Acid base biochemistry 1st year MBBS full notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Let me compile the comprehensive notes:
Acid-Base Biochemistry - 1st Year MBBS Full Notes
Sources: Lippincott Illustrated Reviews Biochemistry 8th Ed | Basic Medical Biochemistry 6th Ed | Guyton & Hall Medical Physiology
1. OVERVIEW
Acid-base biochemistry covers the properties of proton donors and acceptors in biological systems, the concept of pH, buffer systems, and disturbances that occur in clinical disease. This is foundational for understanding protein function, enzyme activity, and normal physiology.
2. DEFINITIONS
| Term | Definition |
|---|---|
| Acid | A proton (H+) donor |
| Base | A proton (H+) acceptor |
| Conjugate base | The ionized form (A-) of a weak acid (HA) after donating a proton |
| Weak acid | An acid that ionizes only partially in solution (e.g., carbonic acid H2CO3) |
| Strong acid | An acid that fully dissociates in water (e.g., HCl) |
| Buffer | A solution that resists change in pH upon addition of acid or base |
3. pH - DEFINITION AND SCALE
The concentration of protons [H+] in aqueous solution is expressed as pH:
$$\text{pH} = \log \frac{1}{[H^+]} = -\log[H^+]$$
Key values:
- Neutral water: pH 7.0 (at 25°C, [H+] = [OH-] = 10-7 mol/L)
- Normal arterial blood pH: 7.35 - 7.45
- Normal intracellular pH: ~7.0 (slightly acidic compared to blood)
- Acidosis: blood pH < 7.35
- Alkalosis: blood pH > 7.45
The pH scale is logarithmic - a change of 1 pH unit represents a 10-fold change in [H+]. A drop from pH 7.4 to 6.4 means [H+] increased 10-fold.
4. DISSOCIATION CONSTANT (Ka and pKa)
For a weak acid HA dissociating: HA ⇌ H+ + A-
The dissociation constant Ka is:
$$K_a = \frac{[H^+][A^-]}{[HA]}$$
- Larger Ka = stronger acid (more dissociated)
- Smaller Ka = weaker acid (less dissociated)
Since Ka values are often very small, we use:
$$\text{pKa} = -\log K_a$$
- Lower pKa = stronger acid
- Higher pKa = weaker acid
5. HENDERSON-HASSELBALCH EQUATION
Derived from the Ka expression by taking -log of both sides:
$$\boxed{pH = pKa + \log \frac{[A^-]}{[HA]}}$$
Or for the bicarbonate buffer system:
$$pH = pKa + \log \frac{[HCO_3^-]}{[H_2CO_3]}$$
How to interpret it:
- When [A-] = [HA], log(1) = 0, so pH = pKa - this is the midpoint of the titration curve
- When [A-] > [HA], pH > pKa (solution is more basic)
- When [HA] > [A-], pH < pKa (solution is more acidic)
- Buffering is most effective when pH is within ±1 unit of pKa (i.e., the ratio [A-]/[HA] is between 0.1 and 10)
Clinical application:
The bicarbonate buffer is the most important extracellular buffer in blood:
- pKa of H2CO3/HCO3- = 6.1
- Normal [HCO3-] = 24 mEq/L; [H2CO3] = 1.2 mEq/L
- pH = 6.1 + log(24/1.2) = 6.1 + log(20) = 6.1 + 1.3 = 7.4
6. BUFFER SYSTEMS
A buffer is created by mixing a weak acid (HA) with its conjugate base (A-).
