Ulcerative colitis
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"ulcerative colitis"[MeSH Terms] AND management
Reading File
Searching PubMed
"ulcerative colitis"[MeSH Terms] AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
I now have all the material needed for a comprehensive, well-organized answer. Here it is:
Ulcerative Colitis
Definition & Overview
Ulcerative colitis (UC) is a chronic, relapsing inflammatory bowel disease (IBD) that is limited exclusively to the colon and rectum. Unlike Crohn disease, which may involve any segment of the GI tract and causes transmural inflammation, UC produces continuous mucosal and submucosal inflammation starting at the rectum and extending proximally. There are no skip lesions, no fistulae, and no granulomas.
Epidemiology
- Most common presentation is in the teenage years and early 20s, with a smaller second peak beyond the 7th decade
- Equal sex distribution (F:M = 1:1)
- More common among people of European (especially Ashkenazi Jewish) descent - occurring 3-5 times more often in this population
- Peak age of onset: 20-40 years
Pathogenesis
UC results from a complex interplay of genetic predisposition, immune dysregulation, and gut microbiota. Genetic studies involving >75,000 subjects have identified numerous susceptibility loci shared with Crohn disease, though each condition has distinct genetic signatures. The microbiome is thought to play a key role - infectious enteritis may trigger mucosal immune activation in susceptible individuals. Notably, up to 75% of UC patients have perinuclear antineutrophil cytoplasmic antibodies (p-ANCA), versus only ~10% in Crohn disease. Smoking cessation is uniquely associated with onset or flares of UC (in contrast to Crohn disease, where smoking may worsen disease).
Pathology
Gross Morphology
UC always involves the rectum and extends proximally in a continuous, uninterrupted fashion. Disease limited to the rectum/sigmoid is called proctosigmoiditis; involvement of the entire colon is pancolitis.
