Management of acute left ventricular failure
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute heart failure" AND management
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed to write a comprehensive, well-sourced answer. Let me compile it.
Management of Acute Left Ventricular Failure
Acute heart failure (AHF) / acute left ventricular failure (ALVF) is a life-threatening syndrome demanding rapid assessment and targeted therapy. The core goals are: relieve congestion and restore/maintain systemic perfusion.
1. Initial Assessment - Hemodynamic Profiling
The first step at the bedside is to classify the patient using the "wet/dry" and "warm/cold" framework, which directly guides therapy:
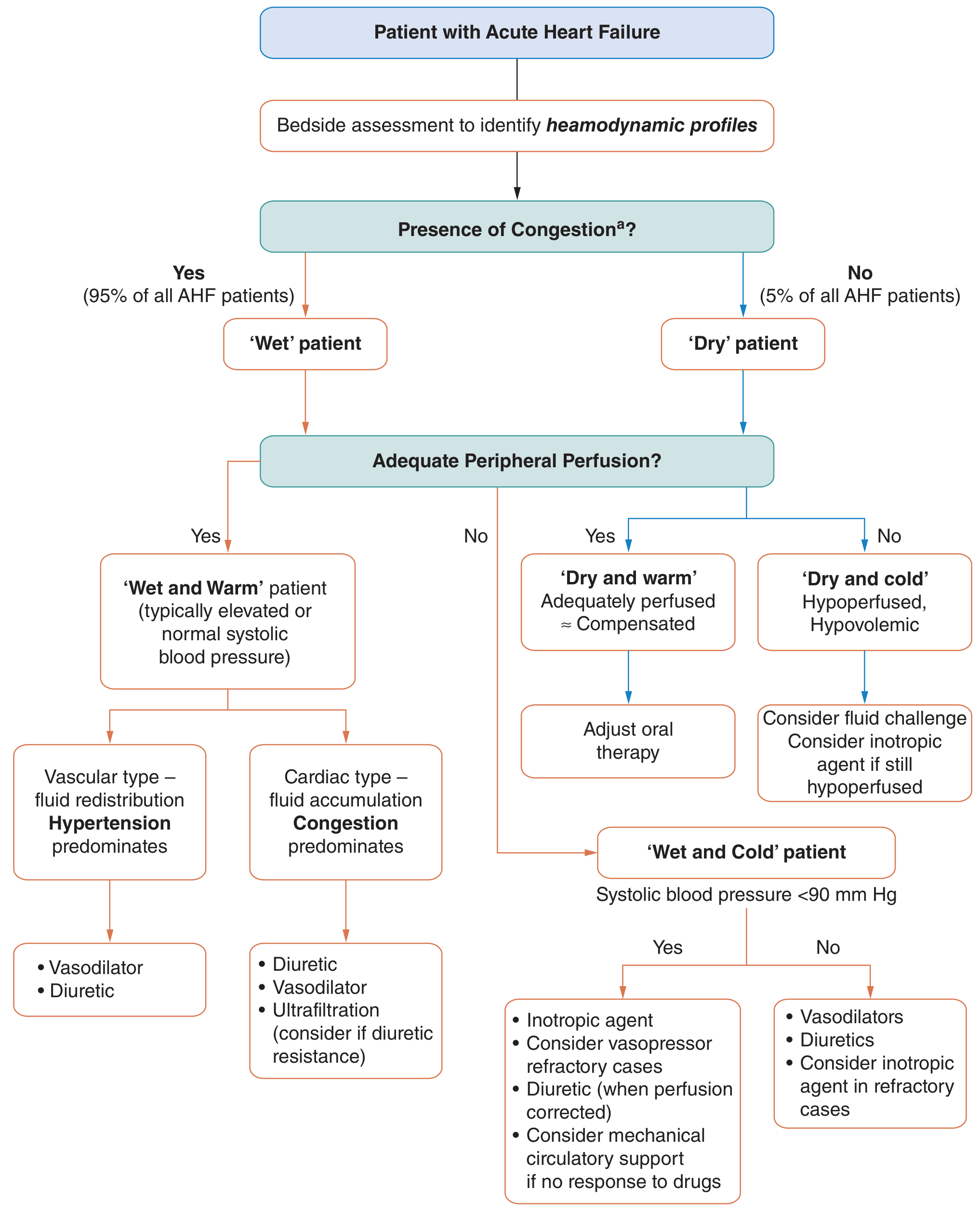
Figure: ESC-based algorithm for managing AHF based on clinical hemodynamic profile (from Fuster and Hurst's The Heart, 15th Ed.)
