Status asthamaticus harrison based
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive Harrison's content. Let me compile the full answer:
Status Asthmaticus - Harrison's Principles of Internal Medicine (22nd Ed., 2025)
Definition
Status asthmaticus is a severe, prolonged asthma attack that does not respond adequately to standard initial bronchodilator therapy. According to Goldman-Cecil (which mirrors Harrison's criteria):
- PEFR or FEV1 does not increase to >40% of predicted with treatment
- Rising PaCO2 without improvement in airflow obstruction indices
- Development of a major complication: pneumothorax, pneumomediastinum, acute myocardial ischemia, or cardiac tachyarrhythmia (other than sinus tachycardia)
Pathophysiology Key Point
Most asthma attack patients present with hypocapnia (low PCO2) due to high respiratory rate.
Critical warning sign: A normal or near-normal PCO2 in a patient in respiratory distress signals impending respiratory failure and the need for mechanical ventilation.
Management: Step-by-Step (Harrison's Approach)
Step 1 - Outpatient/Mild-Moderate Deterioration
- Beta2-agonist (e.g., albuterol) up to every 1 hour
- Consider increasing ICS dose 4-5x
- If hourly beta2-agonist needed for several hours → refer for urgent care
Step 2 - Urgent Care Setting
- Assess PEFR or FEV1
- Nebulized beta2-agonists up to every 20 minutes
- Supplemental oxygen to correct hypoxemia
- Add nebulized anticholinergics (ipratropium) for additional bronchodilation
- If PEFR >60% predicted: beta2-agonists alone often work; if fail to respond in 1-2 h → IV corticosteroids
- Sometimes add: LTRA, magnesium sulfate
Step 3 - Failure to Respond / Status Asthmaticus
Failure to achieve PEFR >60% or persistent severe tachypnea over 4-6 hours → admit to hospital
In-Hospital Treatment:
| Intervention | Details |
|---|---|
| Continuous bronchodilator nebulization | Albuterol 0.083% solution, up to every 2 h |
| IV corticosteroids | Methylprednisolone 40-60 mg IV every 4-6 h (high-dose) |
| IV aminophylline | Loading dose 500-1000 mg over 1 h, then infusion 30-60 mg/h; target plasma level 15-20 mcg/mL |
| Oxygen | Via face mask/nasal cannula; target SpO2 adequate saturation |
| Magnesium sulfate | IV adjunct to standard therapy |
| NIPPV (BiPAP/CPAP) | Non-invasive positive-pressure ventilation for respiratory exhaustion; helps prevent intubation |
| Heliox | Helium-oxygen mixture to decrease work of breathing |
| Antibiotics | Only if signs of infection |
Mechanical Ventilation in Status Asthmaticus
Intubation is challenging due to high positive pressures from airflow obstruction. Key principles:
- Low respiratory rates and/or low tidal volumes to decrease peak airway pressures
- Permissive hypercapnia: allow PCO2 to rise intentionally
- If critical acidosis: correct temporarily with IV sodium bicarbonate to raise pH
- Neuromuscular paralysis may sometimes be beneficial
- Bronchoscopy to clear mucus plugs has been described but is dangerous in this setting - use with extreme caution
High-Risk Patients for Asthma Mortality (Table 298-6)
Harrison's lists the following as high-risk features to consider in any patient presenting with asthma:
- History of ICU admission for asthma
- History of intubation for asthma
- Illicit drug use
- Depression
- New diagnosis within past year
- ≥2 emergency visits in past 6 months
- Severe psychosocial problems
- Lower socioeconomic status
- On daily prednisone prior to admission
Summary Algorithm
Mild-Moderate Attack
└─> Beta2-agonist q1h + ↑ICS 4-5x
└─> Hourly beta2-agonist for hours → Urgent care
└─> PEFR/FEV1 assessment
├─> PEFR >60%: Nebulized beta2-agonist q20 min
│ └─> No response in 1-2h → IV steroids
└─> PEFR <60% or no response in 4-6h → ADMIT
└─> Continuous bronchodilators + IV steroids
+ IV aminophylline + O2 + Mg2+
└─> PCO2 rising → Prepare for MV
└─> Permissive hypercapnia
+ Low rate/volume strategy
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 298 - Asthma, pp. 2269-2270 (ASTHMA ATTACKS / HIGH-RISK ASTHMA PATIENTS sections)
- Goldman-Cecil Medicine, Chapter 75 - Status Asthmaticus section, p. 888
Gbs
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive Harrison's-based GBS answer. Here it is:
Guillain-Barré Syndrome (GBS) - Harrison's Principles of Internal Medicine, 22nd Ed.
