help me on caselresentation of P parptid swelling difficult airway case anaesthesia md
parotid gland swelling difficult airway anaesthesia management case presentation MD
Case Presentation: Parotid Swelling with Difficult Airway - Anaesthesia MD
CASE VIGNETTE
1. HISTORY
Chief Complaint
History of Present Illness
- Mass is firm, non-tender, fixed in later stage / mobile in early stage
- No fever, no pus, no skin erythema (features against acute parotitis)
- Dysphagia or dysphonia: absent / present (note if present - indicates deep lobe or parapharyngeal extension)
- No facial nerve weakness (malignancy less likely, but must rule out)
- No recent weight loss, no cervical lymphadenopathy
Past History
- No prior head/neck surgery or radiotherapy (important - radiation makes mask ventilation difficult)
- No diabetes, hypertension, immunosuppression
Airway-Relevant History
- Snoring/OSA symptoms
- Previous anaesthesia and intubation difficulty
- Neck mobility, dental status
2. PHYSICAL EXAMINATION
General
- Vitals stable; SpO2 on room air: 98%
- Anxious but cooperative
Airway Assessment (MUST document all of the following)
| Parameter | Finding in This Patient |
|---|---|
| Mouth opening | < 2.5 cm (trismus) - GRADE III DIFFICULT |
| Mallampati class | III-IV |
| Thyromental distance | < 6 cm (concern) |
| Sternomental distance | < 12.5 cm |
| Neck extension | Limited if large mass |
| Upper lip bite test | Class II-III |
| Neck circumference | Note any obesity |
| Buck teeth / macroglossia | Note |
"Other clues to a potentially difficult laryngoscopy include limited neck extension (<35°), a distance between the tip of the patient's mandible and hyoid bone of less than 7 cm, a sternomental distance of less than 12.5 cm with the head fully extended." - Morgan & Mikhail's Clinical Anesthesiology, 7e
Local Examination - Parotid
- Right pre-auricular swelling, ~5 x 4 cm, firm, non-tender, non-pulsatile
- Overlying skin normal, no tethering
- Facial nerve: all branches intact (House-Brackmann Grade I)
- No Stensen's duct discharge
- No cervical nodes
ENT examination
- Oropharyngeal bulk / tonsillar displacement if deep lobe extension
3. INVESTIGATIONS
Imaging (critical for anaesthesia planning)
- Delineates extent of mass - superficial vs. deep lobe vs. parapharyngeal extension
- Airway displacement: "The physical examination should look for tumor displacement of the airway, as well as impaired temporomandibular joint (TMJ) mobility and other predictors of airway difficulties. Available head and neck CT scans or MRI studies should be reviewed with the surgical team, with a focus on airway issues." - Miller's Anesthesia, 10e
- Assess parapharyngeal space involvement
- Pleomorphic adenoma: most common benign parotid neoplasm (85% in parotid, 90% in tail of superficial lobe) - slow-growing, painless, firm
- Cytology: epithelial + mesenchymal elements
Routine Labs
- CBC, RFT, LFT, coagulation, blood grouping
- ECG, CXR (posterior-anterior)
- Thyroid function if suspicion
4. PREOPERATIVE ANAESTHESIA ASSESSMENT
ASA Physical Status
- ASA II (healthy adult, no comorbidities) or ASA III if OSA/HTN
Difficult Airway Predictors Checklist
- L - Look externally: parotid mass, neck swelling, limited mouth opening
- E - Evaluate 3-3-2 rule: mouth opening <3 fingers, hyoid-chin <3 fingers, thyroid-mouth floor <2 fingers
- M - Mallampati: III-IV
- O - Obstruction: NO frank obstruction but trismus limits access
- N - Neck mobility: possibly restricted
5. ANAESTHETIC PLAN
Pre-operative Preparation
- Informed consent including risk of awake intubation, tracheostomy, facial nerve injury
- Multidisciplinary team: Anaesthesiologist + Surgeon (ENT surgeon scrubbed and ready for surgical airway)
- Equipment checklist:
- Flexible fiberoptic bronchoscope (primary tool)
- Video laryngoscope (McGrath / GlideScope / C-MAC)
- Bougie, multiple ETT sizes (6.0, 6.5, 7.0)
- Supraglottic airway devices: LMA ProSeal / i-gel (as backup)
- Emergency surgical airway kit (cricothyrotomy/tracheostomy set) - opened and ready
- Anterior commissure (Hollinger) laryngoscope
- Neck prepped and draped before induction
- IV access: Two large-bore IVs
- Monitors: SpO2, ETCO2, ECG, NIBP, temperature, nerve stimulator (facial nerve monitoring during surgery - therefore muscle relaxants avoided after intubation)
Pre-medication
- Tab. Diazepam 5 mg oral night before (anxiolysis, careful if airway concern)
- Inj. Glycopyrrolate 0.2 mg IM 30 min prior: dries secretions, antisialagogue, does NOT cross BBB
- Avoid: Heavy parenteral sedation - risk of losing airway
"Glycopyrrolate would be a good choice of premedication because it minimizes upper airway secretions without crossing the blood-brain barrier. Parenteral sedatives should be very carefully titrated. Dexmedetomidine and ketamine could be used as sedatives and preserve respiratory effort." - Morgan & Mikhail's Clinical Anesthesiology, 7e
Airway Strategy: AWAKE FIBEROPTIC INTUBATION (AFOI)
"Induction of anesthesia should be delayed until after the airway has been secured. Useful alternatives include awake fiberoptic intubation, awake video laryngoscopy, or awake use of optical stylets." - Morgan & Mikhail's Clinical Anesthesiology, 7e
- Nebulised 4% lignocaine (4 mL) for oropharynx and upper airway
- Gargle with 4% lignocaine
- 10% lignocaine spray to posterior pharynx
- Bilateral glossopharyngeal nerve blocks: 2 mL 2% lignocaine injected into base of palatoglossal arch (anterior tonsillar pillar) with 25G spinal needle - blocks posterior 1/3 tongue and oropharynx sensation
- Superior laryngeal nerve (SLN) block (bilateral): 3 mL 2% lignocaine injected 1 cm below greater cornu of hyoid bone, through thyrohyoid membrane - anaesthetises infraglottic larynx
- Transtracheal block: 3 mL 2% lignocaine injected through cricothyroid membrane, patient asked to inhale-cough to spray subglottically
- Total lignocaine dose MUST NOT exceed 3 mg/kg (toxicity risk)
"Bilateral superior laryngeal nerve blocks and a trans tracheal block would anesthetize the airway below the epiglottis." - Morgan & Mikhail's Clinical Anesthesiology, 7e
- Inj. Dexmedetomidine: 1 mcg/kg IV over 10 min loading, then 0.3-0.7 mcg/kg/hr infusion
- Provides excellent sedation, analgesia, anxiolysis
- Preserves respiratory effort and airway tone
- Alternatively: Ketamine 0.5 mg/kg IV (preserves airway reflexes and spontaneous ventilation)
- Supplemental O2 via nasal cannula (THRIVE - Transnasal Humidified Rapid Insufflation Ventilatory Exchange, if available) - prolongs safe apnoea time
- Lubricate and vasoconstrict nostril: Xylometazoline drops + 4% lignocaine to nasal mucosa
- Pass warmed, lubricated 6.0 or 6.5 mm cuffed ETT over bronchoscope
- Advance fiberoptic scope through nostril → nasopharynx → visualise epiglottis → pass through glottis → confirm tracheal rings and carina
- Railroad ETT over the bronchoscope into trachea
- Confirm position with ETCO2 waveform + bilateral breath sounds
- Secure tube, inflate cuff
- Inj. Propofol 1-2 mg/kg IV (titrated) OR Inj. Thiopentone 3-5 mg/kg
- Single intubating dose of Inj. Succinylcholine 1.5 mg/kg OR Inj. Rocuronium 0.6 mg/kg for induction only
- No further muscle relaxants intraoperatively (facial nerve monitoring requirement)
Intraoperative Maintenance
- TIVA (Total IV Anaesthesia): Propofol infusion 50-150 mcg/kg/min + Remifentanil 0.1 mcg/kg/min
- OR Sevoflurane 1-2% in O2/air + Remifentanil infusion
- Avoid neuromuscular blockers after intubation - surgeon must use facial nerve stimulator
- Patient in head-up 15-20° (reduces venous ooze), head turned to LEFT (operative side up - right parotid)
- Throat pack inserted (document and remove at end)
- Eyes protected with padding/tape
"For this reason, the surgical team usually requests that muscle relaxants be avoided after endotracheal intubation has been achieved... A single, small dose of rocuronium to facilitate endotracheal intubation is often employed, followed by sevoflurane anesthesia in conjunction with a remifentanil infusion (e.g., 0.1 mcg/kg/min) to provide immobility." - Miller's Anesthesia, 10e
Monitoring
- Standard ASA monitors + ETCO2
- Neuromuscular monitoring (Train-of-Four) to confirm reversal
- Facial nerve integrity monitoring (by surgeon, requires zero paralysis)
- Temperature, urine output
6. ASA DIFFICULT AIRWAY ALGORITHM
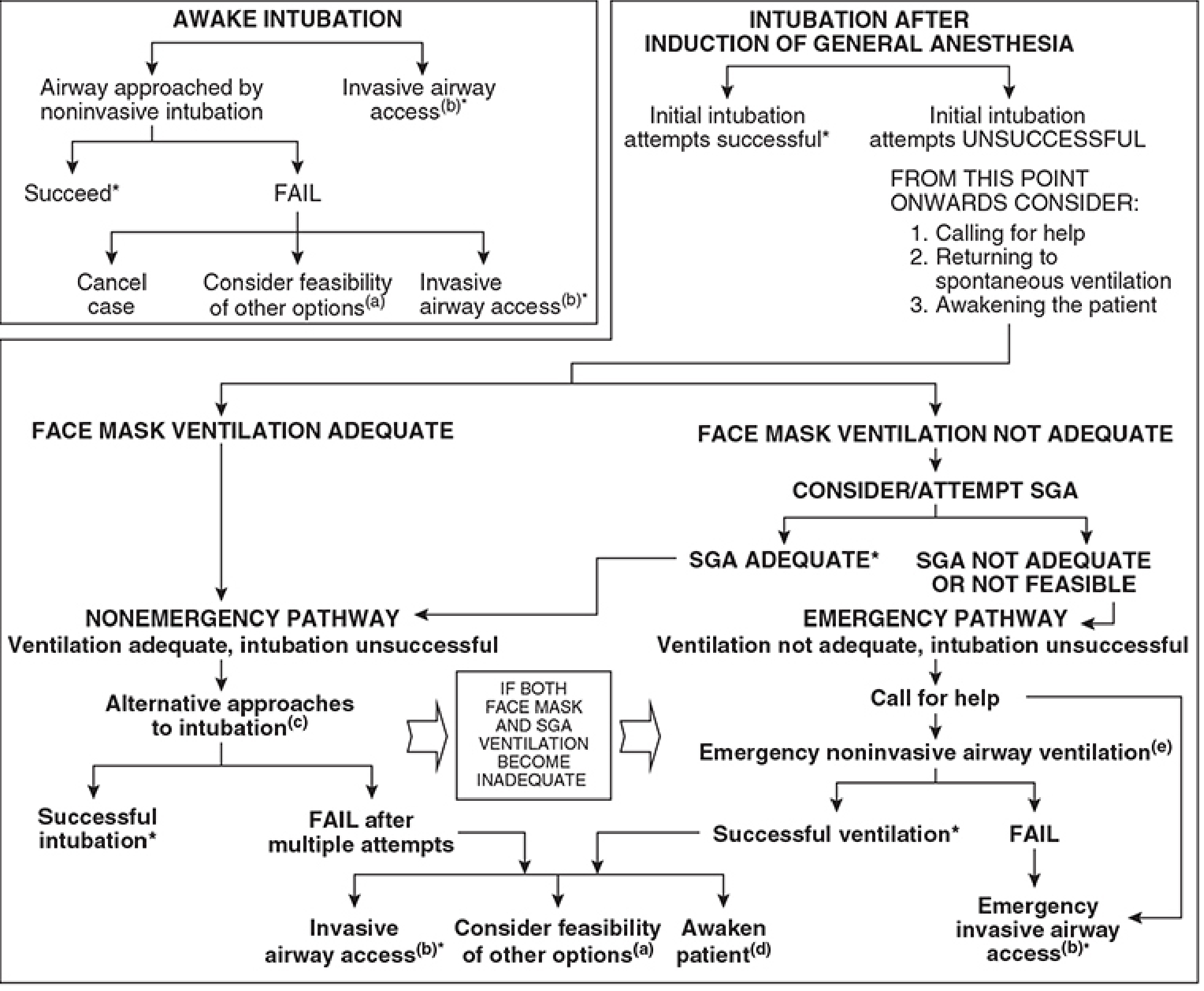
- Anticipated difficult airway → AWAKE INTUBATION pathway (left arm of algorithm)
- If awake intubation fails → Cancel case / Invasive airway access
- Surgical team on standby for emergency surgical airway at all times
7. CANNOT INTUBATE - CANNOT OXYGENATE (CICO) PROTOCOL
- Call for help immediately
- Attempt LMA / i-gel insertion as rescue oxygenation (SGA)
- If SGA fails → Emergency front-of-neck access (FONA)
- Cricothyrotomy (needle/surgical) - fastest
- Emergency tracheostomy by ENT surgeon (preferred if already scrubbed)
"Once a 'cannot intubate, cannot ventilate' situation has been identified, immediate consideration should be given to providing surgical airway access." - Cummings Otolaryngology Head and Neck Surgery
8. POSTOPERATIVE MANAGEMENT
Extubation Strategy (equally important - "difficult extubation")
- Extubate ONLY when patient is fully awake, following commands, with adequate neuromuscular reversal (TOF ratio >0.9)
- Consider: Airway Exchange Catheter (AEC) left in situ before extubation (allows reintubation if needed)
- Patient positioned head-up 30-45°
- Decadron (Dexamethasone) 8 mg IV given intraoperatively reduces postoperative edema
- Post-extubation monitoring in high dependency unit (HDU) for minimum 4 hours
Analgesia (Multimodal)
- Inj. Paracetamol 1g IV 8 hourly
- Inj. Ketorolac 30 mg IV (avoid if risk of bleeding)
- Inj. Morphine 0.1 mg/kg IV PRN (with antiemetic cover)
- Wound infiltration by surgeon with 0.25% Bupivacaine
PONV Prophylaxis
- Inj. Ondansetron 4 mg IV at end of surgery
- Inj. Dexamethasone 8 mg IV (also reduces edema)
- Total I&V: head-up position, avoid opioid excess
Watch for Complications
- Haematoma - can cause rapid airway compromise → emergency reintubation/evacuation
- Facial nerve palsy (temporary or permanent)
- Frey's syndrome (auriculotemporal nerve - gustatory sweating) - late
- Sialocele / salivary fistula - late
- "Anaesthesia mumps" - rare complication: acute postoperative parotid swelling due to Stensen's duct obstruction or backflow of air (pneumoparotitis) - can cause airway compromise in severe cases
9. DISCUSSION POINTS FOR MD EXAM VIVA
Q: Why is awake intubation preferred here?