| Profile | Congestion | Perfusion | BP | Initial Approach |
|---|---|---|---|---|
| Wet + Warm | Yes | Adequate | Normal/elevated | Diuretics ± vasodilators |
| Wet + Cold | Yes | Poor | Low (<90 mmHg) | Inotropes; vasopressors if refractory; MCS if drug-refractory |
| Dry + Warm | No | Adequate | - | Adjust oral therapy (compensated) |
| Dry + Cold | No | Poor | Low | Fluid challenge; inotrope if still hypoperfused |
95% of AHF patients are "wet." - Fuster and Hurst's The Heart, 15th Edition
2. Immediate General Measures
- Sit the patient upright - reduces preload and work of breathing
- Oxygen: Target SpO2 ≥95%. Avoid hyperoxia in patients with chronic HF (may reduce cardiac output). Use high-flow oxygen or NIV for hypoxaemia
- Non-invasive ventilation (CPAP/BiPAP): Indicated for acute cardiogenic pulmonary edema with respiratory distress. Reduces preload, improves oxygenation, and avoids intubation. A Cochrane review (Vital et al.) confirmed benefit of CPAP/BiPAP in cardiogenic pulmonary edema - Braunwald's Heart Disease
- A 2024 meta-analysis (PMID 39166964) found high-flow nasal cannula (HFNC) non-inferior to NIV in AHF-related respiratory failure in some patient subgroups
- IV access + monitoring: Continuous ECG, pulse oximetry, hourly urine output. Insert urinary catheter
- Identify and treat precipitants: ACS/STEMI → urgent reperfusion; arrhythmias → rate/rhythm control; hypertensive emergency → rapid BP reduction; sepsis → antibiotics; medication non-adherence → dietary counseling
3. Pharmacological Management
A. Diuretics (Cornerstone of therapy)
- IV loop diuretics (furosemide, torsemide, bumetanide) are the primary treatment to restore euvolemia
- Initiate without delay - early intervention improves outcomes
- Dosing: IV furosemide starting dose = at least the patient's home oral dose (bioavailability doubles IV vs oral). For diuretic-naive patients: furosemide 40-80 mg IV bolus
- The DOSE trial compared low-dose (equivalent to home dose) vs high-dose (2.5× home dose) furosemide as bolus vs continuous infusion. High-dose showed a trend toward greater symptom improvement, more diuresis, and lower BNP, without worsening renal function - Fuster and Hurst's The Heart, 15th Ed.
- Diuretic resistance: Add metolazone or chlorothiazide (thiazide sequentially 30 min before loop diuretic), or switch to IV torasemide. Recent evidence: adding acetazolamide to high-dose furosemide has an important additive benefit - Katzung's Basic and Clinical Pharmacology, 16th Ed.
- SGLT2 inhibitors (dapagliflozin, empagliflozin): Emerging role in acute HF. A 2024 meta-analysis (PMID 39731023) found dapagliflozin safe and effective in acute HF management with favorable decongestion effects
- Monitor electrolytes (K⁺, Mg²⁺) and renal function closely. Mild rises in creatinine should not prompt diuretic dose reduction if the patient remains volume-overloaded
B. Vasodilators
Used in patients with volume overload without systemic hypotension (SBP >90 mmHg):
| Drug | Mechanism | Best Indication | Key Caution |
|---|---|---|---|
| IV Nitroglycerin | Primarily venodilator (high dose: arterial) | Hypertension, coronary ischemia, severe MR | Tachyphylaxis even at high doses; headache |
| Sodium Nitroprusside | Balanced arterial + venous dilator | Hypertensive emergency with severe MR/AR | Hypotension; thiocyanate toxicity (renal failure) |
| Nesiritide (BNP analogue) | Natriuretic; reduces LV filling pressures | Adjunct to diuresis | Hypotension; ASCEND-HF trial: no mortality benefit |
A 2025 meta-analysis (PMID 40506079) found high-dose nitroglycerin more effective than low-dose for sympathetic crashing acute pulmonary edema (SCPO), with an acceptable safety profile.
Vasodilators should be avoided in: aortic stenosis, severe diastolic dysfunction, or preload-dependent states. There are no data that vasodilators improve mortality in AHF. - Fuster and Hurst's The Heart, 15th Ed.
C. Morphine
- Historically used for anxiolysis, venodilation, and reducing sympathetic drive
- Current position: Use is now more cautious. Observational data (ADHERE registry) associated morphine with worse outcomes (higher intubation and ICU admission rates). Most guidelines reserve morphine for refractory dyspnea/distress only
D. Inotropes and Vasopressors
Reserved for the "wet and cold" or "dry and cold" patient with low cardiac output and end-organ hypoperfusion:
| Drug | Mechanism | Use |
|---|---|---|
| Dobutamine | β₁ agonist → ↑ inotropy, ↑ HR | Low CO with hypotension; bridge to MCS or transplant |
| Dopamine | Dose-dependent: low (renal D₁), mid (β₁), high (α₁) | Low CO with severe hypotension |
| Milrinone | PDE3 inhibitor → ↑ inotropy + vasodilation | Low CO; especially useful in beta-blocked patients |
| Levosimendan | Ca²⁺ sensitiser; PDE3 inhibitor | Low CO; approved in Europe; non-inferior to dobutamine |
| Norepinephrine | α₁ > β₁ vasopressor | Cardiogenic shock with refractory hypotension |
Risk: All inotropes increase arrhythmia risk and myocardial oxygen demand. Use at the lowest effective dose and taper as soon as hemodynamics improve. - Katzung's Basic & Clinical Pharmacology, 16th Ed.
