Hypokalemia evaluation & management
Reading File
Finding Sources
Searching PubMed
"hypokalemia"[MeSH Terms] AND management
Searching the Web
hypokalemia evaluation management guidelines 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
hypokalemia diagnostic algorithm evaluation flowchart
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
I now have comprehensive, authoritative content from multiple major textbooks. Let me compile the full response.
Hypokalemia: Evaluation & Management
Definition & Epidemiology
Hypokalemia is defined as serum potassium < 3.5 mEq/L. It is the most common electrolyte abnormality in clinical practice — affecting >20% of hospitalized patients and up to 40% of outpatients on thiazide diuretics. Severity is classified as:
| Severity | K⁺ (mEq/L) |
|---|---|
| Mild | 3.0–3.5 |
| Moderate | 2.5–3.0 |
| Severe | < 2.5 |
(Rosen's Emergency Medicine)
Pathophysiology
Hypokalemia arises from three mechanisms:
- Transcellular shift (intracellular redistribution) — acute, without total body K⁺ deficit
- Decreased intake — rarely sufficient alone
- Increased losses — renal or extrarenal (most common cause of sustained hypokalemia)
Each 0.3 mEq/L drop in serum K⁺ below normal corresponds to approximately 100 mEq of total body deficit. However, this correlation is imprecise because serum K⁺ reflects both external balance and transcellular shifts simultaneously.
Causes
Five Major Categories (Rosen's EM)
| Category | Examples |
|---|---|
| Renal losses | Diuretics (thiazide > loop), steroids, hyperaldosteronism, RTA, DKA, alcohol, penicillins, aminoglycosides, amphotericin B, cisplatin |
| Non-renal losses | Diarrhea, vomiting/NG suction (indirect — via alkalosis/hyperaldo), sweating, burns |
| Decreased intake | Malnutrition, alcoholism |
| Transcellular shift | Insulin, β₂-agonists, metabolic alkalosis, hyperventilation, thyrotoxic periodic paralysis, familial hypokalemic periodic paralysis (FHPP), barium, theophylline, chloroquine |
| Endocrine | Primary hyperaldosteronism (Conn syndrome), Cushing's, ectopic ACTH syndrome, Liddle syndrome |
Note on vomiting: Gastric fluid contains only 5–10 mEq/L of K⁺. Hypokalemia with vomiting is primarily from metabolic alkalosis, chloride loss, and secondary hyperaldosteronism — not direct gastric K⁺ loss.
Pseudohypokalemia: Transcellular shift in vitro occurs with leukocytosis >100,000/μL or prolonged room-temperature storage. Confirm by rapid separation at 4°C.
Clinical Features
Symptoms generally appear when K⁺ < 3.0 mEq/L (or with abrupt falls at higher levels).
Neuromuscular
- Generalized weakness, fatigue, myalgia
- Depressed deep tendon reflexes, fasciculations
- Paralysis (including respiratory muscles) at K⁺ < 2.0 mEq/L → life-threatening
Cardiac
- In patients without heart disease, arrhythmias are rare above 3.0 mEq/L
- With ischemia or heart failure, even mild hypokalemia increases arrhythmia risk
- Independent risk factor for arrhythmic death; target K⁺ > 4.5 mEq/L in acute MI
