Amblyopia in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
amblyopia treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
amblyopia patching treatment child eye
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the complete, detailed answer on amblyopia.
Amblyopia — A Detailed Overview
Definition
Amblyopia is the unilateral, or rarely bilateral, decrease in best-corrected visual acuity (VA) caused by form vision deprivation and/or abnormal binocular interaction, for which there is no identifiable pathology of the eye or visual pathway. In the absence of an organic lesion, a difference in best-corrected VA of two Snellen lines or more (or >1 log unit) between the eyes is considered diagnostic.
- Kanski's Clinical Ophthalmology, 10th ed.
The colloquial term "lazy eye" is best avoided in clinical practice, as it is often confused or conflated with strabismus — two conditions that only co-exist in about 50% of cases.
- Textbook of Family Medicine, 9th ed.
Epidemiology
- Affects approximately 4% of the population — one of the most common causes of visual loss in children.
- Most frequent cause of unilateral vision loss in children younger than 4 years.
- Half of all amblyopia patients have concomitant strabismus; the other half do not.
- Textbook of Family Medicine, 9th ed.
Pathophysiology & Critical Period
Amblyopia arises from abnormal visual experience during a critical period of visual cortex development in early childhood. The developing visual cortex is highly plastic — when one eye receives a degraded, misaligned, or suppressed image, the cortical neurons subserving that eye are "outcompeted" by those from the dominant eye, leading to a permanent reduction in cortical representation and visual acuity.
Key points:
- The sensitive/critical period during which acuity of an amblyopic eye can be improved is up to 7–8 years for strabismic amblyopia, and may extend into the teens for anisometropic amblyopia where good binocular function is present.
- In strabismic amblyopia, continued monocular suppression of the deviating eye drives the cortical changes.
- In anisometropic amblyopia, the more ametropic eye receives a chronically blurred image, acting as a mild form of form-vision deprivation.
- Kanski's Clinical Ophthalmology, 10th ed.
Classification
1. Strabismic Amblyopia
- Most common type (along with anisometropic)
- Caused by abnormal binocular interaction from persistent ocular misalignment
- Vision is worse in the consistently deviating, non-fixating eye
- Strabismus can lead to or be the result of amblyopia (bidirectional relationship)
2. Anisometropic Amblyopia
- Most common type (along with strabismus)
- Caused by a difference in refractive error between the eyes — as little as 1 dioptre can be sufficient
- The more ametropic eye receives a blurred image
- Frequently associated with microstrabismus; the two types often co-exist
- Can be seen with eyelid hemangioma or congenital ptosis inducing astigmatism
3. Stimulus Deprivation Amblyopia (Form Deprivation)
- Caused by opacities in the ocular media (e.g., congenital cataract, corneal scar, PFV) or ptosis covering the pupil
- Can be unilateral or bilateral
- Most severe form — requires urgent treatment in neonates/infants
- A unilateral cataract not treated within the earliest months of life can lead to dense, irreversible amblyopia
4. Bilateral Ametropic Amblyopia
- Results from high symmetrical refractive errors, usually hypermetropia
- Both eyes equally affected by chronic defocus
5. Meridional Amblyopia
- Caused by uncorrected astigmatism (usually >1 D) persisting beyond emmetropization in early childhood
- Results in image blur in one meridian
- Can be unilateral or bilateral
6. Occlusion (Reverse) Amblyopia
-
Iatrogenic form — amblyopia that occurs in the fellow (previously normal) eye as a result of too much patching or excessive atropine use
-
Prevented by examining at appropriate intervals (~1 week per year of age) and using part-time patching
-
Kanski's Clinical Ophthalmology, 10th ed.; Wills Eye Manual, 7th ed.