E. Specific drug notes
- Digitalis (digoxin): Modest positive inotropic effect; primarily used for rate control in AF. Not a first-line inotrope in AHF
- Vasopressin antagonists (tolvaptan, conivaptan): For dilutional hyponatremia in AHF. Improve serum sodium but do not reduce mortality
4. Respiratory Support
| Modality | Indication |
|---|---|
| Supplemental O₂ (nasal prongs/mask) | Mild hypoxia (SpO2 <95%) |
| CPAP/BiPAP (NIV) | Moderate-severe pulmonary edema with respiratory distress |
| Intubation + mechanical ventilation | Failure of NIV, GCS ↓, respiratory arrest, refractory hypoxemia |
NIV reduces need for intubation and improves hospital mortality in cardiogenic pulmonary edema. - Morgan and Mikhail's Clinical Anesthesiology, 7th Ed.
5. Mechanical Circulatory Support (MCS)
For "wet and cold" patients refractory to pharmacological therapy:
- Intra-aortic balloon pump (IABP): Increases diastolic coronary perfusion, reduces afterload. First-line MCS in AHF from acute coronary ischemia
- Impella (axial flow pump): Greater hemodynamic support than IABP; increasingly used in cardiogenic shock
- VA-ECMO (venoarterial extracorporeal membrane oxygenation): Maximum support for refractory cardiogenic shock; bridge to recovery, VAD, or transplant
- Ultrafiltration: For diuretic-resistant volume overload; removes isotonic fluid directly
6. Phases of Management (ACC Framework)
| Phase | Goals |
|---|---|
| Phase I - Emergency/Stabilization | Treat life-threatening conditions (STEMI → reperfusion), relieve symptoms, identify precipitants, hemodynamic optimization |
| Phase II - In-hospital | Evidence-based decongestion, incorporate guideline-directed medical therapy (GDMT), prevent progression |
| Discharge planning | Initiate/optimize ACE-I/ARB/ARNI, beta-blockers, MRAs; patient education; arrange early follow-up (within 7-14 days) |
Three in-hospital trajectories (ACC consensus): improving toward target / stalled after initial response / not improved or worsening - each requiring different management escalation. - Fuster and Hurst's The Heart, 15th Ed.
7. Guideline-Directed Medical Therapy (GDMT) - Before Discharge
The hospitalization is an opportunity to initiate or optimize long-term therapy in HFrEF:
- ACE inhibitor / ARB or ARNI (sacubitril-valsartan) - reduce mortality and rehospitalization (PARADIGM-HF)
- Beta-blockers (carvedilol, metoprolol succinate, bisoprolol) - start low-dose after stabilization, NOT during acute decompensation
- Mineralocorticoid receptor antagonists (spironolactone, eplerenone) - augment diuresis and reduce mortality in HFrEF
- SGLT2 inhibitors (dapagliflozin, empagliflozin) - reduce cardiovascular death and HF hospitalization in HFrEF; can be initiated during hospitalization
8. Monitoring Parameters
- Vital signs, SpO₂, ECG continuously
- Urine output: target >0.5 mL/kg/hour
- Daily weight and fluid balance
- Electrolytes, BUN, creatinine: q12-24h during active diuresis
- BNP/NT-proBNP: baseline and before discharge (rising values = inadequate decongestion)
- Invasive hemodynamic monitoring (pulmonary artery catheter) for complex cases: cardiogenic shock, unclear fluid status, or refractory disease
Key References
- Fuster and Hurst's The Heart, 15th Edition - Ch. 50: Evaluation and Management of Acute Heart Failure
- Braunwald's Heart Disease, 12th Edition - Management of the Patient with Acute Heart Failure
- Katzung's Basic and Clinical Pharmacology, 16th Edition - Management of Acute Heart Failure
- Morgan and Mikhail's Clinical Anesthesiology, 7th Edition - Treatment of Cardiogenic Pulmonary Edema
- DOSE trial (furosemide strategies) | ASCEND-HF (nesiritide) | PARADIGM-HF (sacubitril-valsartan)
- Recent evidence: dapagliflozin in AHF (PMID 39731023) | high-dose nitroglycerin for SCPO (PMID 40506079) | HFNC vs NIV (PMID 39166964)
This is a shared conversation. Sign in to Orris to start your own chat.