Q: Why no muscle relaxants intraoperatively?
Q: What if awake fiberoptic fails?
Q: Role of dexmedetomidine in difficult airway?
Q: Pathology of parotid swelling (common causes)?
- Benign: Pleomorphic adenoma (most common, 85%), Warthin's tumour (bilateral in 10%)
- Malignant: Mucoepidermoid carcinoma (most common malignant), adenoid cystic carcinoma
- Inflammatory: Acute bacterial parotitis, mumps, Sjogren's syndrome, sarcoidosis
- Other: HIV parotitis, lymphoma
Q: Anaesthesia mumps - what is it?
SUMMARY TABLE
| Phase | Key Action |
|---|---|
| Preop | CT/MRI airway review, AFOI decision, glycopyrrolate, Dexmedetomidine sedation |
| Induction | Awake fiberoptic nasal intubation, topical + nerve block anaesthesia |
| Maintenance | TIVA / Sevoflurane + Remifentanil, NO neuromuscular blockers after induction |
| Emergence | Fully awake extubation, AEC in situ, head-up, HDU |
| CICO rescue | SGA → Emergency FONA (cricothyrotomy/tracheostomy) |
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Difficult Airway Algorithm & Awake Intubation
- Miller's Anesthesia, 10e - Parotid and Salivary Gland Surgery
- Cummings Otolaryngology Head and Neck Surgery - Difficult Airway in Head & Neck Surgery
i want a pdf vverbatium not even a singke word missed
mkdir -p /home/daytona/workspace/parotid-airway-case && ls /home/daytona/workspa…
~/parotid-airway-case/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import ListFlowable, ListItem
OUTPUT = "/home/daytona/workspace/parotid-airway-case/Parotid_Swelling_Difficult_Airway_Case_Presentation.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=2*cm,
leftMargin=2*cm,
topMargin=2*cm,
bottomMargin=2*cm,
title="Case Presentation: Parotid Swelling with Difficult Airway - Anaesthesia MD",
author="Orris AI Medical Assistant"
)
styles = getSampleStyleSheet()
# Custom styles
title_style = ParagraphStyle(
'CustomTitle',
parent=styles['Title'],
fontSize=18,
textColor=colors.HexColor('#1a237e'),
spaceAfter=6,
spaceBefore=0,
alignment=TA_CENTER,
fontName='Helvetica-Bold'
)
subtitle_style = ParagraphStyle(
'Subtitle',
parent=styles['Normal'],
fontSize=11,
textColor=colors.HexColor('#37474f'),
spaceAfter=4,
alignment=TA_CENTER,
fontName='Helvetica'
)
h1_style = ParagraphStyle(
'H1',
parent=styles['Heading1'],
fontSize=13,
textColor=colors.white,
spaceBefore=14,
spaceAfter=4,
fontName='Helvetica-Bold',
backColor=colors.HexColor('#1a237e'),
leftIndent=-10,
rightIndent=-10,
borderPad=5,
)
h2_style = ParagraphStyle(
'H2',
parent=styles['Heading2'],
fontSize=11,
textColor=colors.HexColor('#1a237e'),
spaceBefore=10,
spaceAfter=3,
fontName='Helvetica-Bold',
borderPad=2,
)
h3_style = ParagraphStyle(
'H3',
parent=styles['Heading3'],
fontSize=10,
textColor=colors.HexColor('#0d47a1'),
spaceBefore=7,
spaceAfter=2,
fontName='Helvetica-Bold',
)
body_style = ParagraphStyle(
'Body',
parent=styles['Normal'],
fontSize=9.5,
leading=14,
spaceAfter=4,
spaceBefore=1,
fontName='Helvetica',
alignment=TA_JUSTIFY,
)
bullet_style = ParagraphStyle(
'Bullet',
parent=styles['Normal'],
fontSize=9.5,
leading=13,
spaceAfter=2,
spaceBefore=1,
leftIndent=14,
fontName='Helvetica',
)
sub_bullet_style = ParagraphStyle(
'SubBullet',
parent=styles['Normal'],
fontSize=9,
leading=12,
spaceAfter=1,
spaceBefore=0,
leftIndent=28,
fontName='Helvetica',
textColor=colors.HexColor('#333333'),
)
quote_style = ParagraphStyle(
'Quote',
parent=styles['Normal'],
fontSize=9,
leading=13,
spaceAfter=4,
spaceBefore=4,
leftIndent=16,
rightIndent=8,
fontName='Helvetica-Oblique',
textColor=colors.HexColor('#1565C0'),
backColor=colors.HexColor('#E3F2FD'),
borderPad=6,
borderColor=colors.HexColor('#1565C0'),
borderWidth=1,
borderRadius=3,
)
highlight_style = ParagraphStyle(
'Highlight',
parent=styles['Normal'],
fontSize=9.5,
leading=13,
spaceAfter=3,
spaceBefore=3,
leftIndent=8,
rightIndent=8,
fontName='Helvetica-Bold',
textColor=colors.HexColor('#B71C1C'),
backColor=colors.HexColor('#FFEBEE'),
borderPad=5,
)
table_header_style = ParagraphStyle(
'TableHeader',
fontSize=9,
fontName='Helvetica-Bold',
textColor=colors.white,
alignment=TA_CENTER,
leading=11,
)
table_cell_style = ParagraphStyle(
'TableCell',
fontSize=8.5,
fontName='Helvetica',
textColor=colors.black,
leading=11,
alignment=TA_LEFT,
)
story = []
# ── TITLE PAGE ──────────────────────────────────────────────────────────────
story.append(Spacer(1, 1.2*cm))
story.append(Paragraph("CASE PRESENTATION", title_style))
story.append(Paragraph("Parotid Swelling with Difficult Airway", ParagraphStyle(
'MainTitle', parent=title_style, fontSize=15, textColor=colors.HexColor('#0d47a1'), spaceAfter=4
)))
story.append(Paragraph("Anaesthesia MD Examination", subtitle_style))
story.append(HRFlowable(width="100%", thickness=2, color=colors.HexColor('#1a237e'), spaceAfter=8))
story.append(Spacer(1, 0.3*cm))
# ── CASE VIGNETTE ──────────────────────────────────────────────────────────
story.append(Paragraph("CASE VIGNETTE", h1_style))
story.append(Spacer(1, 0.15*cm))
vignette_data = [
[Paragraph("<b>Patient</b>", table_cell_style), Paragraph("45-year-old male", table_cell_style)],
[Paragraph("<b>Presenting Complaint</b>", table_cell_style), Paragraph("Progressively enlarging right parotid swelling for 2 years, now causing restricted mouth opening and neck stiffness", table_cell_style)],
[Paragraph("<b>Referred for</b>", table_cell_style), Paragraph("Superficial parotidectomy under general anaesthesia", table_cell_style)],
]
vt = Table(vignette_data, colWidths=[4.5*cm, 12*cm])
vt.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,-1), colors.HexColor('#E8EAF6')),
('BACKGROUND', (1,0), (1,-1), colors.HexColor('#FAFAFA')),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#9FA8DA')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
]))
story.append(vt)
# ── SECTION 1: HISTORY ──────────────────────────────────────────────────────
story.append(Paragraph("1. HISTORY", h1_style))
story.append(Paragraph("Chief Complaint", h2_style))
story.append(Paragraph(
"Slow-growing, painless mass in the right pre-auricular/parotid region for 18-24 months. "
"Recent complaint of trismus (mouth opening limited to ~2 cm).",
body_style
))
story.append(Paragraph("History of Present Illness", h2_style))
bullets_hpi = [
"Mass is firm, non-tender, fixed in later stage / mobile in early stage",
"No fever, no pus, no skin erythema (features against acute parotitis)",
"Dysphagia or dysphonia: absent / present (note if present — indicates deep lobe or parapharyngeal extension)",
"No facial nerve weakness (malignancy less likely, but must rule out)",
"No recent weight loss, no cervical lymphadenopathy",
]
for b in bullets_hpi:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("Past History", h2_style))
bullets_past = [
"No prior head/neck surgery or radiotherapy (important: radiation makes mask ventilation difficult)",
"No diabetes, hypertension, immunosuppression",
]
for b in bullets_past:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("Airway-Relevant History", h2_style))
bullets_airway = [
"Snoring / OSA symptoms",
"Previous anaesthesia and intubation difficulty",
"Neck mobility, dental status",
]
for b in bullets_airway:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
# ── SECTION 2: PHYSICAL EXAMINATION ─────────────────────────────────────────
story.append(Paragraph("2. PHYSICAL EXAMINATION", h1_style))
story.append(Paragraph("General", h2_style))
story.append(Paragraph(
"Vitals stable; SpO\u2082 on room air: 98%. Anxious but cooperative.",
body_style
))
story.append(Paragraph("Airway Assessment (MUST document all of the following)", h2_style))
airway_data = [
[Paragraph("<b>Parameter</b>", table_header_style), Paragraph("<b>Finding in This Patient</b>", table_header_style)],
[Paragraph("Mouth opening", table_cell_style), Paragraph("< 2.5 cm (trismus) — GRADE III DIFFICULT", table_cell_style)],
[Paragraph("Mallampati class", table_cell_style), Paragraph("III–IV", table_cell_style)],
[Paragraph("Thyromental distance", table_cell_style), Paragraph("< 6 cm (concern)", table_cell_style)],
[Paragraph("Sternomental distance", table_cell_style), Paragraph("< 12.5 cm", table_cell_style)],
[Paragraph("Neck extension", table_cell_style), Paragraph("Limited if large mass", table_cell_style)],
[Paragraph("Upper lip bite test", table_cell_style), Paragraph("Class II–III", table_cell_style)],
[Paragraph("Neck circumference", table_cell_style), Paragraph("Note any obesity", table_cell_style)],
[Paragraph("Buck teeth / macroglossia", table_cell_style), Paragraph("Note", table_cell_style)],
]
at = Table(airway_data, colWidths=[5*cm, 11.5*cm])
at.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor('#1a237e')),
('ROWBACKGROUNDS', (0,1), (-1,-1), [colors.HexColor('#F5F5F5'), colors.white]),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#9FA8DA')),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
]))
story.append(at)
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph(
'"Other clues to a potentially difficult laryngoscopy include limited neck extension (<35°), a distance between '
'the tip of the patient\'s mandible and hyoid bone of less than 7 cm, a sternomental distance of less than 12.5 cm '
'with the head fully extended and the mouth closed, and a poorly visualized uvula during voluntary tongue protrusion." '
'— Morgan & Mikhail\'s Clinical Anesthesiology, 7e',
quote_style
))
story.append(Paragraph("Local Examination — Parotid", h2_style))
bullets_local = [
"Right pre-auricular swelling, ~5 x 4 cm, firm, non-tender, non-pulsatile",
"Overlying skin normal, no tethering",
"Facial nerve: all branches intact (House-Brackmann Grade I)",
"No Stensen's duct discharge",
"No cervical nodes",
]
for b in bullets_local:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("ENT Examination", h2_style))
story.append(Paragraph(
"\u2022 Oropharyngeal bulk / tonsillar displacement if deep lobe extension",
bullet_style
))
# ── SECTION 3: INVESTIGATIONS ────────────────────────────────────────────────
story.append(Paragraph("3. INVESTIGATIONS", h1_style))
story.append(Paragraph("Imaging (Critical for Anaesthesia Planning)", h2_style))
story.append(Paragraph("CT Neck (with contrast) / MRI:", h3_style))
bullets_imaging = [
"Delineates extent of mass: superficial vs. deep lobe vs. parapharyngeal extension",
"Airway displacement: \"The physical examination should look for tumor displacement of the airway, as well as impaired "
