced material to write a detailed answer on goitre.
Goitre
Goitre refers to any enlargement of the thyroid gland, regardless of whether thyroid hormone levels are normal, elevated, or low. It is the most common anatomic disease of the thyroid, and the single most important cause worldwide is iodine deficiency. - Textbook of Family Medicine 9e
Pathophysiology
The central principle underlying goitre formation is that high levels of TSH (or substances acting like TSH) have a trophic (growth) effect on thyroid follicular cells, causing both hypertrophy and hyperplasia of the gland. - Costanzo Physiology 7e
This explains why goitre can appear in seemingly opposite thyroid states:
- Iodine deficiency: low T4/T3 → high TSH (negative feedback) → gland enlarges. The enlarged gland may still maintain euthyroid hormone levels if the stimulus is sufficient; if not, the patient becomes hypothyroid.
- Autoimmune (Hashimoto's) thyroiditis: antibodies impair thyroid peroxidase → low T4/T3 → high TSH → goitre, despite the gland failing to synthesize hormones effectively.
- Graves' disease: thyroid-stimulating immunoglobulins (TSI) act like TSH, driving both excess hormone production and glandular growth. TSH itself is suppressed by negative feedback, but the immunoglobulins provide the trophic stimulus.
- TSH-secreting pituitary adenoma: excess TSH drives both hyperthyroidism and goitre.
- Exogenous T4 ingestion: suppresses TSH → no goitre; gland can actually involute.
Classification
Bailey and Love's surgical classification of thyroid swellings is useful:
| Category | Type | Examples |
|---|---|---|
| Simple (euthyroid) | Diffuse hyperplastic | Physiological, pubertal, pregnancy |