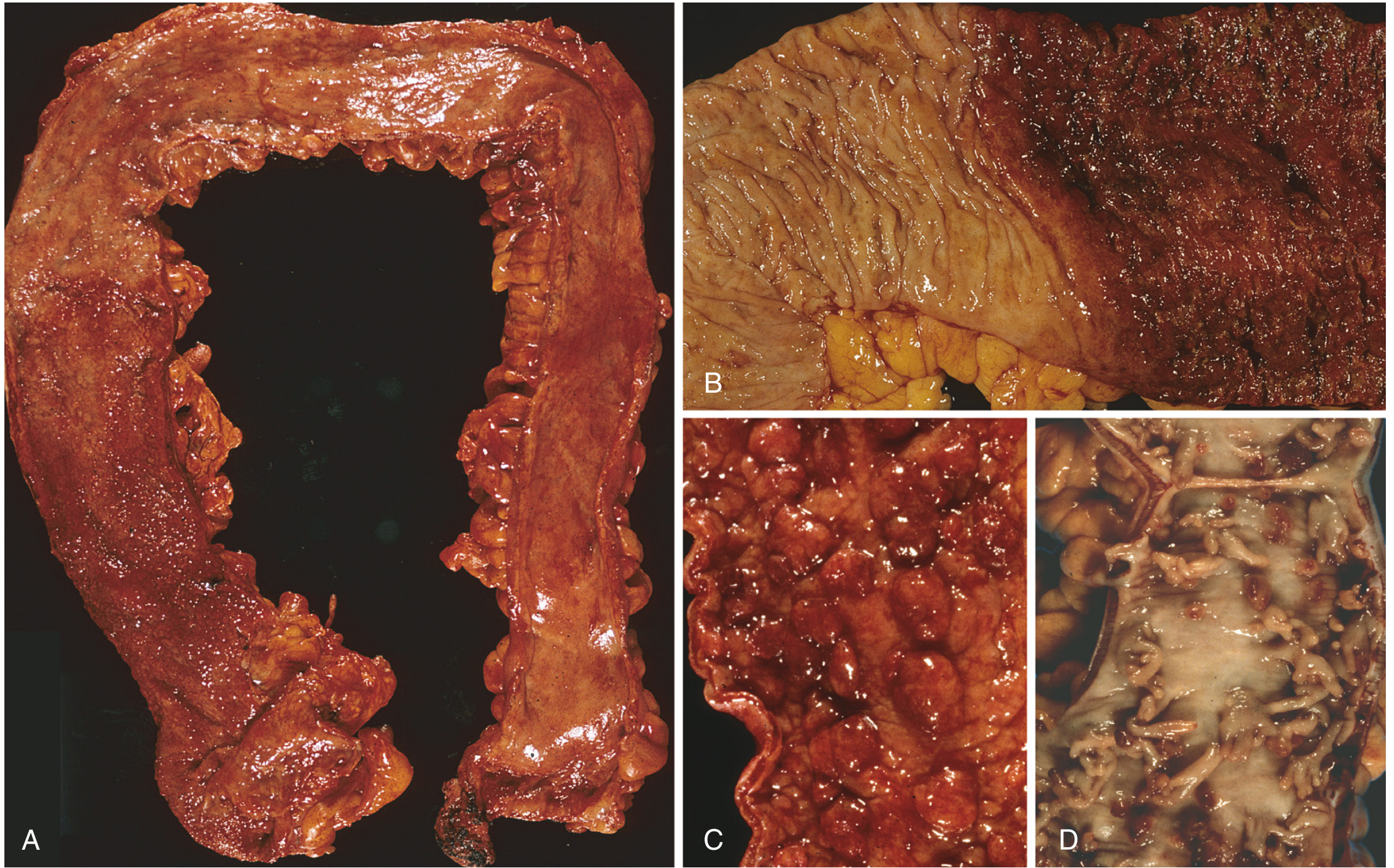
Gross pathology of UC - Robbins, Cotran & Kumar Pathologic Basis of Disease
- In mild disease: granular, hyperemic, edematous mucosa
- In severe disease: broad-based superficial ulcers (not deep/knife-like as in Crohn)
- Pseudopolyps form from islands of regenerating mucosa after recurrent attacks - a marker of more severe, long-standing disease
- Mucosal bridges can form when pseudopolyp tips fuse
- Chronic disease: mucosal atrophy, loss of normal fold pattern, colon shortening
Key distinction from Crohn disease:
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Location | Ileum ± colon (any GI site) | Colon only |
| Pattern | Skip lesions | Continuous |
| Depth | Transmural | Mucosal/submucosal |
| Ulcers | Deep, knife-like | Superficial, broad-based |
| Fistulae | Yes | No |
| Granulomas | Yes (~35%) | No |
| Toxic megacolon | No | Yes |
Microscopic Findings
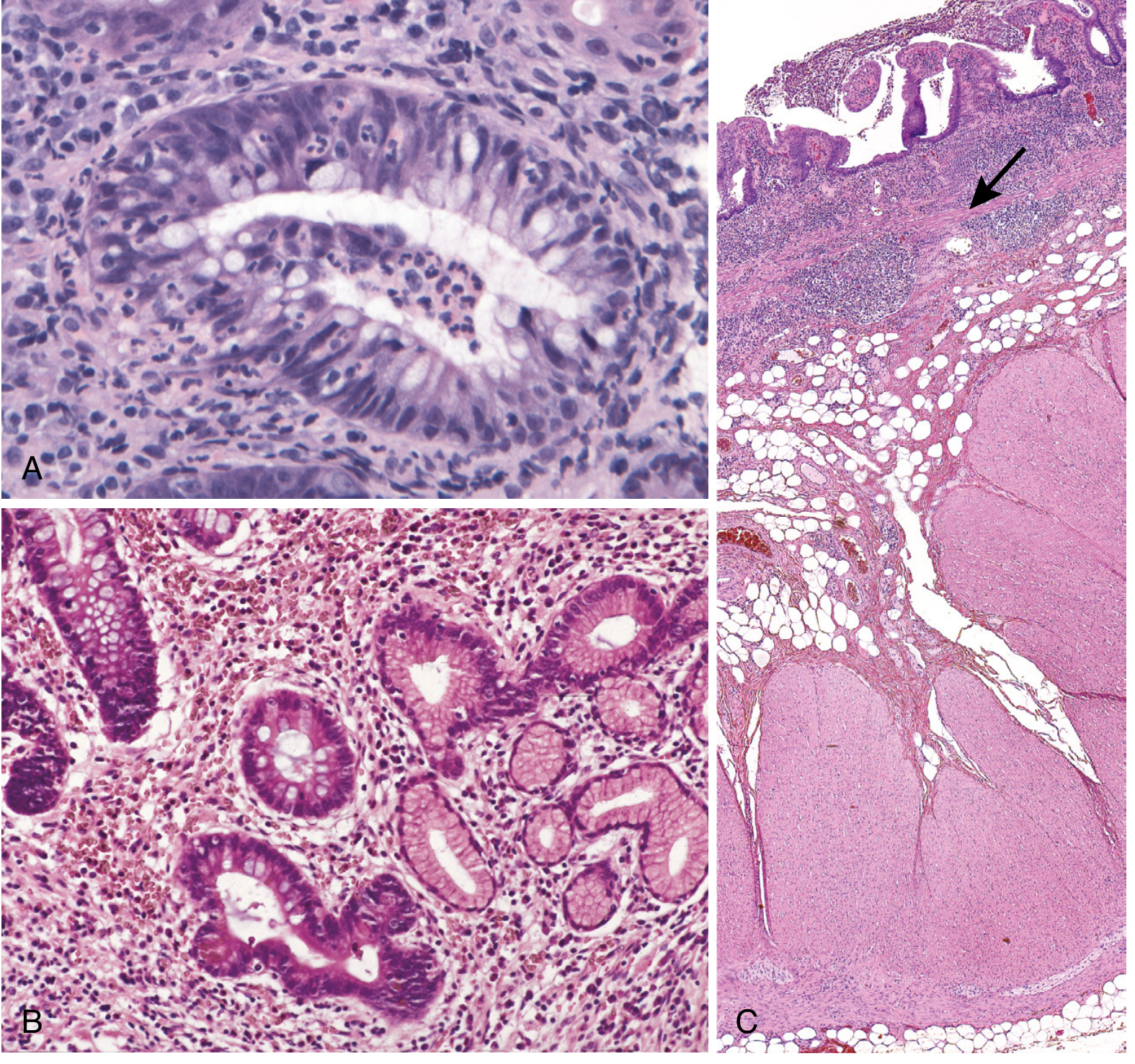
Histopathology of UC - Robbins, Cotran & Kumar Pathologic Basis of Disease
- Acute/early: epithelial necrosis, acute inflammatory infiltrate in the lamina propria, cryptitis and crypt abscesses
- Chronic: predominantly lymphocytic infiltrate, crypt architectural distortion, crypt branching and dropout
- No granulomas (distinguishes from Crohn)
- Inflammation is confined to the mucosa (above the muscularis mucosae)
Clinical Features
Symptoms at Diagnosis
At diagnosis:
- 14-37% have pancolitis
- 36-41% have disease extending beyond the rectum
- 44-49% have proctosigmoiditis
Cardinal symptoms:
- Hematochezia (bloody diarrhea) - the hallmark
- Diarrhea with mucus
- Tenesmus (constant urge to defecate)
- Lower abdominal pain/cramps, relieved temporarily by defecation
- Urgency to defecate
With extensive/severe disease: weight loss, fever, fatigue (anemia), nausea, peripheral edema (hypoalbuminemia)