"temporomandibular joint (TMJ) mobility and other predictors of airway difficulties. Available head and neck CT scans "
"or MRI studies should be reviewed with the surgical team, with a focus on airway issues.\" — Miller's Anesthesia, 10e",
"Assess parapharyngeal space involvement",
]
for b in bullets_imaging:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("USG Parotid + FNAC:", h3_style))
bullets_fnac = [
"Pleomorphic adenoma: most common benign parotid neoplasm (85% in parotid, 90% in tail of superficial lobe) — slow-growing, painless, firm",
"Cytology: epithelial + mesenchymal elements",
]
for b in bullets_fnac:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("Routine Labs", h2_style))
story.append(Paragraph(
"\u2022 CBC, RFT, LFT, coagulation, blood grouping; ECG, CXR (PA view); Thyroid function if suspicion",
bullet_style
))
# ── SECTION 4: PREOPERATIVE ANAESTHESIA ASSESSMENT ───────────────────────────
story.append(Paragraph("4. PREOPERATIVE ANAESTHESIA ASSESSMENT", h1_style))
story.append(Paragraph("ASA Physical Status", h2_style))
story.append(Paragraph(
"ASA II (healthy adult, no comorbidities) or ASA III if OSA/HTN present.",
body_style
))
story.append(Paragraph("Difficult Airway Predictors — LEMON Mnemonic", h2_style))
lemon_data = [
[Paragraph("<b>Letter</b>", table_header_style), Paragraph("<b>Parameter</b>", table_header_style), Paragraph("<b>Finding</b>", table_header_style)],
[Paragraph("L", table_cell_style), Paragraph("Look externally", table_cell_style), Paragraph("Parotid mass, neck swelling, limited mouth opening", table_cell_style)],
[Paragraph("E", table_cell_style), Paragraph("Evaluate 3-3-2 rule", table_cell_style), Paragraph("Mouth opening <3 fingers, hyoid-chin <3 fingers, thyroid-mouth floor <2 fingers", table_cell_style)],
[Paragraph("M", table_cell_style), Paragraph("Mallampati", table_cell_style), Paragraph("Class III–IV", table_cell_style)],
[Paragraph("O", table_cell_style), Paragraph("Obstruction", table_cell_style), Paragraph("No frank obstruction but trismus limits access", table_cell_style)],
[Paragraph("N", table_cell_style), Paragraph("Neck mobility", table_cell_style), Paragraph("Possibly restricted by mass", table_cell_style)],
]
lt = Table(lemon_data, colWidths=[1.5*cm, 4.5*cm, 10.5*cm])
lt.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor('#1a237e')),
('ROWBACKGROUNDS', (0,1), (-1,-1), [colors.HexColor('#FFF8E1'), colors.white]),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#9FA8DA')),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
('ALIGN', (0,0), (0,-1), 'CENTER'),
('FONTNAME', (0,1), (0,-1), 'Helvetica-Bold'),
('TEXTCOLOR', (0,1), (0,-1), colors.HexColor('#1a237e')),
]))
story.append(lt)
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph(
"CONCLUSION: This is an ANTICIPATED DIFFICULT AIRWAY — the critical distinction that drives all anaesthetic planning.",
highlight_style
))
# ── SECTION 5: ANAESTHETIC PLAN ─────────────────────────────────────────────
story.append(Paragraph("5. ANAESTHETIC PLAN", h1_style))
story.append(Paragraph("Pre-operative Preparation", h2_style))
preop_bullets = [
"Informed consent including risk of awake intubation, tracheostomy, facial nerve injury",
"Multidisciplinary team: Anaesthesiologist + ENT Surgeon (scrubbed and ready for surgical airway)",
"Equipment checklist:",
" - Flexible fiberoptic bronchoscope (primary tool)",
" - Video laryngoscope (McGrath / GlideScope / C-MAC)",
" - Bougie, multiple ETT sizes (6.0, 6.5, 7.0)",
" - Supraglottic airway devices: LMA ProSeal / i-gel (backup)",
" - Emergency surgical airway kit (cricothyrotomy/tracheostomy set) — opened and ready",
" - Anterior commissure (Hollinger) laryngoscope",
"Neck prepped and draped before induction",
"IV access: Two large-bore IVs",
"Monitors: SpO\u2082, ETCO\u2082, ECG, NIBP, temperature, nerve stimulator (facial nerve monitoring — therefore muscle relaxants avoided after intubation)",
]
for i, b in enumerate(preop_bullets):
if b.startswith(" -"):
story.append(Paragraph(f" {b.strip()}", sub_bullet_style))
else:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("Pre-medication", h2_style))
premed_bullets = [
"Tab. Diazepam 5 mg oral night before (anxiolysis — use carefully if airway concern)",
"Inj. Glycopyrrolate 0.2 mg IM 30 min prior: dries secretions, antisialagogue, does NOT cross blood-brain barrier",
"Avoid: Heavy parenteral sedation — risk of losing airway",
]
for b in premed_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph(
'"Glycopyrrolate would be a good choice of premedication because it minimizes upper airway secretions without crossing '
'the blood-brain barrier. Parenteral sedatives should be very carefully titrated. Dexmedetomidine and ketamine could '
'be used as sedatives and preserve respiratory effort." — Morgan & Mikhail\'s Clinical Anesthesiology, 7e',
quote_style
))
story.append(Paragraph("Airway Strategy: AWAKE FIBEROPTIC INTUBATION (AFOI)", h2_style))
story.append(Paragraph(
"This is the gold standard for anticipated difficult airway with trismus.",
highlight_style
))
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph(
'"Induction of anesthesia should be delayed until after the airway has been secured. Useful alternatives include '
'awake fiberoptic intubation, awake video laryngoscopy, or awake use of optical stylets." '
'— Morgan & Mikhail\'s Clinical Anesthesiology, 7e',
quote_style
))
story.append(Paragraph("Step 1 — Topical Airway Anaesthesia", h3_style))
step1_bullets = [
"Nebulised 4% lignocaine (4 mL) for oropharynx and upper airway",
"Gargle with 4% lignocaine",
"10% lignocaine spray to posterior pharynx",
"Bilateral glossopharyngeal nerve blocks: 2 mL of 2% lignocaine injected into base of palatoglossal arch (anterior tonsillar pillar) with 25G spinal needle — blocks posterior 1/3 tongue and oropharynx sensation",
"Superior laryngeal nerve (SLN) block (bilateral): 3 mL of 2% lignocaine injected 1 cm below greater cornu of hyoid bone, through thyrohyoid membrane — anaesthetises infraglottic larynx",
"Transtracheal block: 3 mL of 2% lignocaine injected through cricothyroid membrane; patient asked to inhale-cough to spray subglottically",
"TOTAL LIGNOCAINE DOSE MUST NOT EXCEED 3 mg/kg (toxicity risk)",
]
for b in step1_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph(
'"Bilateral superior laryngeal nerve blocks and a trans tracheal block would anesthetize the airway below the epiglottis. '
'The hyoid bone is located, and 3 mL of 2% lidocaine is infiltrated 1 cm below each greater cornu, where the internal '
'branch of the superior laryngeal nerves penetrates the thyrohyoid membrane." — Morgan & Mikhail\'s Clinical Anesthesiology, 7e',
quote_style
))
story.append(Paragraph("Step 2 — Conscious Sedation (with airway preservation)", h3_style))
step2_bullets = [
"Inj. Dexmedetomidine: 1 mcg/kg IV over 10 min (loading), then 0.3–0.7 mcg/kg/hr infusion — provides sedation, analgesia, anxiolysis; preserves respiratory effort and airway tone",
"Alternatively: Ketamine 0.5 mg/kg IV (preserves airway reflexes and spontaneous ventilation)",
"Supplemental O\u2082 via nasal cannula (THRIVE — Transnasal Humidified Rapid Insufflation Ventilatory Exchange, if available) — prolongs safe apnoea time",
]
for b in step2_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("Step 3 — AFOI Execution (Nasal route preferred when mouth opening is very limited)", h3_style))
step3_bullets = [
"Lubricate and vasoconstrict nostril: Xylometazoline drops + 4% lignocaine to nasal mucosa",
"Pass warmed, lubricated 6.0 or 6.5 mm cuffed ETT over bronchoscope",
"Advance fiberoptic scope through nostril → nasopharynx → visualise epiglottis → pass through glottis → confirm tracheal rings and carina",
"Railroad ETT over the bronchoscope into trachea",
"Confirm position with ETCO\u2082 waveform + bilateral breath sounds",
"Secure tube, inflate cuff",
]
for b in step3_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("Step 4 — Induction after Secure Airway", h3_style))
step4_bullets = [
"Once intubation confirmed:",
"Inj. Propofol 1–2 mg/kg IV (titrated) OR Inj. Thiopentone 3–5 mg/kg",
"Single intubating dose: Inj. Succinylcholine 1.5 mg/kg OR Inj. Rocuronium 0.6 mg/kg — for induction ONLY",
"NO FURTHER MUSCLE RELAXANTS intraoperatively (facial nerve monitoring requirement)",
]
for b in step4_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("Intraoperative Maintenance", h2_style))
maint_bullets = [
"TIVA (Total IV Anaesthesia): Propofol infusion 50–150 mcg/kg/min + Remifentanil 0.1 mcg/kg/min",
"OR: Sevoflurane 1–2% in O\u2082/air + Remifentanil infusion",
"Avoid neuromuscular blockers after intubation — surgeon must use facial nerve stimulator",
"Patient position: head-up 15–20° (reduces venous ooze), head turned to LEFT (operative side up — right parotid surgery)",
"Throat pack inserted (document and remove at end of surgery)",
"Eyes protected with padding/tape",
]
for b in maint_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph(
'"For this reason, the surgical team usually requests that muscle relaxants be avoided after endotracheal intubation '
'has been achieved... A single, small dose of rocuronium to facilitate endotracheal intubation is often employed, '
'followed by sevoflurane anesthesia in conjunction with a remifentanil infusion (e.g., 0.1 mcg/kg/min) to provide '
'immobility." — Miller\'s Anesthesia, 10e',
quote_style
))
story.append(Paragraph("Monitoring", h2_style))
monitor_bullets = [
"Standard ASA monitors + ETCO\u2082",
"Neuromuscular monitoring (Train-of-Four) to confirm reversal",
"Facial nerve integrity monitoring by surgeon (requires zero paralysis)",
"Temperature, urine output",
]
for b in monitor_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
# ── SECTION 6: ASA DIFFICULT AIRWAY ALGORITHM ────────────────────────────────
story.append(Paragraph("6. ASA DIFFICULT AIRWAY ALGORITHM", h1_style))
story.append(Paragraph("Key Decision Points for This Patient:", h2_style))
algo_bullets = [
"Anticipated difficult airway → AWAKE INTUBATION pathway (left arm of algorithm)",
"Assess likelihood of: difficult mask ventilation, difficult SGA, difficult laryngoscopy, difficult intubation, difficult surgical airway",
"Consider: awake intubation vs. intubation after GA induction; non-invasive vs. invasive; preserve vs. ablate spontaneous ventilation",