How a buffer works:
- If acid (H+) is added → A- neutralizes it: A- + H+ → HA
- If base (OH-) is added → HA neutralizes it: HA + OH- → A- + H2O
Key properties:
- Maximum buffering capacity occurs when pH = pKa (equal amounts of acid and conjugate base)
- Effective buffering range: pKa ± 1 pH unit
7. BIOLOGICALLY IMPORTANT BUFFERS
A. Bicarbonate Buffer System (Extracellular)
- Most important buffer in blood plasma
- H2CO3 ⇌ H+ + HCO3-
- pKa = 6.1
- Although pH 7.4 is far from pKa 6.1, this system is highly effective because:
- CO2 is continuously regulated by lungs (respiratory compensation)
- HCO3- is regulated by kidneys (renal compensation)
- It is an open system - CO2 can be blown off
B. Phosphate Buffer System (Intracellular)
- H2PO4- ⇌ H+ + HPO42-
- pKa = 6.8 (close to intracellular pH of ~7.0)
- Important inside cells and in urine
C. Protein Buffer System
- Histidine residues (pKa ~6.0) are particularly important
- Hemoglobin is a major blood buffer - can accept H+ when O2 is released
- Plasma proteins (albumin) also contribute
D. Hemoglobin Buffer
- Deoxyhemoglobin is a weaker acid than oxyhemoglobin
- At tissues: O2 released → deoxyhemoglobin forms → accepts H+ produced by CO2 metabolism
- Isohydric shift: CO2 + H2O → H2CO3 → H+ + HCO3- (H+ buffered by Hb, HCO3- enters plasma)
8. TITRATION CURVES
A titration curve plots pH (y-axis) vs. equivalents of base added (x-axis).
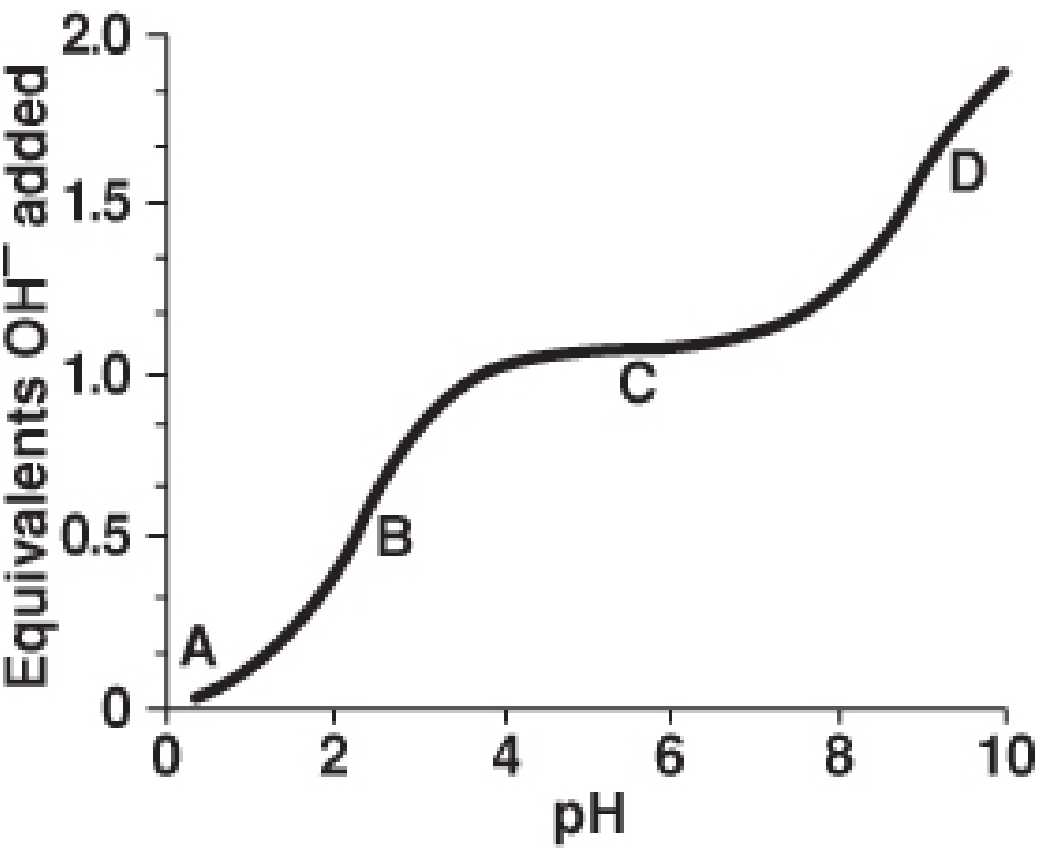
Titration curve of a nonpolar amino acid - Lippincott Illustrated Reviews Biochemistry 8e
Points on the curve:
| Point | Description |
|---|---|
| A | Amino acid fully protonated (lowest pH, start of titration) |
| B | pH = pKa1 (carboxyl group). Maximum buffering capacity for -COOH. [HA] = [A-] |
| C | Isoelectric point (pI) - midway between pKa1 and pKa2. Net charge = 0 |
| D | pH = pKa2 (amino group). Maximum buffering capacity for -NH3+ |
Shape characteristics:
- The flat, S-shaped region (inflection point) = maximum buffering
- The steep portion at pI = minimum buffering (most vulnerable to pH change)
9. AMINO ACID IONIZATION
Ionizable groups on amino acids:
| Group | pKa range |
|---|---|
| α-Carboxyl (-COOH) | 1.8 - 2.4 |
| α-Amino (-NH3+) | 8.8 - 11.0 |
| Side chain Asp/Glu (-COOH) | ~4.0 |
| Side chain His (-imidazole) | ~6.0 |
| Side chain Cys (-SH) | ~8.3 |
| Side chain Tyr (-OH) | ~10.0 |
| Side chain Lys (-NH3+) | ~10.5 |
| Side chain Arg (guanidinium) | ~12.5 |
Zwitterion:
At physiologic pH 7.4, an amino acid carries both positive (-NH3+) and negative (-COO-) charges simultaneously = zwitterion (electrically neutral overall for simple amino acids)
Isoelectric point (pI):
- The pH at which the molecule carries zero net charge
- For a simple amino acid: pI = (pKa1 + pKa2) / 2
- For acidic amino acids (Asp, Glu): pI = (pKa1 + pKa of side chain) / 2 → pI < 7