With proctitis/proctosigmoiditis: paradoxically, constipation may occur
Extraintestinal Manifestations
These affect up to 10-20% of patients:
| System | Manifestations |
|---|---|
| Joints | Peripheral arthralgia/arthritis, ankylosing spondylitis, sacroiliitis |
| Skin | Erythema nodosum (10-15%), pyoderma gangrenosum (1-2%) |
| Eyes | Uveitis, episcleritis (5-15%) |
| Liver | Primary sclerosing cholangitis (2-7.5%; 70-80% of PSC patients have IBD) |
| Renal | Uric acid stones (due to volume depletion) |
Diagnosis
Endoscopy
The primary diagnostic tool. Findings start in the rectum and extend proximally in a continuous pattern:
- Early: diffuse mucosal erythema, loss of normal vascular pattern, granularity
- Moderate: friability, contact bleeding
- Severe: ulceration
Histopathology
Crypt distortion, continuous mucosal inflammation from rectum, absence of granulomas, absence of small bowel disease.
Laboratory Findings
- Anemia - from chronic disease, blood loss, or nutritional deficiency
- Elevated ESR and CRP (nonspecific inflammatory markers)
- Fecal calprotectin - elevated in active disease, lower in remission
- Leukocytosis (mild = active disease; marked = abscess/suppurative complication)
- Hypoalbuminemia - malnutrition from active disease
Serologic Markers
- p-ANCA positive in ~55% of UC patients (versus 20% in Crohn)
- ASCA (anti-Saccharomyces cerevisiae antibodies) present in 40-70% of Crohn patients but <15% of UC patients
- ASCA+/pANCA- pattern: 55% sensitivity, 93% specificity for Crohn disease
- Note: serologic markers are supportive - cannot independently diagnose IBD
Severity Classification (Mayo Score / Truelove & Witts)
Mild UC: <4 stools/day, minimal blood, normal vitals
Moderate UC: 4-6 stools/day, some blood, mild systemic features
Severe UC: >6 bloody stools/day, fever >37.8°C, tachycardia, anemia, elevated ESR
Treatment
The goals are to induce and maintain mucosal healing and clinical remission while minimizing side effects.