"If awake intubation fails → Cancel case / Invasive airway access (surgical tracheostomy)",
"Surgical team on standby for emergency surgical airway at all times",
]
for b in algo_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph(
"Algorithm Summary (ASA Task Force on Management of the Difficult Airway — Anesthesiology 2003;98:1269–1277 as "
"reproduced in Morgan & Mikhail's Clinical Anesthesiology, 7e):",
body_style
))
story.append(Spacer(1, 0.2*cm))
algo_table_data = [
[Paragraph("<b>AWAKE INTUBATION PATHWAY</b>", table_header_style), Paragraph("<b>INTUBATION AFTER GA INDUCTION</b>", table_header_style)],
[
Paragraph(
"1. Airway approached by noninvasive intubation\n"
" - SUCCEED* → proceed\n"
" - FAIL → Cancel / Other options / Invasive access\n\n"
"2. Invasive airway access*",
table_cell_style
),
Paragraph(
"If initial intubation SUCCESSFUL* → proceed\n\n"
"If UNSUCCESSFUL → Consider:\n"
" 1. Call for help\n"
" 2. Return to spontaneous ventilation\n"
" 3. Awaken patient\n\n"
" Then: Face mask ventilation adequate?\n"
" YES → Nonemergency pathway\n"
" → Alternative intubation approaches\n"
" → FAIL after multiple attempts: Invasive access / other options / awaken\n"
" NO → Consider/Attempt SGA\n"
" → SGA ADEQUATE* → Nonemergency\n"
" → SGA NOT ADEQUATE → EMERGENCY PATHWAY\n"
" → Call for help → Emergency noninvasive ventilation\n"
" → FAIL → Emergency invasive airway access*",
table_cell_style
)
]
]
algo_tbl = Table(algo_table_data, colWidths=[8.25*cm, 8.25*cm])
algo_tbl.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor('#1a237e')),
('BACKGROUND', (0,1), (0,1), colors.HexColor('#E8F5E9')),
('BACKGROUND', (1,1), (1,1), colors.HexColor('#FFF3E0')),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#9FA8DA')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
]))
story.append(algo_tbl)
story.append(Paragraph(
"* Confirm ventilation, tracheal intubation, or SGA placement with exhaled CO\u2082. "
"Invasive airway access includes surgical or percutaneous airway, jet ventilation, and retrograde intubation.",
ParagraphStyle('AlgoNote', parent=body_style, fontSize=8, textColor=colors.HexColor('#555555'), spaceBefore=3)
))
# ── SECTION 7: CICO PROTOCOL ─────────────────────────────────────────────────
story.append(Paragraph("7. CANNOT INTUBATE - CANNOT OXYGENATE (CICO) PROTOCOL", h1_style))
story.append(Paragraph(
"If ALL intubation attempts fail and SpO\u2082 is falling:",
body_style
))
cico_steps = [
"Call for help IMMEDIATELY",
"Attempt LMA / i-gel insertion as rescue oxygenation (Supraglottic Airway Device)",
"If SGA fails → Emergency Front-of-Neck Access (FONA):",
" - Cricothyrotomy (needle/surgical) — fastest route",
" - Emergency Tracheostomy by ENT surgeon (preferred if already scrubbed and ready)",
]
for s in cico_steps:
if s.startswith(" -"):
story.append(Paragraph(f" {s.strip()}", sub_bullet_style))
else:
story.append(Paragraph(f"\u2022 {s}", bullet_style))
story.append(Paragraph(
'"Once a \'cannot intubate, cannot ventilate\' situation has been identified, immediate consideration should be '
'given to providing surgical airway access." — Cummings Otolaryngology Head and Neck Surgery',
quote_style
))
# ── SECTION 8: POSTOPERATIVE MANAGEMENT ──────────────────────────────────────
story.append(Paragraph("8. POSTOPERATIVE MANAGEMENT", h1_style))
story.append(Paragraph("Extubation Strategy (equally important — 'Difficult Extubation')", h2_style))
extub_bullets = [
"Extubate ONLY when patient is fully awake, following commands, with adequate neuromuscular reversal (TOF ratio > 0.9)",
"Consider: Airway Exchange Catheter (AEC) left in situ before extubation — allows reintubation if needed",
"Patient positioned head-up 30–45°",
"Inj. Dexamethasone 8 mg IV given intraoperatively — reduces postoperative oedema",
"Post-extubation monitoring in High Dependency Unit (HDU) for minimum 4 hours",
]
for b in extub_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("Analgesia — Multimodal", h2_style))
analg_bullets = [
"Inj. Paracetamol 1 g IV 8 hourly",
"Inj. Ketorolac 30 mg IV (avoid if risk of bleeding)",
"Inj. Morphine 0.1 mg/kg IV PRN (with antiemetic cover)",
"Wound infiltration by surgeon with 0.25% Bupivacaine",
]
for b in analg_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("PONV Prophylaxis", h2_style))
ponv_bullets = [
"Inj. Ondansetron 4 mg IV at end of surgery",
"Inj. Dexamethasone 8 mg IV (also reduces oedema — dual benefit)",
"Head-up position; avoid opioid excess",
]
for b in ponv_bullets:
story.append(Paragraph(f"\u2022 {b}", bullet_style))
story.append(Paragraph("Complications to Watch For", h2_style))
comp_data = [
[Paragraph("<b>Complication</b>", table_header_style), Paragraph("<b>Notes</b>", table_header_style)],
[Paragraph("Haematoma", table_cell_style), Paragraph("Can cause RAPID airway compromise — emergency reintubation / surgical evacuation required", table_cell_style)],
[Paragraph("Facial nerve palsy", table_cell_style), Paragraph("Temporary (neurapraxia) or permanent (neurotmesis) — House-Brackmann grading", table_cell_style)],
[Paragraph("Frey's syndrome", table_cell_style), Paragraph("Late complication — auriculotemporal nerve — gustatory sweating over parotid area", table_cell_style)],
[Paragraph("Sialocele / salivary fistula", table_cell_style), Paragraph("Late complication — collection of saliva under skin flap", table_cell_style)],
[Paragraph("Anaesthesia mumps", table_cell_style), Paragraph("Rare — acute postoperative parotid swelling (Stensen's duct obstruction / pneumoparotitis) — can compromise airway in severe cases. Self-limiting.", table_cell_style)],
[Paragraph("Wound infection", table_cell_style), Paragraph("Prophylactic antibiotics, wound care", table_cell_style)],
]
comp_tbl = Table(comp_data, colWidths=[4*cm, 12.5*cm])
comp_tbl.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor('#1a237e')),
('ROWBACKGROUNDS', (0,1), (-1,-1), [colors.HexColor('#FFEBEE'), colors.white]),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#9FA8DA')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
]))
story.append(comp_tbl)
# ── SECTION 9: VIVA DISCUSSION ────────────────────────────────────────────────
story.append(Paragraph("9. DISCUSSION POINTS FOR MD EXAM VIVA", h1_style))
qna = [
(
"Q: Why is awake intubation preferred here?",
"Because trismus from the parotid mass makes any attempt at direct or video laryngoscopy after GA induction dangerous. "
"Induction abolishes airway tone and may cause complete obstruction. Awake technique preserves spontaneous ventilation "
"and muscle tone, maintaining the airway at all times."
),
(
"Q: Why no muscle relaxants intraoperatively?",
"Facial nerve identification and preservation is central to parotid surgery. Surgeons use a nerve stimulator. If the "
"patient is paralyzed, stimulation will not produce visible muscle twitch and the nerve cannot be identified, risking permanent facial palsy. "
"As stated in Miller's Anesthesia 10e: 'preservation of the facial nerve is of prime importance in these operations; consequently, "
"the surgeon often must identify the facial nerve by using a nerve stimulator. This crucial step is not possible if "
"neuromuscular blockade is present.'"
),
(
"Q: What if awake fiberoptic intubation fails?",
"Per ASA algorithm: cancel case, reassess, consider video laryngoscopy with topical anaesthesia, retrograde intubation, "
"or elective tracheostomy under local anaesthesia before proceeding. Never attempt the same failed technique repeatedly."
),
(
"Q: Role of dexmedetomidine in difficult airway management?",
"Dexmedetomidine is a highly selective alpha-2 adrenoceptor agonist. It provides dose-dependent sedation, analgesia, "
"and anxiolysis while PRESERVING respiratory drive and airway reflexes. This makes it the sedative of choice for awake "
"intubation. Patient is calm and cooperative but maintains airway patency and spontaneous ventilation. Loading dose: "
"1 mcg/kg over 10 minutes; maintenance: 0.3–0.7 mcg/kg/hr."
),
(
"Q: Common causes of parotid swelling — surgical classification?",
"Benign neoplasms: Pleomorphic adenoma (most common — 80%, 85% in parotid, 90% in tail of superficial lobe; slow-growing, "
"painless, firm; may undergo malignant transformation), Warthin's tumour (bilateral in 10%, smokers, males, Tc-99m scan hot). "
"Malignant: Mucoepidermoid carcinoma (most common malignant), Adenoid cystic carcinoma (perineural invasion, skip lesions), "
"Acinic cell carcinoma. Inflammatory: Acute bacterial parotitis (dehydration, elderly, Staph. aureus), Mumps (epidemic parotitis, "
"EBV recurrence), Sjogren's syndrome, Sarcoidosis. Other: HIV parotitis, Lymphoma."
),
(
"Q: What is 'anaesthesia mumps'?",
"Rare complication of general anaesthesia: acute bilateral or unilateral parotid swelling occurring intraoperatively or "
"within 24 hours postoperatively. Caused by: (a) Stensen's duct obstruction due to head position or direct compression, "
"(b) Retrograde entry of air into duct (pneumoparotitis — increased oral cavity pressure during airway manipulation). "
"Clinical: tender pre-auricular swelling, mild erythema, no pus. CT may show parapharyngeal involvement. Management: "
"conservative (hydration, NSAIDs, warm compresses). Can rarely cause airway compromise via parapharyngeal extension — "
"monitor closely and maintain high index of suspicion."
),
(
"Q: Sternomental vs. Thyromental distance in airway assessment?",
"Thyromental distance (Patil's test): distance from thyroid notch to tip of mandible with neck fully extended. "
"Normal >6.5 cm; <6 cm = difficult intubation predicted. "
"Sternomental distance: distance from sternum to tip of mandible with neck fully extended and mouth closed. "
"Normal >12.5 cm; <12.5 cm suggests difficult laryngoscopy (Morgan & Mikhail, 7e)."
),
(
"Q: What is the Hollinger (anterior commissure) laryngoscope?",
"Per Cummings Otolaryngology: 'The anterior commissure laryngoscope is arguably the otolaryngologist's most useful tool "
"in the management of a difficult airway.' It is a straight-bladed laryngoscope that gives an excellent anterior glottic view. "
"It accommodates only small ETT (5.5 mm or less). If a larger ETT is required, an intubation bougie is first inserted through "
"the laryngoscope, which is then removed, and the ETT is railroaded over the bougie."
