Svt
Reading File
Finding Sources
Searching PubMed
"supraventricular tachycardia" management
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Here is a thorough overview of Supraventricular Tachycardia (SVT):
Supraventricular Tachycardia (SVT)
Definition & Scope
SVT is a broad term for any tachyarrhythmia originating above the bundle of His. In common clinical usage, "SVT" or "PSVT" refers specifically to tachycardias that are dependent on the AV node for initiation and maintenance - primarily AVNRT, AVRT, and junctional tachycardia. Technically the umbrella also includes atrial fibrillation, atrial flutter, sinus tachycardia, and atrial tachycardia, but those are usually discussed separately.
Classification of Paroxysmal SVT
| Type | Mechanism | Key Feature |
|---|---|---|
| AVNRT | Reentry within AV node / perinodal atrium | Most common (~60% of cases); retrograde P near or within QRS |
| AVRT (Orthodromic) | Reentry via accessory pathway (antegrade AV node, retrograde AP) | Narrow QRS; common in WPW |
| AVRT (Antidromic) | Reentry via AP antegrade, AV node retrograde | Wide QRS; uncommon |
| Atrial Tachycardia (AT) | Automaticity or microreentry in atrium | P wave before QRS, independent of AV node |
| Atrial Flutter (AFL) | Macroreentry around tricuspid valve | "Sawtooth" P waves; atrial rate 250-350 bpm; often 2:1 block -> 150 bpm |
| MAT | Multiple ectopic foci | ≥3 distinct P-wave morphologies; seen in COPD, CHF |
| Junctional (JET) | Automaticity in AV node | Rare in adults; AV dissociation |
- Washington Manual, p. 234
Epidemiology
- Prevalence: ~2.25/1000; incidence 35/100,000 person-years
- SVT most commonly presents between ages 12-30 in structurally normal hearts
- Women are twice as likely to develop SVT as men
- AVRT tends to present earlier (first 2 decades); AVNRT and AT present later in life
- Washington Manual, p. 235
AVNRT (Most Common Type)
Mechanism: Dual AV nodal pathways - a slow pathway (right inferior extension along tricuspid annulus) and a fast pathway. The reentry wavefront travels up the slow pathway and exits via the fast pathway. Atrial and ventricular activation occur nearly simultaneously.
ECG findings:
- Narrow QRS tachycardia, rate 150-250 bpm
- P wave hidden within or just at the end of the QRS
- Pseudo-r' in lead V1 and pseudo-S waves in leads II, III, aVF (retrograde P)
- No clear RP interval
Symptoms: Palpitations, neck pounding (cannon A waves from atrial contraction against closed tricuspid valve), dizziness. Post-tachycardia diuresis from natriuretic peptide release.
- Harrison's 22E, p. 1983
ECG Approach to Wide vs. Narrow Complex
- Regular narrow-complex tachycardia -> think AVNRT, AVRT, or AFL (2:1)
- Irregular narrow-complex -> AF, MAT, AFL with variable block
- Wide-complex tachycardia -> treat as VT until proven otherwise
- Regular + stable: trial of IV adenosine is reasonable
- Very irregular wide-complex: likely preexcited AF/flutter -> cardioversion, IV procainamide, or ibutilide
Acute Management
Treatment algorithm for hemodynamically stable narrow-complex tachycardia (PSVT):