- Target K⁺ 4.0–5.0 mEq/L in heart failure
ECG Changes
Progressive findings: ST depression → T-wave flattening → prominent U wave → T-U fusion → QT prolongation → torsades de pointes (when QTc > 500 ms, risk ↑ 2–3×)
Renal
- Hypokalemic nephropathy, polyuria/polydipsia (NDI-like)
Other
- Glucose intolerance (impairs insulin secretion)
- Rhabdomyolysis (severe cases)
- Ileus (paralytic)
Diagnostic Evaluation
Harrison's Diagnostic Algorithm
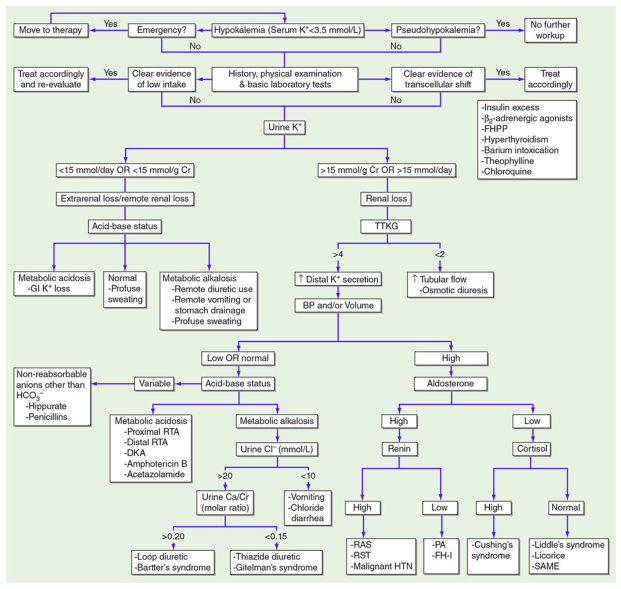
Step-by-step approach:
1. Emergency? → If yes, move directly to therapy while investigating.
2. Pseudohypokalemia? → Rule out in-vitro shift (leukocytosis, prolonged storage).
3. History, exam, basic labs — check for:
- Clear evidence of low intake (malnutrition, alcoholism) → treat accordingly
- Clear evidence of transcellular shift (insulin, alkalosis, β₂-agonist, FHPP, thyrotoxicosis) → treat cause
4. Urine K⁺ (spot or 24-hour):
| Result | Interpretation |
|---|---|
| < 15 mmol/day or < 15 mmol/g Cr | Extrarenal/remote renal loss |
| > 15 mmol/day or > 15 mmol/g Cr | Ongoing renal K⁺ wasting |
(A spot urine K⁺ > 13 mEq/g Cr indicates inappropriate renal losses)
5. If renal loss → TTKG (transtubular potassium gradient = [urine K⁺ / plasma K⁺] ÷ [urine Osm / plasma Osm]):
- TTKG > 4: ↑ distal K⁺ secretion → check BP/volume → check aldosterone → if high + high renin: RAS/RST/malignant HTN; if high + low renin: primary aldosteronism (PA), FH-I; if low: check cortisol → high = Cushing's; normal = Liddle/licorice/SAME
- TTKG < 2: ↑ tubular flow / osmotic diuresis
6. If extrarenal loss → acid-base status:
- Metabolic acidosis: GI K⁺ loss (diarrhea)
- Normal: profuse sweating
- Metabolic alkalosis: remote diuretic use, vomiting/NG drainage → check urine Cl⁻:
- Urine Cl⁻ > 20 mmol/L + urine Ca/Cr > 0.20 → Loop diuretic / Bartter syndrome
- Urine Cl⁻ > 20 mmol/L + urine Ca/Cr < 0.15 → Thiazide / Gitelman syndrome
- Urine Cl⁻ < 10 mmol/L → vomiting, chloride diarrhea
Management
General Principles
- Identify and treat the underlying cause
- Replete K⁺ with appropriate route and rate
- Correct hypomagnesemia — critical (see below)
- Monitor frequently — K⁺ levels every 2–3 hours during IV repletion
Oral Potassium Replacement
- Preferred for mild-to-moderate hypokalemia (K⁺ 2.5–3.5 mEq/L) in patients who can take PO
- Safer than IV — less overshoot risk
- KCl is most commonly used (available as liquid, powder, tablet)
- Dose: 20–40 mEq per dose, up to 40–60 mEq q2–4h
- Dietary sources: potatoes, avocado, black beans, bananas, fresh fruits, nuts, legumes
IV Potassium Replacement
| Indication | Rate |
|---|---|
| Mild/moderate (K⁺ 2.5–3.5), unable to take PO | 20–40 mEq KCl in 1 L NS over ≥ 8 hours |
| Severe symptomatic (K⁺ < 3.0 mEq/L) | 10–20 mEq/hr |
| Life-threatening (K⁺ < 2.0 mEq/L or QTc > 500 ms) | Up to > 20 mEq/hr — requires continuous cardiac monitoring + central line |
Do not give IV KCl faster than 10 mmol/hr without continuous ECG monitoring.