),
]
for q, a in qna:
story.append(Paragraph(q, h3_style))
story.append(Paragraph(a, body_style))
story.append(Spacer(1, 0.1*cm))
# ── SECTION 10: SUMMARY TABLE ─────────────────────────────────────────────────
story.append(Paragraph("10. QUICK SUMMARY TABLE", h1_style))
summary_data = [
[Paragraph("<b>Phase</b>", table_header_style), Paragraph("<b>Key Actions</b>", table_header_style)],
[Paragraph("Pre-operative", table_cell_style), Paragraph(
"CT/MRI airway review with surgeon; AFOI decision; Glycopyrrolate premedication; "
"Dexmedetomidine sedation; equipment checklist; neck prepped; ENT surgeon scrubbed",
table_cell_style)],
[Paragraph("Induction", table_cell_style), Paragraph(
"Awake fiberoptic nasal intubation; topical lignocaine + SLN block + transtracheal block; "
"nasotracheal 6.0–6.5 mm ETT; confirm ETCO\u2082; then Propofol/Thiopentone induction",
table_cell_style)],
[Paragraph("Maintenance", table_cell_style), Paragraph(
"TIVA (Propofol + Remifentanil) or Sevoflurane + Remifentanil; "
"NO neuromuscular blockers after induction; head-up 15–20°; facial nerve monitoring",
table_cell_style)],
[Paragraph("Emergence", table_cell_style), Paragraph(
"Fully awake extubation only; TOF >0.9; airway exchange catheter in situ; "
"head-up 30–45°; HDU monitoring minimum 4 hours",
table_cell_style)],
[Paragraph("CICO Rescue", table_cell_style), Paragraph(
"SGA (LMA/i-gel) → if fails → Emergency Front-of-Neck Access: "
"Needle/surgical cricothyrotomy or emergency tracheostomy",
table_cell_style)],
[Paragraph("Postoperative Watch", table_cell_style), Paragraph(
"Haematoma (urgent airway risk), facial nerve palsy, Frey's syndrome (late), "
"sialocele, PONV, pain, anaesthesia mumps",
table_cell_style)],
]
sum_tbl = Table(summary_data, colWidths=[3.5*cm, 13*cm])
sum_tbl.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor('#1a237e')),
('ROWBACKGROUNDS', (0,1), (-1,-1), [colors.HexColor('#E8EAF6'), colors.white]),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#9FA8DA')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
]))
story.append(sum_tbl)
# ── REFERENCES ────────────────────────────────────────────────────────────────
story.append(Paragraph("KEY TEXTBOOK REFERENCES", h1_style))
refs = [
"Morgan & Mikhail's Clinical Anesthesiology, 7th Edition — Chapter 19: Airway Management; Difficult Airway Algorithm; Awake Intubation; Nerve Blocks",
"Miller's Anesthesia, 2-Volume Set, 10th Edition — Chapter: Otolaryngology / Head & Neck Surgery; Parotid and Salivary Gland Surgery (p. 9818)",
"Cummings Otolaryngology Head and Neck Surgery — Chapter 6: Difficult Airway / Intubation; Surgical Airway Access",
"Barash, Cullen, and Stoelting's Clinical Anesthesia, 9th Edition — The Difficult Airway",
"ASA Task Force on Management of the Difficult Airway. Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2003 May;98(5):1269–1277",
"Robbins & Kumar Basic Pathology — Diseases of Salivary Glands; Pleomorphic Adenoma",
"K.J. Lee's Essential Otolaryngology — Salivary Glands: Tumours and Classification",
"Frontiers in Surgery 2022 — Anesthesia Mumps with Airway Obstruction after Radical Nephrectomy: A Case Report and Literature Review",
]
for i, r in enumerate(refs, 1):
story.append(Paragraph(f"{i}. {r}", ParagraphStyle(
'Ref', parent=body_style, fontSize=8.5, spaceAfter=3, textColor=colors.HexColor('#333333')
)))
# ── FOOTER NOTE ───────────────────────────────────────────────────────────────
story.append(Spacer(1, 0.4*cm))
story.append(HRFlowable(width="100%", thickness=1, color=colors.HexColor('#9FA8DA'), spaceAfter=6))
story.append(Paragraph(
"Prepared for Anaesthesia MD Examination | All content sourced from standard anaesthesia and surgical textbooks | "
"Clinical judgement must always take precedence over any single algorithm or protocol | July 2026",
ParagraphStyle('Footer', parent=body_style, fontSize=7.5, textColor=colors.HexColor('#777777'), alignment=TA_CENTER)
))
# ── BUILD ─────────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF generated: {OUTPUT}")
cd /home/daytona/workspace/parotid-airway-case && python generate_pdf.py 2>&1
ls -lh /home/daytona/workspace/parotid-airway-case/
Parotid Swelling Difficult Airway Case Presentation
PDF Document · PDF
- Case Vignette - formatted summary table
- History - chief complaint, HPI, past history, airway-relevant history
- Physical Examination - full airway assessment table, local parotid exam, ENT
- Investigations - CT/MRI imaging notes, FNAC, routine labs
- Preoperative Anaesthesia Assessment - ASA status, LEMON mnemonic table, difficult airway conclusion box
- Anaesthetic Plan - pre-op prep checklist, premedication, full AFOI step-by-step (Steps 1-4), intraoperative maintenance, monitoring
- ASA Difficult Airway Algorithm - full dual-column pathway table with footnotes
- CICO Protocol - with textbook citation
- Viva Discussion Q&A - 8 questions with detailed answers (awake intubation rationale, no muscle relaxants, dex fail, dexmedetomidine, parotid pathology, anaesthesia mumps, distance measures, Hollinger laryngoscope)
- Quick Summary Table + References (8 sources cited)
Hyperkalemia and ecg chnages 7 mark que
Hyperkalemia and ECG Changes — 7 Mark Answer
Definition
| Grade | Serum K+ | ECG |
|---|---|---|
| Mild | 5.0–6.0 mEq/L | Without ECG changes |
| Moderate | 5–6 mEq/L with ECG changes, or 6.1–6.5 mEq/L without ECG changes | |
| Severe | 6.1–6.5 mEq/L with ECG changes, or > 6.5 mEq/L |
ECG Changes in Hyperkalemia — Sequential / Progressive
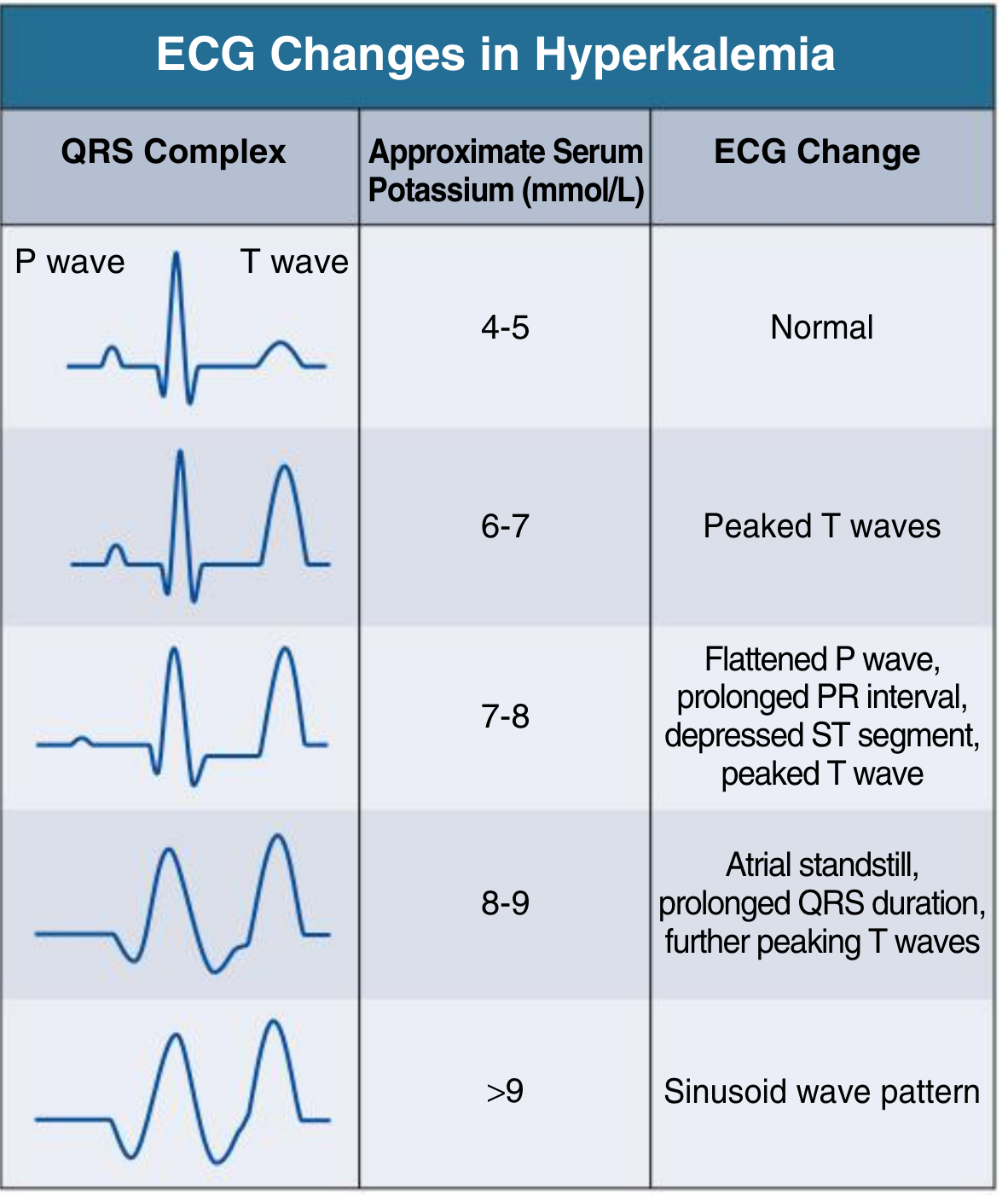
Sequential ECG Changes with K+ Levels
| Serum K+ (mmol/L) | ECG Change | Mechanism |
|---|---|---|
| 4–5 (Normal) | Normal ECG | Normal resting membrane potential |
| 5.5–6.5 | Peaked (tented) T waves — tall, narrow, symmetric; best seen in precordial leads | Accelerated repolarisation; reduced resting membrane potential |
| 6.5–7.5 | Prolonged PR interval (1st degree AV block); Flattened / absent P waves (atrial standstill); ST segment depression | Slowed atrial conduction and depolarisation |
| 7.5–8.5 | Widened QRS complex (> 120 ms); further T-wave peaking | Slowed ventricular intraventricular conduction |
| > 8.5–9 | Sine wave pattern (QRS and T wave merge) — sign of impending cardiac arrest | Extreme slowing of all conduction; fusion of QRS-T |
| > 9–10 | Ventricular fibrillation / Asystole / Diastolic arrest | Complete conduction failure |
"Progressive hyperkalemia results in identifiable changes in the electrocardiogram. These include peaking of the T wave, flattening of the P wave, prolongation of the PR interval, depression of the ST segment, prolongation of the QRS complex, and, eventually, progression to a sine wave pattern. Ventricular fibrillation may occur at any time during this ECG progression." — Comprehensive Clinical Nephrology, 7e (Fig. 10.6)
"The 'sine wave' is a sign of impending cardiac arrest and is often a fatal rhythm." — Miller's Anesthesia, 10e
Pathophysiology of ECG Changes
- Normal RMP = -90 mV (maintained by high K+ gradient across cell membrane)
- High extracellular K+ → RMP becomes less negative (closer to threshold) → partial depolarisation
- Partial depolarisation → inactivation of fast Na+ channels → slowed conduction velocity → widened QRS, AV block
- Repolarisation is accelerated early → tall peaked T waves (increased slope of phase 3)
- As K+ rises further → depolarisation blockade → arrest
Key ECG Features — Point-wise (for exam)
- Peaked (tented) T waves — earliest change; tall, narrow, symmetric, with narrow base; present in all leads
- Prolonged PR interval — first-degree AV block; may progress to complete heart block
- Flattened / absent P waves — atrial standstill (sino-ventricular conduction may persist)
- ST segment depression
- Widened QRS complex — > 120 ms; bizarre morphology; may mimic bundle branch block
- Sine wave pattern — QRS widens and merges with T wave — pre-arrest pattern
- Ventricular fibrillation / asystole — terminal event; "death from hyperkalemia is usually the result of diastolic arrest or ventricular fibrillation" (Tintinalli's Emergency Medicine)
Important: ECG findings correlate generally with the degree of hyperkalemia, but the rate of progression from mild to severe cardiac effects can be unpredictable and may not correlate well with changes in serum K+. — Comprehensive Clinical Nephrology, 7e
ECG in Context: When to Act
- A stat ECG is essential in ALL hyperkalemic patients
- If ECG changes are present → emergency treatment starts immediately (Tintinalli's)
- Even if ECG is normal but K+ ≥ 6.5 mEq/L → aggressive management still required (Harrison's, 22e)
Treatment Summary (Linked to ECG)
| Step | Drug | Mechanism | Onset | Duration |
|---|---|---|---|---|
| 1. Membrane stabilisation (ECG changes present) | Inj. Calcium gluconate 10 mL of 10% IV over 2–3 min | Raises action potential threshold; restores difference between RMP and threshold; does NOT lower K+ | 1–3 min | 30–60 min |
| 2. Redistribution (shift K+ into cells) | Inj. Regular insulin 10 units IV + 50 mL of 50% dextrose (D50W) | Activates Na/K ATPase → K+ into cells | 10–20 min | 4–6 h |
| Nebulised salbutamol (albuterol) 10–20 mg | Beta-2 agonist → K+ into cells (additive with insulin) | 30 min | 2–6 h | |
| Inj. NaHCO₃ (sodium bicarbonate) — isotonic infusion only | Delayed effect (4–6 h); useful in metabolic acidosis | Hours | Variable | |
| 3. Removal (eliminate K+ from body) | Frusemide (loop diuretic) | Urinary excretion | 30 min | — |
| Patiromer / Sodium zirconium cyclosilicate / Resonium (K+-binding resins) | GI binding and excretion | Hours | — | |
| Haemodialysis | Direct removal; for renal failure or refractory cases | Rapid | — |
Digoxin caution: IV calcium should be used with extreme caution in patients on digoxin (hypercalcemia potentiates digoxin toxicity). If necessary, 10 mL of 10% calcium gluconate in 100 mL D5W over 20–30 min to avoid acute hypercalcemia. — Harrison's Principles of Internal Medicine, 22e
Common Causes of Hyperkalemia (for completeness)
- Impaired renal excretion: CKD, AKI, Addison's disease (mineralocorticoid deficiency)
- Drugs: ACE inhibitors, ARBs, potassium-sparing diuretics (spironolactone, amiloride), NSAIDs, beta-blockers, succinylcholine, digoxin, calcineurin inhibitors
- Transcellular shift: Metabolic acidosis, insulin deficiency, rhabdomyolysis, massive trauma, tumour lysis syndrome, haemolysis
- Pseudohyperkalemia: Haemolysed sample (tourniquet ischaemia, thrombocytosis, leukocytosis) — no ECG changes
Create a PDF study guide on hyperkalemia and ECG changes for exam revision
mkdir -p /home/daytona/workspace/hyperkalemia-guide && echo "ready"
~/hyperkalemia-guide/generate_guide.py
import math
import urllib.request
import os
from reportlab.lib.pagesizes import A4
from reportlab.lib.units import cm, mm
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY, TA_RIGHT
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether, Image
)
from reportlab.graphics.shapes import (
Drawing, Rect, String, Line, Polygon, Circle, Path, Group
)
from reportlab.graphics import renderPDF
from reportlab.graphics.charts.lineplots import LinePlot
from reportlab.graphics.widgets.markers import makeMarker
from reportlab.pdfgen import canvas
W, H = A4
OUTPUT = "/home/daytona/workspace/hyperkalemia-guide/Hyperkalemia_ECG_Changes_Study_Guide.pdf"
# ── Download ECG image ─────────────────────────────────────────────────────
ECG_IMG_URL = "https://cdn.orris.care/cdss_images/b676e83606cc2f60f1fb18ad9937e2eec334e88df4df44312d2e4d1e30fe329d.png"
ECG_IMG_PATH = "/home/daytona/workspace/hyperkalemia-guide/ecg_hyperkalemia.png"
if not os.path.exists(ECG_IMG_PATH):
urllib.request.urlretrieve(ECG_IMG_URL, ECG_IMG_PATH)
print("ECG image downloaded.")