| Multinodular | Endemic, sporadic | |
| Toxic | Diffuse | Graves' disease |
| Multinodular | Toxic MNG | |
| Solitary nodule | Toxic adenoma | |
| Neoplastic | Benign/Malignant | Adenoma, carcinoma |
| Inflammatory | Autoimmune | Hashimoto's, chronic lymphocytic thyroiditis |
| Granulomatous | de Quervain's thyroiditis | |
| Fibrosing | Riedel's thyroiditis | |
| Infective | Bacterial, viral, TB, syphilitic |
- Bailey and Love's Short Practice of Surgery 28e
Types in Detail
1. Simple (Non-Toxic) Goitre
A diffuse or nodular enlargement in a euthyroid patient. The most common cause globally is iodine deficiency (daily requirement: ~0.1-0.15 mg/day). Endemic areas include mountain ranges (Alps, Andes, Himalayas, Rocky Mountains) and inland lowlands far from sea (Great Lakes, Congo, Nile Valley, Derbyshire UK). Calcium is also goitrogenic - goitre is more common in chalk/limestone areas with low iodine.
Goitrogenic foods and drugs (goitrogens) that interfere with hormone synthesis can also cause simple goitre when iodine intake is marginal.
2. Multinodular Goitre (MNG)
Nodules develop as the gland undergoes uneven growth stimulation - some clones of thyroid cells appear particularly sensitive to growth factors and immunoglobulins beyond just TSH. - Bailey and Love 28e
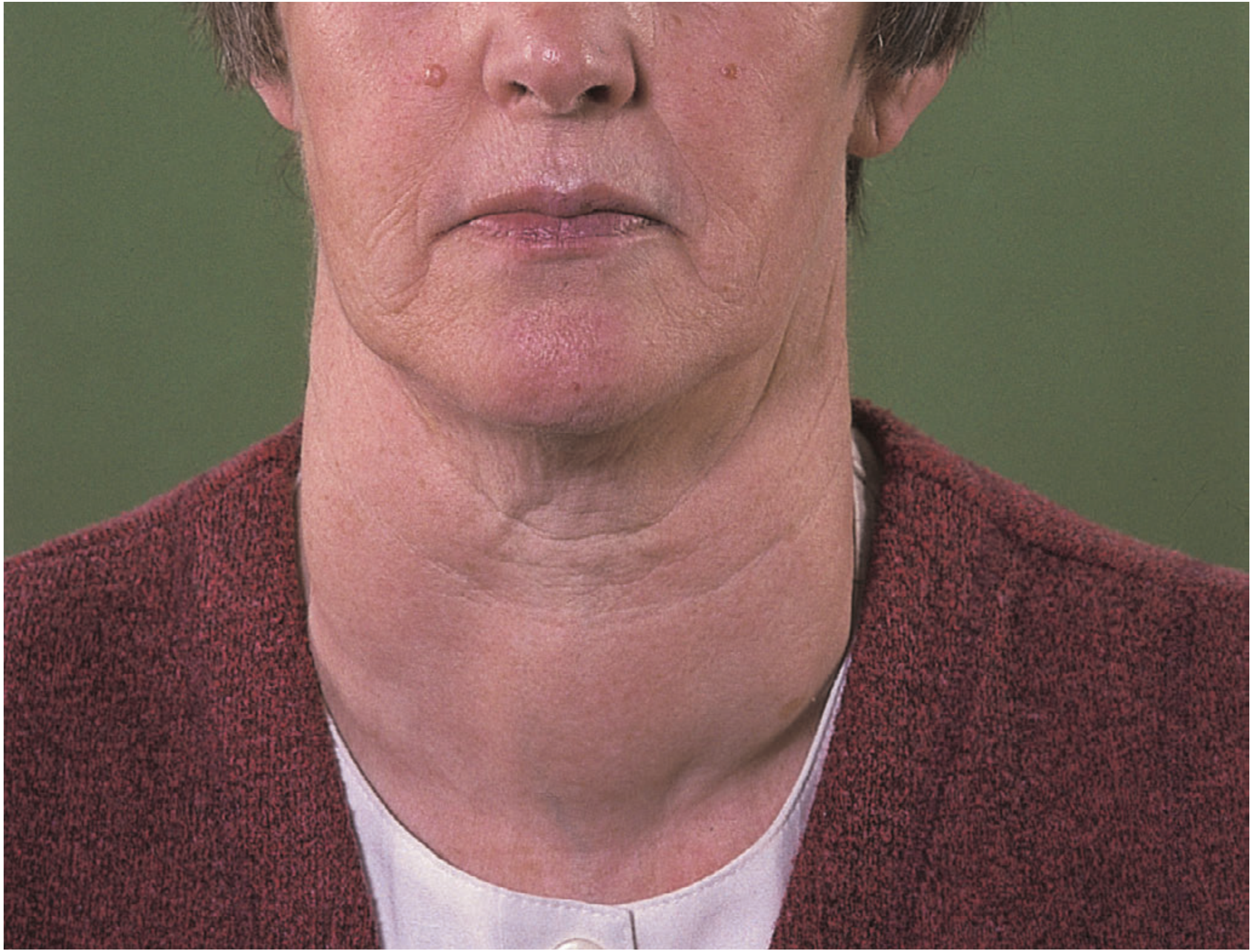
Colloid goitre (Bailey and Love's Surgery 28e)
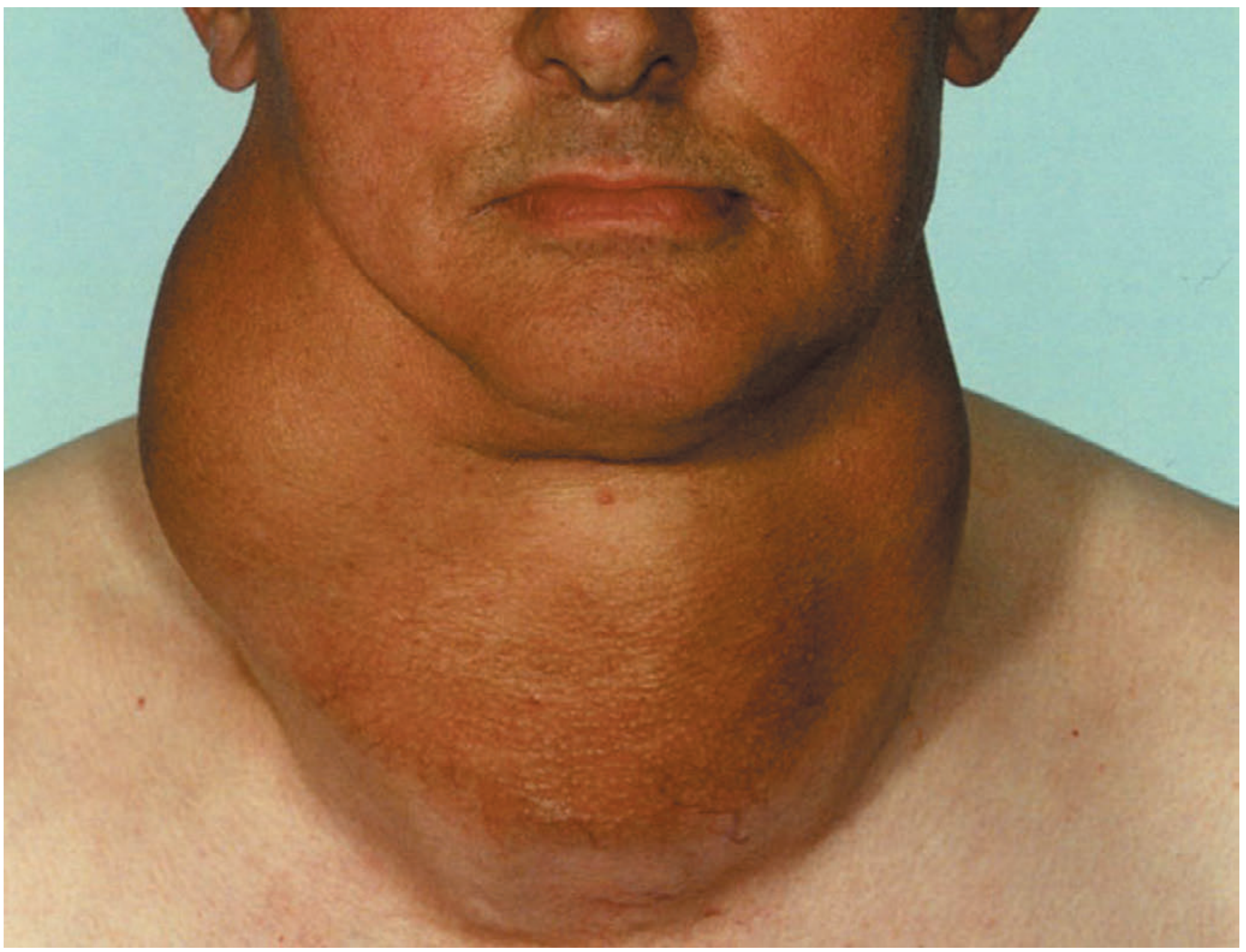
Large multinodular goitre (Bailey and Love's Surgery 28e)
Nodules appear early in endemic goitre but later (age 20-30 years) in sporadic goitre. The patient may be unaware until their 40s or 50s. All forms of simple goitre are more common in females due to oestrogen receptors in thyroid tissue.