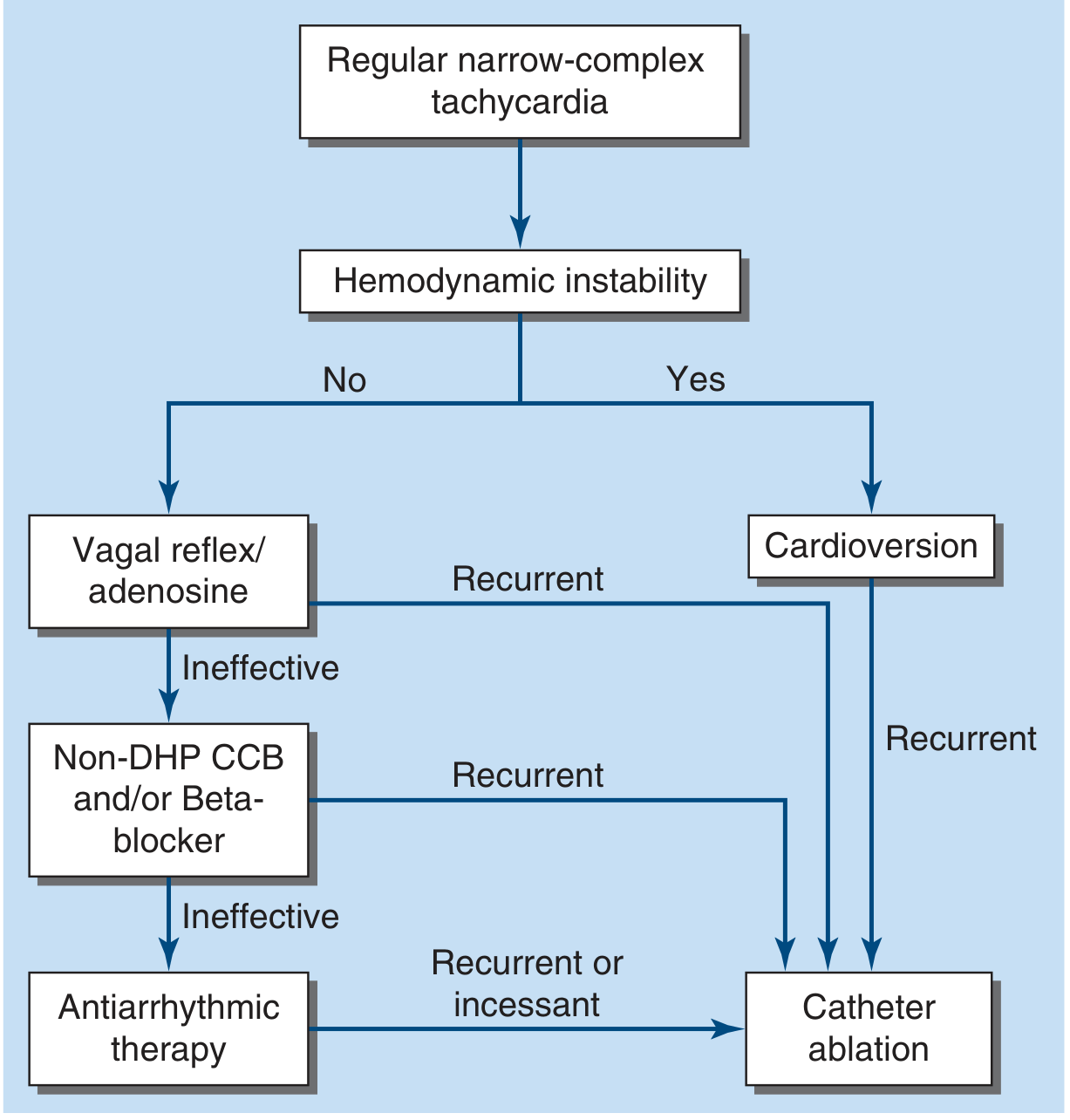
Step-by-step approach:
- Hemodynamic instability? -> Immediate synchronized DC cardioversion
- Stable -> Vagal maneuvers (Valsalva, carotid sinus massage if no carotid bruits/prior stroke)
- A 2025 network meta-analysis (PMID: 41380061) evaluated optimal vagal maneuvers in stable SVT
- Vagal maneuvers fail -> IV adenosine
- Terminates the vast majority of PSVT by transiently blocking AV conduction
- Side effects: chest pain, dyspnea, flushing, anxiety (very brief)
- Cautions: contraindicated post-cardiac transplant; use cautiously in WPW (can precipitate AF with rapid ventricular response); can aggravate bronchospasm
- Precipitates AF in up to 15% of patients
- If adenosine fails -> IV non-DHP CCB (verapamil or diltiazem) or IV beta-blocker
- Effective but may cause hypotension; longer duration of action than adenosine
- Recurrent episodes -> antiarrhythmic therapy (beta-blockers, CCBs, flecainide, propafenone)
- Recurrent/incessant or drug failure -> catheter ablation
- Harrison's 22E, p. 1986
Long-Term Management
- AVNRT: Catheter ablation of the slow AV nodal pathway - curative in >95% of patients. Risk of AV block requiring pacemaker is <1%.
- AVRT/WPW: Accessory pathway ablation
- Medical alternatives: Oral beta-blockers, verapamil, diltiazem; flecainide/propafenone for recurrent episodes
- Patients can be taught to self-terminate with Valsalva maneuver
Special Considerations
WPW Syndrome:
- Accessory pathway conducts anterogradely -> short PR (<0.12s), delta wave, wide QRS during sinus rhythm
- Orthodromic AVRT: narrow complex, clinically indistinguishable from AVNRT - treat with vagal maneuvers and adenosine
- Avoid AV nodal blocking agents (adenosine, CCBs, digoxin, beta-blockers) in preexcited AF/flutter (antidromic) - these can accelerate conduction down the AP causing VF
Pediatric SVT:
- Rate >220 bpm in infants or >180 bpm in children suggests SVT over sinus tachycardia
- AVNRT (reentrant) is the classic pediatric SVT
- Associated with Ebstein's anomaly, corrected transposition of great arteries
Wide-complex SVT vs. VT (key distinguishing features):
- Any wide-complex tachycardia of uncertain origin -> treat as VT
- AV dissociation, fusion beats, capture beats all strongly favor VT
- RBBB or LBBB morphology with preceding known bundle branch block may indicate SVT with aberrancy
Key Drug Summary
| Drug | Route | Dose | Notes |
|---|---|---|---|
| Adenosine | IV rapid push | 6 mg -> 12 mg -> 12 mg | Flush with NS; very short half-life (~10s) |
| Verapamil | IV | 2.5-5 mg slow push | Avoid in wide-complex/uncertain tachycardia |
| Diltiazem | IV | 0.25 mg/kg over 2 min | |
| Metoprolol | IV | 5 mg q5min x3 | |
| Procainamide | IV | 15-17 mg/kg loading | For preexcited AF/flutter or wide-complex |
Sources: Harrison's Principles of Internal Medicine 22E (2025), Washington Manual of Medical Therapeutics, Tintinalli's Emergency Medicine, Rosen's Emergency Medicine; 2019 ESC SVT Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.