# ── Color palette ──────────────────────────────────────────────────────────
C_NAVY = colors.HexColor('#0D2B55')
C_BLUE = colors.HexColor('#1565C0')
C_LBLUE = colors.HexColor('#1E88E5')
C_TEAL = colors.HexColor('#00838F')
C_RED = colors.HexColor('#C62828')
C_AMBER = colors.HexColor('#E65100')
C_GREEN = colors.HexColor('#2E7D32')
C_BGBLUE = colors.HexColor('#E3F2FD')
C_BGRED = colors.HexColor('#FFEBEE')
C_BGAMB = colors.HexColor('#FFF3E0')
C_BGGRN = colors.HexColor('#E8F5E9')
C_BGPURP = colors.HexColor('#F3E5F5')
C_STRIPE = colors.HexColor('#F5F8FF')
C_GOLD = colors.HexColor('#F9A825')
C_PURPLE = colors.HexColor('#6A1B9A')
C_GRAY = colors.HexColor('#546E7A')
C_LGRAY = colors.HexColor('#ECEFF1')
# ── Styles ─────────────────────────────────────────────────────────────────
ss = getSampleStyleSheet()
def S(name, **kw):
base = kw.pop('parent', ss['Normal'])
return ParagraphStyle(name, parent=base, **kw)
TITLE = S('TITLE', fontSize=26, textColor=colors.white, fontName='Helvetica-Bold',
alignment=TA_CENTER, leading=32, spaceAfter=2)
SUBTITLE = S('SUBTITLE', fontSize=13, textColor=colors.HexColor('#BBDEFB'),
fontName='Helvetica', alignment=TA_CENTER, leading=18, spaceAfter=2)
BADGE = S('BADGE', fontSize=9, textColor=colors.white, fontName='Helvetica-Bold',
alignment=TA_CENTER, backColor=C_RED, borderPad=3)
H1 = S('H1', fontSize=13, textColor=colors.white, fontName='Helvetica-Bold',
spaceBefore=12, spaceAfter=4, backColor=C_NAVY,
leftIndent=-12, rightIndent=-12, borderPad=6, leading=18)
H2 = S('H2', fontSize=11, textColor=C_NAVY, fontName='Helvetica-Bold',
spaceBefore=9, spaceAfter=3, leading=15)
H3 = S('H3', fontSize=10, textColor=C_BLUE, fontName='Helvetica-Bold',
spaceBefore=6, spaceAfter=2, leading=13)
BODY = S('BODY', fontSize=9.5, leading=14, spaceAfter=3, alignment=TA_JUSTIFY,
fontName='Helvetica')
BULL = S('BULL', fontSize=9.5, leading=13, spaceAfter=2, leftIndent=12,
fontName='Helvetica')
SBULL = S('SBULL', fontSize=9, leading=12, spaceAfter=1, leftIndent=24,
fontName='Helvetica', textColor=C_GRAY)
QUOTE = S('QUOTE', fontSize=9, leading=13, spaceAfter=4, spaceBefore=4,
leftIndent=14, rightIndent=8, fontName='Helvetica-Oblique',
textColor=C_NAVY, backColor=C_BGBLUE, borderPad=6)
BOX_RED = S('BOX_RED', fontSize=9.5, leading=13, spaceAfter=2, spaceBefore=2,
leftIndent=8, rightIndent=8, fontName='Helvetica-Bold',
textColor=C_RED, backColor=C_BGRED, borderPad=5)
BOX_GRN = S('BOX_GRN', fontSize=9.5, leading=13, spaceAfter=2, spaceBefore=2,
leftIndent=8, rightIndent=8, fontName='Helvetica-Bold',
textColor=C_GREEN, backColor=C_BGGRN, borderPad=5)
BOX_AMB = S('BOX_AMB', fontSize=9.5, leading=13, spaceAfter=2, spaceBefore=2,
leftIndent=8, rightIndent=8, fontName='Helvetica', textColor=C_AMBER,
backColor=C_BGAMB, borderPad=5)
TH = S('TH', fontSize=8.5, fontName='Helvetica-Bold', textColor=colors.white,
alignment=TA_CENTER, leading=11)
TC = S('TC', fontSize=8.5, fontName='Helvetica', textColor=colors.black,
alignment=TA_LEFT, leading=11)
TC_C = S('TC_C', fontSize=8.5, fontName='Helvetica', textColor=colors.black,
alignment=TA_CENTER, leading=11)
TC_B = S('TC_B', fontSize=8.5, fontName='Helvetica-Bold', textColor=C_NAVY,
alignment=TA_LEFT, leading=11)
FOOT = S('FOOT', fontSize=7.5, textColor=C_GRAY, alignment=TA_CENTER, leading=10)
REF = S('REF', fontSize=8, leading=11, spaceAfter=2, textColor=C_GRAY,
fontName='Helvetica')
def tbl_style(hdr_color=C_NAVY, row_colors=(C_STRIPE, colors.white)):
return TableStyle([
('BACKGROUND', (0,0), (-1,0), hdr_color),
('ROWBACKGROUNDS', (0,1), (-1,-1), row_colors),
('GRID', (0,0), (-1,-1), 0.4, colors.HexColor('#B0BEC5')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
])
def p(text, style=BODY): return Paragraph(text, style)
def sp(h=0.2): return Spacer(1, h*cm)
def hr(): return HRFlowable(width='100%', thickness=1, color=colors.HexColor('#B0BEC5'), spaceAfter=4)
def bull(text): return p(f'\u2022 {text}', BULL)
def sbull(text): return p(f'\u25E6 {text}', SBULL)
# ── ECG waveform drawing ───────────────────────────────────────────────────
def make_ecg_drawing(label, k_level, color, width=130, height=55,
peaked_t=False, flat_p=False, wide_qrs=False,
sine=False, vf=False, pr_long=False):
"""Draw a stylised ECG trace for a given K+ level."""