3. Toxic Goitre
- Graves' disease: goitre occurs in nearly 100% of patients. It is one of the five hallmarks - the others being thyrotoxicosis, ophthalmopathy, pretibial myxedema, and acropachy (clubbing).
- Toxic MNG: episodes of mild hyperthyroidism occur in up to 30% of patients with MNG.
4. Retrosternal (Substernal) Goitre
Arises from slow inferior growth of a multinodular gland into the mediastinum. Pressure within the thoracic inlet causes dysphagia, tracheal compression, and airway symptoms. The vast majority of patients have minimal symptoms. More than 95% can be removed via a transcervical approach. - Bailey and Love 28e
Clinical Features
- Neck swelling that moves on swallowing (key diagnostic feature)
- Usually painless - sudden pain suggests haemorrhage into a nodule or rarely carcinoma
- Firm, smooth nodules; hardness/calcification may mimic carcinoma
- Pressure symptoms (larger goitres): dysphagia, hoarseness (recurrent laryngeal nerve compression), stridor, superior vena cava obstruction
- Thyroid status (hypo/eu/hyperthyroid) depends on underlying cause
Investigations
- Thyroid function tests (TSH, free T4, free T3) - to determine functional status
- Thyroid antibodies (anti-TPO, anti-Tg, TSI) - to differentiate autoimmune causes
- Ultrasound - gold standard for anatomical assessment; identifies nodules needing FNA
- Fine-needle aspiration cytology (FNAC) - for any sonographically suspicious nodule (not necessarily the dominant one)
- CT scan - when retrosternal extension, swallowing or breathing symptoms are present; assesses tracheal/oesophageal deviation
- Radioiodine scan - to identify hot (autonomous) vs. cold nodules
- Bailey and Love's Short Practice of Surgery 28e
Complications
- Tracheal obstruction - lateral displacement or anteroposterior compression, especially with retrosternal extension
- Acute airway compromise - haemorrhage into a nodule impacted at the thoracic inlet
- Secondary thyrotoxicosis - in up to 30% of MNG patients
- Malignant transformation - increased follicular carcinoma incidence in endemic areas; dominant or rapidly growing nodules should always have FNAC
Treatment
Prevention
- Iodised salt has strikingly reduced the incidence of endemic goitre worldwide.
Medical
- Early hyperplastic goitre: thyroxine 0.15-0.2 mg daily for several months may cause regression.
- Goitre with hypothyroidism: euthyroid doses of thyroxine often cause involution over 6-12 months. If it fails to involute, surgery may be needed.
- Note: once nodular change occurs, it is irreversible with medical therapy, although >50% of benign nodules regress spontaneously over 10 years.
Surgical Indications
- Suspected or confirmed malignancy
- Significant pressure symptoms (dysphagia, stridor)
- Retrosternal extension with airway compromise
- Cosmetic reasons
- Failed medical therapy
Surgical Options for MNG
| Approach | Advantage | Disadvantage |
|---|---|---|
| Total thyroidectomy | Definitive, no recurrence | Lifelong thyroxine, 5% risk permanent hypoparathyroidism |
| Subtotal thyroidectomy | May preserve function | Up to 5% recurrence risk; up to 100% failure by 30 years |
For Graves' disease specifically, current guidelines favour near-total or total thyroidectomy if surgery is chosen. - Scott-Brown's Otorhinolaryngology 2e
Radioiodine (I-131)
An alternative to surgery for toxic goitre in suitable patients (not pregnant, no large pressure symptoms), leading to gland reduction and correction of hyperthyroidism.
Key Points Summary
| Feature | Detail |
|---|---|
| Most common cause (global) | Iodine deficiency |
| Most common cause (iodine-sufficient areas, US) | Graves' disease / Hashimoto's thyroiditis |
| TSH role | High TSH = goitre; Low TSH = no goitre / involution |
| Female predominance | Due to oestrogen receptors on thyroid cells |
| Gold standard imaging | Ultrasound |
| First-line investigation | TSH |
| Surgery indication | Malignancy, pressure symptoms, retrosternal extension, cosmesis |
Sources: Bailey and Love's Short Practice of Surgery 28e; Costanzo Physiology 7e; Textbook of Family Medicine 9e; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.