Large deficits may require several days of combined oral + IV replacement.
The Magnesium Connection ⚠️
- ~50% of hypokalemic patients have concurrent hypomagnesemia
- Mg²⁺ is a critical cofactor for Na⁺/K⁺-ATPase and maintenance of intracellular K⁺
- Hypomagnesemia causes refractory hypokalemia — K⁺ replacement will fail without Mg²⁺ repletion
- Rule: unless the patient receives ≥ 0.5 g/hr MgSO₄ concurrently, potassium will not move intracellularly and will be lost in urine
- Always check and replace Mg²⁺ when treating hypokalemia
(Rosen's EM, Sabiston Surgery, Harrison's, NKF Primer)
K⁺-Sparing Strategies (Chronic/Recurrent Hypokalemia)
For patients on diuretics or with persistent renal K⁺ wasting:
- Add potassium-sparing diuretic (spironolactone, eplerenone, amiloride, triamterene)
- Switch to combined thiazide + K⁺-sparing agent
- ACE inhibitor or ARB (reduce aldosterone-mediated K⁺ secretion)
- Chronic oral K⁺ supplementation
- Dietary modification (potassium-rich foods)
(Brenner & Rector's The Kidney)
Special Populations
| Population | Target K⁺ | Notes |
|---|---|---|
| Acute MI | > 4.5 mEq/L | ↑ arrhythmic risk; aggressive repletion |
| Heart failure | 4.0–5.0 mEq/L | Independent mortality risk factor |
| Digoxin use | > 4.0 mEq/L | Hypokalemia potentiates digoxin toxicity |
| DKA | Replete early | Despite initial normal/high K⁺, total body deficit is 2–3 mEq/kg |
| Thyrotoxic periodic paralysis | Beta-blocker + K⁺ repletion | Avoid excessive K⁺ (risk rebound hyperkalemia post-correction) |
| Transcellular shift (no true deficit) | Minimal replacement | Risk rebound hyperkalemia once shift reverses |
Disposition
- Mild (K⁺ > 3.0, asymptomatic, no ECG changes): Discharge with oral replacement, dietary advice, repeat labs in 1 week
- Moderate (K⁺ 2.5–3.0): Oral/IV replacement; admit if symptomatic or cardiac comorbidities
- Severe (K⁺ < 2.5) or symptomatic: Admit; continuous ECG monitoring; IV replacement; investigate underlying cause
Key Pearls
- Serum K⁺ is a poor proxy for total body deficit — replace incrementally with frequent monitoring
- Always replace Mg²⁺ — refractory hypokalemia is almost always due to unrecognized hypomagnesemia
- Vomiting causes hypokalemia indirectly (alkalosis + hyperaldosteronism), not from gastric K⁺ loss
- TTKG and urine Cl⁻ are the key discriminating tests for renal vs. extrarenal etiology
- Transcellular shift hypokalemia (e.g., insulin, β₂-agonist, FHPP) requires little K⁺ replacement — risk of rebound hyperkalemia
- Ectopic ACTH syndrome (small cell lung, bronchial carcinoid) classically presents with severe, refractory hypokalemia + HTN
Sources: Rosen's Emergency Medicine, 10th Ed.; Harrison's Principles of Internal Medicine, 21st/22nd Ed.; Brenner & Rector's The Kidney, 2-Vol Set; NKF Primer on Kidney Diseases, 8th Ed.; Sabiston Textbook of Surgery, 21st Ed.
This is a shared conversation. Sign in to Orris to start your own chat.