Clinical Features
Symptoms
- Usually none — often discovered incidentally on VA testing of each eye individually
- History of patching, strabismus, or muscle surgery in childhood may be elicited
- Wills Eye Manual
Signs
Critical finding:
- Poorer vision in one eye not entirely correctable with refraction and not entirely explained by organic pathology
- Central vision primarily affected; peripheral visual field usually remains normal
- In anisometropic amblyopia, the involved eye nearly always has a higher refractive error
Additional signs:
-
Crowding phenomenon: Individual letters are read more easily than a full line of letters — more pronounced in amblyopes than normal individuals; must be accounted for in preverbal children
-
Neutral-density filter effect: In reduced illumination, visual acuity of an amblyopic eye is reduced much less than in an organically diseased eye
-
A severe case may cause a trace relative afferent pupillary defect (RAPD) — care must be taken with light alignment in strabismic patients to avoid false positives
-
In deprivation amblyopia, the involved eye may be slightly smaller (microphthalmos)
-
Wills Eye Manual, 7th ed.; Kanski's Clinical Ophthalmology
Workup / Diagnosis
- History: Eye problems in childhood (misalignment, patching, surgery)?
- Ocular examination: Rule out organic cause for reduced VA
- Cover-uncover test: Evaluate eye alignment for strabismus
- Cycloplegic refraction of both eyes — mandatory to unmask anisometropia and determine refractive status
- Fundoscopy: Essential to exclude organic disease before starting treatment; organic disease and amblyopia can co-exist
- If acuity does not respond to treatment → consider electrophysiology or neuroimaging
- Wills Eye Manual, 7th ed.; Kanski's Clinical Ophthalmology, 10th ed.
VA testing in preverbal children:
- Qualitative: fixation and following behavior; occlusion resistance (strong objection to covering one eye suggests poorer acuity in the other)
- Quantitative: preferential looking tests (Teller acuity cards), Cardiff cards
- Fixation behavior graded as central/eccentric, steady/unsteady, maintained/unmaintained
Treatment
General Principles
- Exclude organic disease first before starting amblyopia treatment
- Correct the underlying refractive error with full cycloplegic refraction as the first step — spectacles alone can resolve amblyopia in 27–77% of children
- Earlier treatment → better prognosis; amblyopia is usually treatable if detected at 3–4 years, and is generally considered irreversible after age 13
- The younger the patient: more rapid improvement but greater risk of inducing reverse (occlusion) amblyopia in the fellow eye
- Better baseline VA at start of treatment → shorter duration required
- Poor compliance is the single greatest barrier to improvement
Step-by-Step Approach (Patients <12 Years)
Step 1 — Optical correction
- Prescribe full cycloplegic refraction (or symmetrically reduce hyperopia by ≥1.50 D)
- Allow 6–12 weeks of refractive adaptation — vision often improves with glasses alone
- If vision remains reduced after this period, proceed to patching/penalization
Step 2 — Occlusion (Patching) — most effective treatment
- Patch the better (non-amblyopic) eye to force use of the amblyopic eye
- Adhesive patches placed directly over the eye are most effective (patches worn over glasses risk peeking)
- 2–6 hours/day part-time patching is as effective as full-time and carries less risk
- Follow-up: 1 week per year of age (e.g., 3-year-old → 3-week follow-up)
- If no improvement after 6 months of effective occlusion → further treatment unlikely to be fruitful
- Skin irritation: apply tincture of benzoin before patching; warm compress for removal
Step 3 — Penalization with Atropine
- Atropine 1% drops instilled once daily in the fellow eye (with glasses)
- Blurs distance vision in the fellow eye, forcing use of the amblyopic eye
- Equally effective as patching in mild-to-moderate amblyopia (VA 20/100 or better)
- Effect can be enhanced by removing the hyperopic lens from the fellow eye's glasses
- Weekend-only atropine is as effective as daily atropine (ATS 4 trial: 2.3 lines improvement in both groups)