Definition & Epidemiology
GBS is an acute, frequently severe, and fulminant polyradiculoneuropathy that is autoimmune in nature.
- Incidence: 10-20 cases per million per year; ~5,000-6,000 cases/year in the USA
- Males slightly more affected than females
- Adults more frequently affected than children (in Western countries)
- Occurs year-round
Antecedent Events / Triggers
~70% of cases occur 1-3 weeks after an acute infectious process (respiratory or GI):
| Trigger | Proportion |
|---|---|
| Campylobacter jejuni | 20-30% (most common) |
| Human herpes virus (CMV, EBV) | ~Similar proportion |
| Other: HIV, Hepatitis E, Zika virus, Mycoplasma pneumoniae | Less common |
| SARS-CoV-2 | Reported, causal link not established |
| Vaccines (adenovector COVID-19 vaccines) | Slightly increased risk |
| Swine flu vaccine (1976) | Most notable vaccine example |
Note: mRNA COVID vaccines do NOT carry increased GBS risk.
Clinical Manifestations
- Rapidly evolving areflexic motor paralysis with or without sensory disturbance
- Ascending paralysis - often described as "rubbery legs" first
- Weakness evolves over hours to a few days
- Tingling dysesthesias in extremities
- Legs > arms; facial paresis in 50%
- Lower cranial nerve involvement - bulbar weakness (difficulty handling secretions, maintaining airway)
- Pain (neck, shoulder, back, spine) in ~50% in early stages
- Deep tendon reflexes - attenuate or disappear within first few days
- Large-fiber sensory functions (proprioception, DTRs) more severely affected than cutaneous sensation
- Bladder dysfunction - may occur in severe cases, usually transient
- Fever and constitutional symptoms absent at onset (if present, doubt the diagnosis)
- Weakness reaches nadir in 2-4 weeks, then plateau
Warning: ~30% of patients require ventilatory assistance, especially those with:
- Severe weakness on admission
- Rapid progression
- Facial and/or bulbar weakness in the first week
Subtypes and Associated Autoantibodies (Harrison's Fig. 458-1)
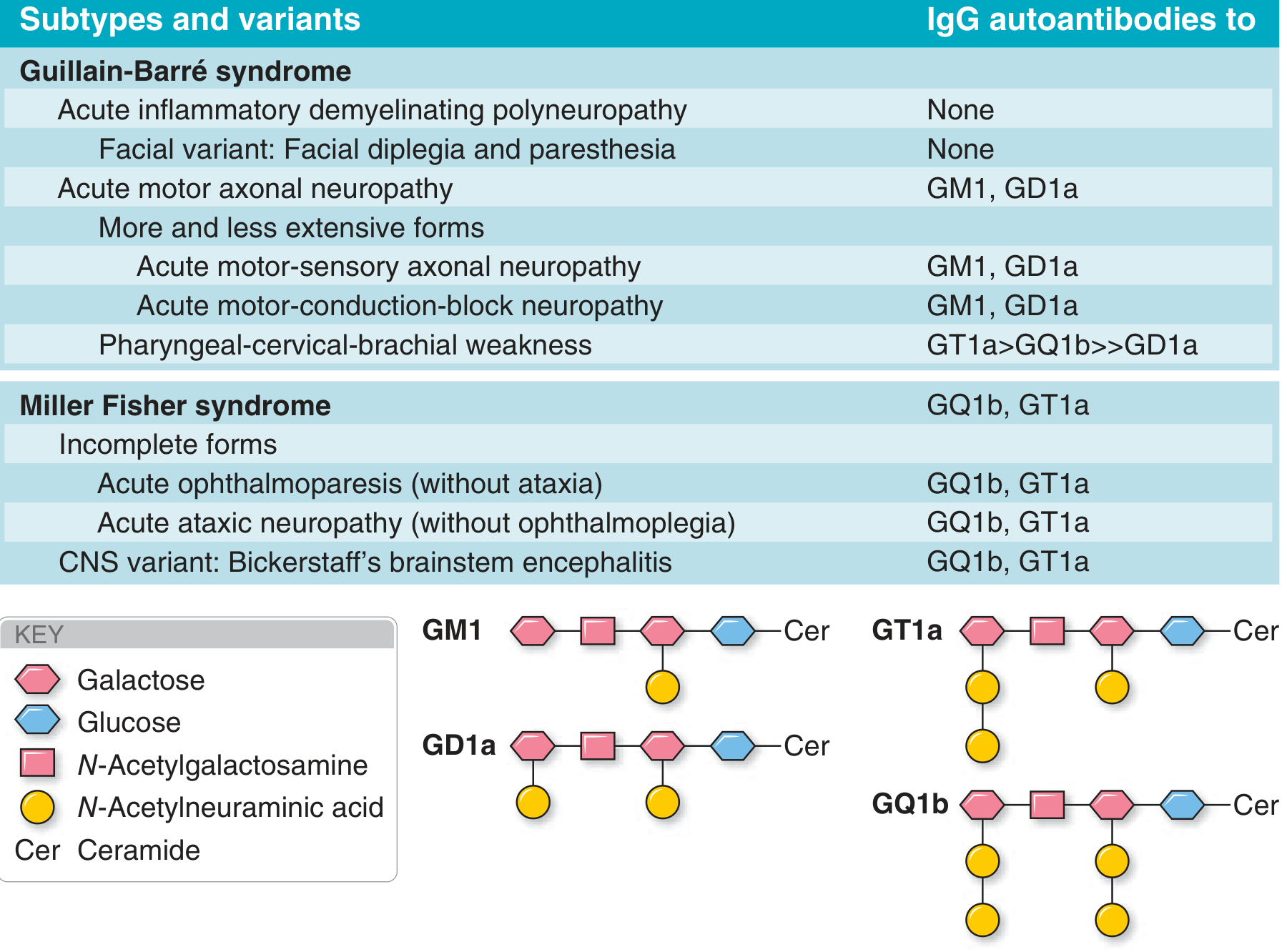
| Subtype | Autoantibody |
|---|---|
| AIDP (Acute Inflammatory Demyelinating Polyneuropathy) | None identified (most common in West) |
| AMAN (Acute Motor Axonal Neuropathy) | Anti-GM1, GD1a, GM1b, GalNAc-GD1a |
| AMSAN (Acute Motor-Sensory Axonal Neuropathy) | Anti-GM1, GD1a |