- For basic amino acids (Lys, Arg, His): pI = (pKa of side chain + pKa2) / 2 → pI > 7
10. BLOOD pH AND ACID-BASE DISTURBANCES
Normal blood values:
| Parameter | Normal Value |
|---|---|
| Arterial pH | 7.35 - 7.45 |
| pCO2 (arterial) | 35 - 45 mmHg |
| HCO3- | 22 - 26 mEq/L |
| pO2 (arterial) | 80 - 100 mmHg |
Four primary acid-base disturbances:
| Disorder | pH | Primary Change | Compensation |
|---|---|---|---|
| Metabolic Acidosis | ↓ | ↓ HCO3- | ↑ Ventilation → ↓ pCO2 (Kussmaul breathing) |
| Metabolic Alkalosis | ↑ | ↑ HCO3- | ↓ Ventilation → ↑ pCO2 |
| Respiratory Acidosis | ↓ | ↑ pCO2 | Kidneys retain HCO3-, excrete H+ |
| Respiratory Alkalosis | ↑ | ↓ pCO2 | Kidneys excrete HCO3-, retain H+ |
Causes (important exam points):
Metabolic Acidosis:
- Diabetic ketoacidosis (DKA) - accumulation of ketone bodies (acetoacetate, β-hydroxybutyrate)
- Lactic acidosis - anaerobic metabolism
- Renal failure - retention of H+, loss of HCO3-
- Diarrhea - loss of HCO3- in stool
Metabolic Alkalosis:
- Vomiting - loss of HCl
- Diuretics (furosemide, thiazides) - loss of Cl-, K+
- Hyperaldosteronism - increased H+ excretion by kidney
Respiratory Acidosis:
- Hypoventilation - COPD, respiratory center depression (opioids)
- CO2 retention
Respiratory Alkalosis:
- Hyperventilation - anxiety, early sepsis, ascent to high altitude
- Excess CO2 blown off
11. REGULATION OF BLOOD pH - THREE MECHANISMS
A. Chemical Buffer Systems (Seconds)
- Immediate, first line of defense
- Bicarbonate, phosphate, hemoglobin, proteins
- Do not eliminate H+ - they just redistribute it
B. Respiratory Regulation (Minutes)
- Medullary respiratory centers detect [H+] and CO2
- ↑ [H+] → ↑ ventilation rate → CO2 exhaled → pH rises
- CO2 + H2O ⇌ H2CO3 ⇌ H+ + HCO3- (carbonic anhydrase)
- Respiratory compensation is rapid but limited
C. Renal Regulation (Hours - Days)
- Most powerful, but slowest
- Kidneys excrete H+ directly into urine (bound to phosphate as titratable acid or as NH4+)
- Kidneys reabsorb HCO3- (mainly proximal tubule)
- Kidneys generate new HCO3- (distal tubule/collecting duct)
- Only mechanism that truly eliminates acid
12. CO2 TRANSPORT AND ACID-BASE
CO2 produced in tissues is transported to the lungs via three mechanisms:
| Form | % of Total |
|---|---|
| Dissolved in plasma | ~7% |
| As HCO3- (bicarbonate) | ~70% |
| Carbaminohemoglobin (CO2 bound to Hb-NH2) | ~23% |
The key reaction (red blood cells):
$$CO_2 + H_2O \xrightarrow{\text{carbonic anhydrase}} H_2CO_3 \rightarrow H^+ + HCO_3^-$$
- H+ is buffered by hemoglobin (Haldane effect / isohydric mechanism)
- HCO3- exits RBC via Cl-/HCO3- exchanger (chloride shift / Hamburger phenomenon)
13. CARBONIC ANHYDRASE
- Enzyme in RBCs, renal tubular cells, gastric mucosa
- Catalyzes: CO2 + H2O ⇌ H2CO3