- School difficulty → use full hyperopic correction + +2.50 bifocal during school hours, or weekend-only dosing
Step 4 — Optical Degradation (Bangerter Filters / High-Plus Lens)
- Bangerter filters over the fellow eye lens provide similar outcomes to patching (ATS 10)
- High-plus lens (+9.00 D or aphakic contact lens) to blur the fellow eye image
- If child is highly myopic, remove the minus lens from the preferred eye
Key Clinical Trial Data (Amblyopia Treatment Studies — ATS)
| Trial | Key Finding |
|---|---|
| ATS 3 | Children 7–12 yr: patching/atropine + glasses achieved 20/25 in 36% vs. 14% glasses alone (moderate amblyopia) |
| ATS 4 | Daily vs. weekend atropine → identical 2.3-line improvement |
| ATS 5 | Glasses alone improved ≥2 lines in 77%; resolved amblyopia in 27% |
| ATS 6 | 2 hrs/day patching → 3.7 lines improvement in severe amblyopia at 17 weeks |
| ATS 10 | Bangerter filters ≈ patching for moderate amblyopia |
| ATS 13 | Glasses alone for strabismic amblyopia → mean 2.6-line improvement; 32% resolution |
Special Situations
- Strabismic amblyopia: Delay strabismus surgery until VA is equalized or maximal improvement achieved in the amblyopic eye
- Deprivation amblyopia (media opacity): Remove opacity urgently + immediately begin patching of the fellow eye
- Bilateral ametropic amblyopia: Full refractive correction; bilateral patching rarely needed
- Patients >12 years: Treatment is still possible, though less effective; some improvement reported even in adults with dichoptic therapy and newer technologies
- Treatment failure or outside treatment age: Protective polycarbonate glasses should be worn to safeguard the better eye — the "one-eyed athlete rule" applies (sports eye protection mandatory)
Adjusting Treatment
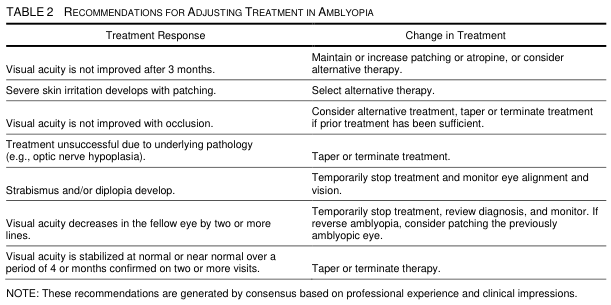
Key triggers for treatment modification:
- No VA improvement after 3 months → increase or change modality
- VA decreases ≥2 lines in the fellow eye → stop treatment, consider reverse amblyopia
- VA stabilized at normal/near-normal on 2+ visits → taper/terminate
- Strabismus or diplopia develops → temporarily stop and monitor alignment
Newer & Emerging Treatments
- Dichoptic therapy / Virtual reality: Presents different images to each eye simultaneously to force binocular cooperation; shown effective in some trials; particularly relevant for older children and adults (see [VR systematic review, PMID 39141772])
- Perceptual learning: Computer-based visual training tasks aimed at cortical plasticity
- Pharmacological approaches: Levodopa, citicoline (investigational — limited evidence)
- Binocular iPad games: Dichoptic approach showing promise in pediatric trials
A recent 2025 systematic review ([PMID 41971201]) reviews conventional and emerging treatment strategies specifically for adult amblyopia, where traditional approaches have limited efficacy.
Prognosis
- Best prognosis: Treatment started at 3–4 years during the critical period
- Generally irreversible after age 13 (though not absolutely so)
- Anisometropic amblyopia may be amenable to treatment into the teens if binocular function is preserved
- Recurrence can occur after treatment — part-time maintenance patching may be needed
- If treatment is successful and then stopped, regular monitoring for recurrence is essential
- Failure to treat leads to permanent unilateral visual impairment
Screening
Vision screening programs target the 3–4 year age group as the optimal window. Photoscreening and autorefraction devices can detect risk factors (anisometropia, strabismus, media opacity) before VA testing is reliable. Pediatricians should perform the corneal light reflex test, cover test, and red reflex at every well-child visit.
Key Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.
- Wills Eye Manual, 7th ed. — Section 8.7
- Textbook of Family Medicine, 9th ed. — Chapter 17
- ATS trial data (Amblyopia Treatment Studies, PEDIG)
- Recent evidence: [Treatment strategies for amblyopia in adults, PMID 41971201] (2025 systematic review); [VR/eye tracking in pediatric ophthalmology, PMID 39141772] (2024 systematic review)
This is a shared conversation. Sign in to Orris to start your own chat.