| Miller Fisher Syndrome (MFS) | Anti-GQ1b (>90%) - classic triad: ophthalmoplegia + ataxia + areflexia |
| Pharyngeal-cervical-brachial weakness | Anti-GT1a |
Pathophysiology
- Molecular mimicry: Immune response to antecedent infection cross-reacts with peripheral nerve components
- In AIDP: T cell-mediated + antibody/complement-mediated attack on Schwann cell surface and myelin
- In AMAN: Antibodies (anti-GM1, anti-GD1a) attack axolemma at nodes of Ranvier - no demyelination
- Anti-GQ1b antibodies: Found in >90% of MFS; GQ1b is highly expressed in extraocular motor nerves - explains selective ophthalmoplegia
- Earliest pathologic finding: activated macrophages penetrate the basement membrane of Schwann cells
Investigations
CSF (Lumbar Puncture) - Classic Finding
- Cytoalbuminous dissociation (albuminocytologic dissociation):
- Elevated protein (often >45 mg/dL, may reach 100-1000 mg/dL)
- Normal or near-normal white cell count (<10 cells/μL)
- CSF may be normal in the first week
Electrodiagnostic Studies (NCS/EMG)
- AIDP: Reduced conduction velocity, prolonged distal latencies, conduction block, absent F-waves (demyelinating pattern)
- AMAN/AMSAN: Reduced CMAP amplitudes, preserved conduction velocity (axonal pattern)
- Sural nerve "spared" pattern (sural sparing with absent median sensory)
Serology
- Anti-GQ1b (MFS), Anti-GM1/GD1a (AMAN), NCS, CBC, electrolytes, renal/liver function, LFTs
- HIV testing if risk factors
Diagnostic Criteria (Brighton/WHO Criteria per Harrison's)
Level 1 (Highest certainty) - GBS:
- Bilateral flaccid limb weakness
- Decreased/absent DTRs in weak limbs
- Monophasic illness; onset to nadir: 12 hours to 28 days; then clinical plateau
- Albuminocytologic dissociation: CSF WBC <50 cells/μL + elevated CSF protein
- Electrodiagnostic evidence consistent with GBS
- No alternative diagnosis
Level 2:
- Same motor findings + monophasic pattern + CSF WBC <50 (with or without protein elevation) OR EDx consistent
- No alternative diagnosis
Level 3 (Lowest certainty):
- Bilateral flaccid limb weakness + decreased DTRs + monophasic pattern
- No alternative diagnosis (no CSF/EDx required)
Miller Fisher Syndrome Diagnosis (Level 1):
- Bilateral ophthalmoparesis + bilateral reduced/absent DTRs + ataxia
- Absence of limb weakness
- Monophasic; onset to nadir: 12 h to 28 days
- Albuminocytologic dissociation + normal/sensory-only NCS