d = Drawing(width, height)
# background
d.add(Rect(0, 0, width, height, fillColor=colors.HexColor('#F8FAFE'),
strokeColor=colors.HexColor('#CFD8DC'), strokeWidth=0.5))
# grid lines
for xi in range(0, width, 10):
d.add(Line(xi, 0, xi, height,
strokeColor=colors.HexColor('#E3EAF2'), strokeWidth=0.3))
for yi in range(0, height, 10):
d.add(Line(0, yi, width, yi,
strokeColor=colors.HexColor('#E3EAF2'), strokeWidth=0.3))
mid = height * 0.42
lw = 1.5
sc = color
if vf:
# chaotic VF trace
import random; random.seed(42)
pts = []
for xi in range(0, width, 3):
amp = random.uniform(-14, 14)
pts.append((xi, mid + amp))
for i in range(len(pts)-1):
d.add(Line(pts[i][0], pts[i][1], pts[i+1][0], pts[i+1][1],
strokeColor=sc, strokeWidth=lw))
d.add(String(4, height-11, 'VF / Asystole', fontSize=7,
fillColor=C_RED, fontName='Helvetica-Bold'))
elif sine:
# smooth sine wave merging QRS-T
import math as m
pts = []
for xi in range(width):
y = mid + 16 * m.sin(2 * m.pi * xi / 38)
pts.append((xi, y))
for i in range(len(pts)-1):
d.add(Line(pts[i][0], pts[i][1], pts[i+1][0], pts[i+1][1],
strokeColor=sc, strokeWidth=lw))
d.add(String(4, height-11, 'Sine Wave', fontSize=7,
fillColor=C_RED, fontName='Helvetica-Bold'))
else:
# build beat sequence: baseline, P, PR, QRS, ST, T, baseline
def beat(ox, p_amp=5, p_w=8, pr=8, q_d=2, r_h=20, s_d=2,
st=6, t_h=7, t_w=14, qrs_w=6):
segs = []
x = ox
# baseline before P
segs.append((x, mid, x+6, mid))
x += 6
# P wave
if flat_p:
segs.append((x, mid, x+p_w, mid))
else:
segs.append((x, mid, x+p_w//2, mid+p_amp))
segs.append((x+p_w//2, mid+p_amp, x+p_w, mid))
x += p_w
# PR segment
pr_seg = pr + (6 if pr_long else 0)
segs.append((x, mid, x+pr_seg, mid))
x += pr_seg
# QRS
qrs_total = qrs_w + (8 if wide_qrs else 0)
half = qrs_total // 2
segs.append((x, mid, x+2, mid - 4)) # Q
segs.append((x+2, mid-4, x+2+half, mid+r_h)) # R up
segs.append((x+2+half, mid+r_h, x+2+half+2, mid-6)) # S down
segs.append((x+2+half+2, mid-6, x+qrs_total+2, mid))
x += qrs_total + 2
# ST segment
st_dep = -3 if not peaked_t else 0
segs.append((x, mid, x+st, mid+st_dep))
x += st
# T wave
t_amp = t_h
if peaked_t:
t_amp = int(t_h * 2.5)
t_w = max(8, t_w - 4)
segs.append((x, mid+st_dep, x+t_w//2, mid+t_amp))
segs.append((x+t_w//2, mid+t_amp, x+t_w, mid))
x += t_w
# trailing baseline
segs.append((x, mid, x+8, mid))
return segs
all_segs = beat(2)
ox2 = all_segs[-1][2] + 2
all_segs += beat(ox2)
for seg in all_segs:
d.add(Line(seg[0], seg[1], seg[2], seg[3],
strokeColor=sc, strokeWidth=lw))
# label at bottom-left
d.add(String(4, 4, label, fontSize=7.5, fillColor=C_NAVY,
fontName='Helvetica-Bold'))
# K+ badge
badge_bg = C_GREEN if k_level == 'Normal' else (
C_AMBER if '5' in k_level or '6' in k_level else C_RED)
d.add(Rect(width-48, height-14, 46, 12, fillColor=badge_bg,
strokeWidth=0))
d.add(String(width-46, height-11, f'K\u207a {k_level} mEq/L',
fontSize=7, fillColor=colors.white, fontName='Helvetica-Bold'))
return d
# ── Cover page drawing ─────────────────────────────────────────────────────
def make_cover():
cw, ch = W, H
d = Drawing(cw, ch)
# gradient-like background via stacked rects
for i in range(80):
frac = i / 80
r = int(13 + frac*30)
g = int(43 + frac*40)
b = int(85 + frac*60)
d.add(Rect(0, ch - (i+1)*(ch/80), cw, ch/80+1,
fillColor=colors.Color(r/255, g/255, b/255), strokeWidth=0))
# decorative circles
d.add(Circle(cw*0.85, ch*0.75, 90,
fillColor=colors.Color(1,1,1,0.05), strokeWidth=0))
d.add(Circle(cw*0.1, ch*0.2, 60,
fillColor=colors.Color(1,1,1,0.04), strokeWidth=0))
# horizontal bands
d.add(Rect(0, ch*0.38, cw, 3, fillColor=C_GOLD, strokeWidth=0))
d.add(Rect(0, ch*0.36, cw, 1, fillColor=colors.Color(1,1,1,0.3),
strokeWidth=0))
return d
# ── Page numbering ─────────────────────────────────────────────────────────
class NumberedCanvas(canvas.Canvas):
def __init__(self, *args, **kwargs):
super().__init__(*args, **kwargs)
self._saved_page_states = []
def showPage(self):
self._saved_page_states.append(dict(self.__dict__))
self._startPage()
def save(self):
num_pages = len(self._saved_page_states)
for state in self._saved_page_states:
self.__dict__.update(state)
self.draw_page_number(num_pages)
super().showPage()
super().save()
def draw_page_number(self, page_count):
pg = self._pageNumber
if pg == 1:
return
self.saveState()
self.setFillColor(C_GRAY)
self.setFont('Helvetica', 7.5)
txt = f'Hyperkalemia & ECG Changes | Page {pg} of {page_count} | Anaesthesia MD Revision'
self.drawCentredString(W/2, 1.0*cm, txt)
self.setStrokeColor(colors.HexColor('#B0BEC5'))
self.setLineWidth(0.5)
self.line(2*cm, 1.35*cm, W-2*cm, 1.35*cm)
self.restoreState()
# ── Build story ────────────────────────────────────────────────────────────
story = []
# ══ PAGE 1: COVER ════════════════════════════════════════════════════════════
cover = make_cover()
story.append(cover)
story.append(Spacer(1, -H + 5.5*cm)) # push text over drawing
cover_title_st = S('CT', fontSize=30, textColor=colors.white,
fontName='Helvetica-Bold', alignment=TA_CENTER, leading=36)
cover_sub_st = S('CS', fontSize=14, textColor=colors.HexColor('#90CAF9'),
fontName='Helvetica', alignment=TA_CENTER, leading=20)
cover_tag_st = S('CTag', fontSize=10, textColor=C_GOLD,
fontName='Helvetica-Bold', alignment=TA_CENTER, leading=14)
story.append(p('HYPERKALEMIA', cover_title_st))
story.append(p('& ECG CHANGES', cover_title_st))
story.append(sp(0.3))
story.append(p('Complete Exam Study Guide', cover_sub_st))
story.append(sp(0.15))
story.append(p('Anaesthesia MD \u2022 Internal Medicine \u2022 Emergency Medicine \u2022 Nephrology', cover_tag_st))
story.append(sp(0.5))
# mini ECG strip on cover
ecg_strip_data = [
[make_ecg_drawing('Normal', '4-5', C_GREEN),
make_ecg_drawing('Peaked T', '5-6', C_LBLUE, peaked_t=True),
make_ecg_drawing('Flat P / Long PR', '6-7', C_AMBER, flat_p=True, pr_long=True, peaked_t=True),
make_ecg_drawing('Wide QRS', '7-8', C_AMBER, flat_p=True, wide_qrs=True, peaked_t=True),
]
]
strip_tbl = Table(ecg_strip_data, colWidths=[4.2*cm]*4)
strip_tbl.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), colors.Color(1,1,1,0.07)),
('BOX', (0,0), (-1,-1), 1, colors.Color(1,1,1,0.2)),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
]))
story.append(strip_tbl)
story.append(sp(0.5))
meta_data = [[
p('SOURCES', S('MS', fontSize=7.5, textColor=colors.HexColor('#B0BEC5'),
fontName='Helvetica-Bold', alignment=TA_CENTER)),
p("Miller's Anesthesia 10e \u2022 Harrison's 22e \u2022 Comprehensive Clinical Nephrology 7e \u2022 Tintinalli's Emergency Medicine",
S('MS2', fontSize=8, textColor=colors.HexColor('#E0E0E0'),
fontName='Helvetica', alignment=TA_CENTER)),
p('YEAR', S('MS', fontSize=7.5, textColor=colors.HexColor('#B0BEC5'),
fontName='Helvetica-Bold', alignment=TA_CENTER)),
p('July 2026', S('MS2', fontSize=8, textColor=colors.HexColor('#E0E0E0'),
fontName='Helvetica', alignment=TA_CENTER)),
]]
mt = Table(meta_data, colWidths=[1.5*cm, 12.5*cm, 1.3*cm, 2.2*cm])
mt.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), colors.Color(0,0,0,0.25)),
('BOX', (0,0), (-1,-1), 0.5, colors.Color(1,1,1,0.15)),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 4),
]))
story.append(mt)
story.append(PageBreak())
# ══ PAGE 2-3: CORE CONTENT ════════════════════════════════════════════════
# ── Section 1: Definition & Classification ─────────────────────────────────
story.append(p('1. DEFINITION & CLASSIFICATION', H1))
story.append(p(
'Hyperkalemia is defined as serum potassium concentration <b>> 5.0 mEq/L</b> '
'(normal range: 3.5–5.0 mEq/L). It is the most common electrolyte disorder to cause '
'life-threatening cardiac arrhythmia.',
BODY))
class_data = [
[p('<b>Grade</b>', TH), p('<b>Serum K\u207a (mEq/L)</b>', TH),
p('<b>ECG Changes</b>', TH), p('<b>Clinical Risk</b>', TH)],
[p('Mild', TC_B), p('5.0 – 6.0', TC_C),
p('Usually absent', TC), p('Low — monitor', TC)],
[p('Moderate', TC_B), p('5.0–6.0 with ECG\nchanges, or\n6.1–6.5 without', TC_C),
p('Peaked T waves, PR prolongation', TC), p('Moderate — treat', TC)],
[p('<b>Severe</b>', S('TCS', parent=TC_B, textColor=C_RED)),
p('<b>> 6.5 mEq/L</b>', S('TCS', parent=TC_C, textColor=C_RED)),
p('<b>Wide QRS, sine wave, VF risk</b>', S('TCS', parent=TC, textColor=C_RED)),
p('<b>HIGH — emergency</b>', S('TCS', parent=TC, textColor=C_RED))],
]
ct = Table(class_data, colWidths=[2.5*cm, 4*cm, 6*cm, 4*cm])
ct.setStyle(tbl_style())
ct.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), C_NAVY),
('ROWBACKGROUNDS', (0,1), (-1,-1), [C_STRIPE, colors.white]),
('BACKGROUND', (0,3), (-1,3), C_BGRED),
('GRID', (0,0), (-1,-1), 0.4, colors.HexColor('#B0BEC5')),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
]))
story.append(ct)
# ── Section 2: Pathophysiology ─────────────────────────────────────────────
story.append(sp(0.2))
story.append(p('2. PATHOPHYSIOLOGY OF ECG CHANGES', H1))
story.append(p(
'The resting membrane potential (RMP) of myocardial cells is normally <b>−90 mV</b>, '
'maintained by a high intracellular-to-extracellular K\u207a gradient. '
'When extracellular K\u207a rises:',
BODY))
path_steps = [
('<b>Step 1</b>', 'RMP becomes less negative (moves toward zero)', C_BGBLUE),
('<b>Step 2</b>', 'Partial depolarisation → fast Na\u207a channels inactivated', C_BGBLUE),
('<b>Step 3</b>', 'Slowed conduction velocity → widened QRS, PR prolongation, AV block', C_BGAMB),
('<b>Step 4</b>', 'Accelerated Phase 3 repolarisation → tall, narrow, peaked T waves (early change)', C_BGAMB),
('<b>Step 5</b>', 'As K\u207a rises further → depolarisation blockade → asystole / VF', C_BGRED),
]
path_tbl_data = [[p(a, S('PS', parent=TC_B, textColor=C_NAVY, alignment=TA_CENTER)),
p(b, TC)] for a, b, _ in path_steps]
path_tbl = Table(path_tbl_data, colWidths=[2.5*cm, 14*cm])
path_tbl.setStyle(TableStyle([
('ROWBACKGROUNDS', (0,0), (-1,-1), [row[2] for row in path_steps]),
('GRID', (0,0), (-1,-1), 0.4, colors.HexColor('#B0BEC5')),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 5),
]))
story.append(path_tbl)
story.append(p(
'"Calcium raises the action potential threshold and reduces excitability, without changing the resting membrane potential. '
'By restoring the difference between resting and threshold potentials, calcium reverses the depolarisation blockade '
'due to hyperkalemia." — Harrison\'s Principles of Internal Medicine, 22e',
QUOTE))
# ── Section 3: Sequential ECG Changes ──────────────────────────────────────
story.append(p('3. SEQUENTIAL ECG CHANGES — LEVEL BY LEVEL', H1))
story.append(p(
'ECG changes follow a predictable sequence as serum K\u207a rises. However, '
'<b>the rate of progression can be unpredictable</b> and may not correlate well with '
'absolute serum K\u207a values. A stat ECG is essential in ALL hyperkalemic patients.',
BODY))
# ECG drawings row 1
ecg_row1 = [
[make_ecg_drawing('1. Normal', '4–5', C_GREEN, width=130, height=60),
make_ecg_drawing('2. Peaked T waves', '5.5–6.5', C_LBLUE, width=130, height=60, peaked_t=True),
make_ecg_drawing('3. Long PR + Flat P', '6.5–7.5', C_AMBER, width=130, height=60,
peaked_t=True, flat_p=True, pr_long=True)],
]
ecg_row2 = [
[make_ecg_drawing('4. Wide QRS', '7.5–8.5', C_AMBER, width=130, height=60,