- This reaction is otherwise extremely slow without the enzyme
- Inhibited by acetazolamide (used in glaucoma, altitude sickness)
- Inhibition → less HCO3- reabsorption → metabolic acidosis
14. CLINICAL CORRELATIONS
Diabetic Ketoacidosis (DKA)
- Insulin deficiency → fatty acid mobilization → ketogenesis
- Acetoacetic acid + β-hydroxybutyric acid accumulate
- pH drops → metabolic acidosis
- Compensation: Kussmaul breathing (deep, sighing respirations) - blows off CO2
- Urine: ketonuria, glucose
Salicylate (Aspirin) Poisoning
- Direct stimulation of respiratory center → respiratory alkalosis (initial)
- Then uncoupling of oxidative phosphorylation → organic acids accumulate → metabolic acidosis
- Mixed acid-base disorder
Pyloric Stenosis / Persistent Vomiting
- Loss of HCl (H+ and Cl-)
- Results in hypochloraemic metabolic alkalosis
- Paradoxical aciduria - kidneys excrete H+ to conserve Na+ (with low Cl-, kidney uses H+)
COPD
- Chronic CO2 retention → respiratory acidosis
- Kidneys compensate by retaining HCO3- (chronic compensation)
- These patients have chronically elevated HCO3-
15. KEY FORMULAS SUMMARY
$$pH = -\log[H^+]$$
$$pK_a = -\log K_a$$
$$K_a = \frac{[H^+][A^-]}{[HA]}$$
$$\boxed{pH = pK_a + \log\frac{[A^-]}{[HA]}} \quad \text{(Henderson-Hasselbalch)}$$
$$pI = \frac{pK_a^1 + pK_a^2}{2} \quad \text{(for simple amino acids)}$$
$$pH_{blood} = 6.1 + \log\frac{[HCO_3^-]}{0.03 \times pCO_2}$$
(where 0.03 is the solubility coefficient of CO2)
16. QUICK REVISION TABLE
| Concept | Key Point |
|---|---|
| pH 7.4 = normal blood | [H+] = 40 nmol/L |
| Henderson-Hasselbalch | pH = pKa + log [base]/[acid] |
| Buffer best when | pH = pKa (±1 unit) |
| Isoelectric point | Net charge = 0; pI = (pKa1 + pKa2)/2 |
| Strongest buffer in blood | Bicarbonate (extracellular), Hemoglobin (in RBC) |
| Fastest compensation | Respiratory (minutes) |
| Most powerful/complete | Renal (hours-days) |
| DKA | Metabolic acidosis → Kussmaul breathing |
| Vomiting | Metabolic alkalosis |
| COPD | Respiratory acidosis + renal compensation |
| Carbonic anhydrase inhibitor | Acetazolamide → metabolic acidosis |
17. EXAM MNEMONICS
-
ROME: Respiratory Opposite, Metabolic Equal
- Respiratory: pH and pCO2 move in opposite directions (↑CO2 → ↓pH)
- Metabolic: pH and HCO3- move in the same direction (↓HCO3- → ↓pH)
-
pKa of bicarbonate buffer = 6.1 (remember: "six point one, the lung and kidney have fun")
-
Amino acid buffering groups: His (pKa ~6) is the only amino acid that buffers at physiologic pH - hence its abundance in hemoglobin's active site
Sources: Lippincott Illustrated Reviews Biochemistry, 8th Ed. (Unit I, Chapter 1) | Basic Medical Biochemistry - A Clinical Approach, 6th Ed. | Guyton & Hall Medical Physiology | Biochemistry Quick Compendium of Clinical Pathology 5th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.