Step-Up Approach by Severity
Mild to Moderate Disease
Proctitis:
- Topical 5-ASA (enema/suppository) - superior to topical corticosteroids
- Combine with oral 5-ASA for faster response
- If 5-ASA fails: corticosteroid enemas/suppositories/foam
Extensive colitis (proximal to splenic flexure):
- Oral 5-ASA (first-line; efficacy increases with dose)
- Supplement with 5-ASA enemas even for extensive disease
- If inadequate response after 3-4 weeks, or >5-6 bowel movements/day: oral corticosteroids (prednisone 40 mg/day, taper over 8-12 weeks)
- Budesonide MMX provides incremental benefit
Severe Colitis
- IV methylprednisolone 40-60 mg/day
- If no response to IV corticosteroids within 3-5 days, or no complete response within 7-10 days: options are colectomy, infliximab, or IV cyclosporine
- Tofacitinib (JAK inhibitor, 10 mg twice daily) - improves symptoms and maintains remission in moderate-to-severe UC
- Ozanimod (S1P receptor modulator, 1 mg daily) - effective for induction and maintenance
Steroid-Dependent/Refractory Disease
If requiring >15 mg/day prednisone for >4 months, initiate:
- Biologics: infliximab, adalimumab, golimumab, vedolizumab, ustekinumab (vedolizumab may be the most efficacious and safe)
- Immunomodulators: azathioprine, 6-mercaptopurine, tofacitinib, upadacitinib, ozanimod
Drug Categories
| Drug Class | Examples | Role |
|---|---|---|
| 5-ASA (aminosalicylates) | Mesalamine, sulfasalazine, olsalazine, balsalazide | Mild-moderate UC; maintenance |
| Corticosteroids | Prednisone, methylprednisolone, budesonide MMX | Flare induction only (not maintenance) |
| Immunomodulators | Azathioprine, 6-mercaptopurine, methotrexate, tofacitinib, upadacitinib | Steroid-sparing; maintenance |
| Anti-TNF biologics | Infliximab, adalimumab, golimumab | Moderate-severe; maintenance |
| Anti-integrin | Vedolizumab | Moderate-severe; maintenance (gut-selective) |
| Anti-IL-12/23 | Ustekinumab | Moderate-severe; maintenance |
| S1P modulator | Ozanimod | Moderate-severe; induction + maintenance |
Maintenance Therapy
- Virtually all patients should receive maintenance 5-ASA to reduce recurrence - unless on biologics (5-ASA adds little benefit once biologics are started)
- Corticosteroids are not effective for maintenance and should not be used chronically
- Azathioprine, 6-mercaptopurine, vedolizumab, infliximab, adalimumab, golimumab, ustekinumab, tofacitinib, upadacitinib, and ozanimod are all options for maintenance in refractory disease
Complications
Toxic Megacolon
The most significant acute complication. Defined as colonic dilation >6 cm with:
- Fever, tachycardia, leukocytosis
- Abdominal tenderness, absent bowel sounds
- Risk of perforation and peritonitis
Management: NPO + NG suction, IV fluids, broad-spectrum antibiotics, IV corticosteroids, avoid antidiarrheals and anticholinergics (precipitate megacolon). If no improvement within 24-48 hours, surgical colectomy is indicated.
Colorectal Cancer
- Risk begins after 8 years of disease and increases progressively
- Related to: extent of disease, duration of disease, presence of primary sclerosing cholangitis, and family history of colorectal cancer
- Surveillance: colonoscopy with chromoendoscopy or narrow-band imaging, beginning 8 years after onset, repeated every 1-2 years
- Dysplasia found on random biopsies without discrete polypoid lesion = indication for colectomy
Pouchitis
After ileal pouch-anal anastomosis surgery, inflammation of the ileal pouch (pouchitis) can occur. Treatment: metronidazole 500 mg TID or ciprofloxacin 500 mg BID for 2 weeks.
Surgical Treatment
Colectomy is curative for UC (unlike Crohn disease where surgery is not curative).
Indications for surgery:
- Toxic megacolon not responding to 48 hours of medical therapy
- Severe fulminant attack unresponsive to treatment
- Refractory disease (colectomy rates: ~3% at 1 year, ~7% at 5 years, ~10% at 10 years - reduced dramatically by biologics)
- Dysplasia/cancer
Procedure: Proctocolectomy with Brooke ileostomy (standard), or ileal pouch-anal anastomosis (IPAA) to preserve anal function and avoid permanent ileostomy. Note: IPAA significantly reduces fertility in women.
Prognosis
- More than half of patients have clinically mild disease
- Almost all experience at least one relapse over 10 years
- The incidence of colectomy has fallen sharply over the past 20 years due to biologics
- Although colectomy cures intestinal disease, extraintestinal manifestations may persist after surgery
- Fertility is usually normal or minimally impaired, though active disease during pregnancy carries greater fetal risk than most medications
Sources: Goldman-Cecil Medicine (25th ed.), Robbins & Cotran Pathologic Basis of Disease (10th ed.), Yamada's Textbook of Gastroenterology (7th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.