- No corticospinal signs, no altered consciousness
- No alternative diagnosis
Treatment
Specific Immunotherapy - Two equivalent options:
| Treatment | Regimen | Benefit |
|---|---|---|
| IVIg (Intravenous Immunoglobulin) | 0.4 g/kg/day x 5 days (total 2 g/kg) | Reduces MV need; speeds recovery |
| PLEX (Plasma Exchange) | ~40-50 mL/kg, 4-6 exchanges over 7-12 days | Reduces MV need from 27% to 14%; full recovery at 1 year improves from 55% to 68% |
Key points:
- IVIg and PLEX are equally effective - neither is superior
- Combination is NOT more effective than either alone
- Corticosteroids are NOT beneficial (not recommended)
- Lack of noticeable improvement after one treatment is NOT an indication to try the other (except if patient worsened then stabilized)
- Treatment most effective if started within 2 weeks of onset
Supportive Care (Critical - ICU Monitoring Required):
- Vital capacity monitoring - serial measurements (intubate if VC <15-20 mL/kg or <1 L)
- Cardiac monitoring (arrhythmias from autonomic instability)
- Blood pressure monitoring (autonomic dysfunction - labile BP)
- DVT prophylaxis (heparin + compression stockings)
- Nutrition support
- Chest physiotherapy
- Tracheotomy: consider after 2 weeks of intubation
- Daily range-of-motion exercises (prevent joint contractures)
- Pain management (gabapentin, carbamazepine, opioids for neuropathic pain)
- Psychological support and reassurance
Prognosis
- ~85% achieve full functional recovery within several months to 1 year
- Mortality <5% in optimal care settings (usually from pulmonary complications)
- 5-10% have one or more late relapses - may be reclassified as CIDP
Poor Prognostic Factors:
- Severe proximal motor and sensory axonal damage
- Advanced age
- Fulminant or severe attack
- Delay in onset of treatment
- Elevated serum neurofilament light (NfL) chains
- High titers of anti-GM1 antibodies (more axonal involvement)
Autonomic Dysfunction
A significant and potentially life-threatening feature:
- Sinus tachycardia (most common)
- Bradycardia, heart block
- Labile blood pressure
- Urinary retention
- Paralytic ileus
- Orthostatic hypotension
Source: Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 458 - Guillain-Barré Syndrome and Other Immune-Mediated Neuropathies
This is a shared conversation. Sign in to Orris to start your own chat.