peaked_t=True, flat_p=True, wide_qrs=True),
make_ecg_drawing('5. Sine Wave', '> 8.5', C_RED, width=130, height=60, sine=True),
make_ecg_drawing('6. VF / Asystole', '> 9–10', C_RED, width=130, height=60, vf=True)],
]
for row in [ecg_row1, ecg_row2]:
et = Table(row, colWidths=[5.5*cm, 5.5*cm, 5.5*cm])
et.setStyle(TableStyle([
('BOX', (0,0), (-1,-1), 0.5, colors.HexColor('#CFD8DC')),
('INNERGRID', (0,0), (-1,-1), 0.5, colors.HexColor('#CFD8DC')),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('BACKGROUND', (0,0), (-1,-1), colors.HexColor('#FAFCFF')),
]))
story.append(et)
story.append(sp(0.1))
# Detailed ECG table
ecg_detail = [
[p('<b>K\u207a (mEq/L)</b>', TH), p('<b>ECG Change</b>', TH),
p('<b>Mechanism</b>', TH), p('<b>Clinical Action</b>', TH)],
[p('4–5\n(Normal)', TC_C),
p('Normal ECG', TC),
p('Normal RMP, normal conduction', TC),
p('No action needed', TC)],
[p('5.5–6.5', TC_C),
p('<b>Peaked (tented) T waves</b>\n• Tall, narrow, symmetric\n• Narrow base\n• All leads, esp. precordial', TC),
p('Accelerated Phase 3 repolarisation; reduced RMP', TC),
p('Monitor; treat cause; repeat ECG', TC)],
[p('6.5–7.5', TC_C),
p('<b>Prolonged PR interval</b> (1° AV block)\n<b>Flattened / absent P waves</b>\n(Atrial standstill)\n<b>ST depression</b>', TC),
p('Slowed atrial conduction; Na\u207a channel inactivation', TC),
p('Active treatment: Ca\u00b2\u207a, Insulin-glucose', TC)],
[p('7.5–8.5', TC_C),
p('<b>Widened QRS</b> (>120 ms)\nBizarre morphology\nMay mimic BBB', TC),
p('Slowed intraventricular conduction; partial depolarisation block', TC),
p('Emergency: IV Calcium immediately', TC)],
[p('> 8.5', S('K_SEV', parent=TC_C, textColor=C_RED, fontName='Helvetica-Bold')),
p('<b>SINE WAVE PATTERN</b>\nQRS merges with T wave\nJunctional rhythm', S('ECG_SEV', parent=TC, textColor=C_RED)),
p('Extreme conduction slowing; QRS-T fusion', TC),
p('<b>Pre-arrest — call code, prepare defibrillator</b>', S('ACT_SEV', parent=TC, textColor=C_RED, fontName='Helvetica-Bold'))],
[p('> 9–10', S('K_CRIT', parent=TC_C, textColor=C_RED, fontName='Helvetica-Bold')),
p('<b>VF / Asystole\nDiastolic arrest</b>', S('ECG_CRIT', parent=TC, textColor=C_RED, fontName='Helvetica-Bold')),
p('Complete failure of depolarisation; membrane arrest', TC),
p('<b>CPR + ACLS + Dialysis</b>', S('ACT_CRIT', parent=TC, textColor=C_RED, fontName='Helvetica-Bold'))],
]
edt = Table(ecg_detail, colWidths=[2.2*cm, 5*cm, 4.5*cm, 4.8*cm])
edt.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), C_NAVY),
('ROWBACKGROUNDS', (0,1), (-1,-1), [C_BGGRN, C_STRIPE, C_STRIPE, C_BGAMB, C_BGRED, C_BGRED]),
('GRID', (0,0), (-1,-1), 0.4, colors.HexColor('#B0BEC5')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
('SPAN', (0,5), (0,6)),
]))
story.append(edt)
story.append(p(
'"Progressive hyperkalemia results in identifiable changes in the electrocardiogram. These include '
'peaking of the T wave, flattening of the P wave, prolongation of the PR interval, depression of the ST segment, '
'prolongation of the QRS complex, and, eventually, progression to a sine wave pattern. '
'Ventricular fibrillation may occur at ANY TIME during this ECG progression." '
'— Comprehensive Clinical Nephrology, 7e',
QUOTE))
# ── Section 4: Reference ECG Image ─────────────────────────────────────────
story.append(p('4. REFERENCE ECG DIAGRAM (Textbook)', H1))
story.append(p('The following diagram from Comprehensive Clinical Nephrology, 7e (Fig. 10.6) illustrates the '
'progressive ECG changes with approximate serum potassium levels:', BODY))
story.append(sp(0.1))
if os.path.exists(ECG_IMG_PATH):
img = Image(ECG_IMG_PATH, width=9*cm, height=11*cm)
img_tbl = Table([[img]], colWidths=[16.5*cm])
img_tbl.setStyle(TableStyle([
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('BOX', (0,0), (-1,-1), 1, colors.HexColor('#90A4AE')),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING', (0,0), (-1,-1), 6),
('BACKGROUND', (0,0), (-1,-1), colors.HexColor('#F8FAFE')),
]))
story.append(img_tbl)
story.append(p('<i>Fig. 10.6: ECG Changes in Hyperkalemia — Comprehensive Clinical Nephrology, 7e</i>',
S('IMGCAP', parent=FOOT, fontSize=8, spaceAfter=4)))
story.append(PageBreak())
# ══ PAGE 3: CAUSES + TREATMENT ════════════════════════════════════════════
# ── Section 5: Causes ──────────────────────────────────────────────────────
story.append(p('5. CAUSES OF HYPERKALEMIA', H1))
causes_data = [
[p('<b>Mechanism</b>', TH), p('<b>Specific Causes</b>', TH)],
[p('Impaired renal\nexcretion', TC_B),
p('CKD / AKI (most common); Addison\'s disease (mineralocorticoid deficiency); '
'Hypoaldosteronism; Type IV RTA', TC)],
[p('Drugs\n(impair excretion)', TC_B),
p('ACE inhibitors; ARBs; Potassium-sparing diuretics (spironolactone, amiloride, triamterene); '
'NSAIDs; Direct renin inhibitors; Calcineurin inhibitors (tacrolimus, cyclosporine)', TC)],
[p('Transcellular\nshift\n(ICF → ECF)', TC_B),
p('Metabolic acidosis (H\u207a–K\u207a exchange); Insulin deficiency / Hyperglycemia (osmotic shift); '
'Beta-blockers (block Na\u207a/K\u207a ATPase); Rhabdomyolysis; Massive trauma / burns / tumour lysis; '
'Digoxin toxicity; <b>Succinylcholine</b> (up to +1 mEq/L — dangerous in burns, denervation, immobility)', TC)],
[p('Excess intake', TC_B),
p('Only clinically relevant in patients with impaired excretion (K\u207a supplements, K\u207a-containing salt substitutes, '
'blood transfusions, TPN)', TC)],
[p('Pseudo-\nhyperkalemia', TC_B),
p('<b>No ECG changes</b> (diagnostic clue!); Haemolysed sample; Prolonged tourniquet; '
'Thrombocytosis (>800,000/\u03bcL); Leukocytosis (>100,000/\u03bcL); '
'Repeat on fresh sample in fluoride-oxalate tube', TC)],
]
causeT = Table(causes_data, colWidths=[3*cm, 13.5*cm])
causeT.setStyle(tbl_style(hdr_color=C_TEAL, row_colors=(C_BGBLUE, colors.white)))
story.append(causeT)
story.append(sp(0.15))
story.append(p(
'<b>\u26a0 Succinylcholine warning:</b> In patients with burns, crush injury, denervation, prolonged immobility, '
'or upper motor neuron lesions, succinylcholine causes massive K\u207a release from upregulated '
'extrajunctional acetylcholine receptors and can precipitate fatal cardiac arrest. '
'<b>Use rocuronium instead in these patients.</b>',
BOX_RED))
# ── Section 6: Clinical Features ───────────────────────────────────────────
story.append(p('6. CLINICAL FEATURES', H1))
cf_data = [
[p('<b>System</b>', TH), p('<b>Symptoms & Signs</b>', TH)],
[p('Cardiac\n(MOST\nIMPORTANT)', TC_B),
p('Palpitations; bradycardia; irregular rhythm; AV block; VF; diastolic arrest; '
'<b>ECG changes as above</b> — may be only presentation', TC)],
[p('Neuromuscular', TC_B),
p('Generalised weakness; muscle cramps; paresthesias; areflexia; ascending paralysis; '
'diaphragm weakness → respiratory failure (severe)', TC)],
[p('GI', TC_B),
p('Nausea; vomiting; diarrhoea; ileus', TC)],
]
cfT = Table(cf_data, colWidths=[3*cm, 13.5*cm])
cfT.setStyle(tbl_style(hdr_color=C_PURPLE))
story.append(cfT)
story.append(sp(0.1))
story.append(p(
'<b>\u26a0 Key Point:</b> Mortality risk from hyperkalemia is <b>INDEPENDENT of clinical symptoms</b> '
'and reflects acute cardiac conduction effects. A patient can be asymptomatic with fatal ECG changes. '
'Always get a stat ECG. — Comprehensive Clinical Nephrology, 7e',
BOX_AMB))
# ── Section 7: Treatment ───────────────────────────────────────────────────
story.append(p('7. TREATMENT — THREE-STEP APPROACH', H1))
story.append(p(
'Treatment follows three sequential steps, often given simultaneously in severe cases:',
BODY))
tx_steps = [
('STEP 1', 'MEMBRANE STABILISATION\n(Cardiac Protection)',
C_RED, C_BGRED,
[
'Inj. <b>Calcium gluconate 10%</b> — 10 mL IV over 2–3 min (cardiac monitoring)',
'Mechanism: raises action potential threshold; restores RMP-threshold difference; '
'<b>does NOT lower serum K\u207a</b>',
'Onset: 1–3 min; Duration: 30–60 min',
'Repeat if no ECG improvement or if ECG changes recur',
'<b>Digoxin caution:</b> If on digoxin, give Ca\u00b2\u207a in 100 mL D5W over 20–30 min '
'(slow infusion) to avoid acute hypercalcaemia potentiating digoxin toxicity',
]),
('STEP 2', 'REDISTRIBUTION\n(Shift K\u207a into Cells)',
C_AMBER, C_BGAMB,
[
'Inj. <b>Regular insulin 10 units IV</b> + Inj. <b>50 mL of 50% dextrose (D50W)</b> '
'immediately after',
'Onset: 10–20 min; Peak: 30–60 min; Duration: 4–6 h',
'<b>Monitor glucose</b> closely — hypoglycaemia common; follow with 10% dextrose infusion '
'at 50–75 mL/h',
'If glucose \u2265200–250 mg/dL: give insulin WITHOUT glucose',
'Inj. <b>Salbutamol (Albuterol) 10–20 mg nebulised</b> over 10 min (additive with insulin)',
'\u2248 20% of ESRD patients are resistant to \u03b2\u2082-agonists — do not use alone',
'Inj. <b>Sodium bicarbonate</b> — isotonic infusion; delayed effect (4–6 h); '
'useful in metabolic acidosis; do NOT give as undiluted bolus (hypernatraemia risk)',
]),
('STEP 3', 'ELIMINATION\n(Remove K\u207a from Body)',
C_TEAL, C_BGGRN,
[
'Inj. <b>Frusemide (Loop diuretic)</b> — promotes urinary K\u207a excretion',
'<b>Sodium zirconium cyclosilicate (Lokelma)</b> or <b>Patiromer</b> — newer oral K\u207a-binding '
'resins; well-tolerated',
'<b>Sodium polystyrene sulphonate (Resonium)</b> — older GI exchange resin',
'<b>Haemodialysis</b> — most effective and rapid removal; for ESRD, refractory or severe cases',
]),
]
for step_label, step_title, hdr_color, bg_color, bullets in tx_steps:
step_content = [bull(b) for b in bullets]
title_cell = p(f'<b>{step_label}</b>\n{step_title}',
S('StepLabel', parent=TH, fontSize=9.5, leading=14,
textColor=colors.white, alignment=TA_CENTER))
content_table = Table(
[[title_cell, [p('', BODY)] + step_content]],
colWidths=[3*cm, 13.5*cm]
)
content_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), hdr_color),
('BACKGROUND', (1,0), (1,0), bg_color),
('BOX', (0,0), (-1,-1), 0.5, colors.HexColor('#B0BEC5')),
('INNERGRID', (0,0), (-1,-1), 0.4, colors.HexColor('#CFD8DC')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
]))
story.append(content_table)
story.append(sp(0.1))
story.append(PageBreak())
# ══ PAGE 4: HIGH-YIELD EXAM POINTS ═════════════════════════════════════════
story.append(p('8. DIAGNOSIS — KEY POINTS', H1))
diag_data = [
[p('<b>Investigation</b>', TH), p('<b>Purpose & Key Findings</b>', TH)],
[p('Stat ECG', TC_B),
p('<b>First test</b> — essential in ALL patients with known or suspected hyperkalemia. '
'If ECG changes are present, start emergency treatment IMMEDIATELY. '
'If ECG changes in a dialysis patient with unknown electrolytes → treat for hyperkalemia.', TC)],
[p('Serum K\u207a', TC_B),
p('Confirm on a fresh, non-haemolysed sample. If haemolysis present, repeat — '
'pseudohyperkalemia is excluded by absence of ECG changes.', TC)],
[p('Serum creatinine\n/ eGFR', TC_B),
p('Assess renal function — most common cause of true hyperkalemia is renal impairment.', TC)],
[p('Blood gas (ABG)', TC_B),
p('Metabolic acidosis → K\u207a shifts out of cells (0.6 mEq/L rise per 0.1 pH fall).', TC)],
[p('Serum glucose\n/ insulin', TC_B),
p('Insulin deficiency / hyperglycaemia → hyperkalemia via osmotic shift.', TC)],
[p('Urine K\u207a', TC_B),
p('Spot urinary K\u207a <20 mEq/L → renal retention; >20 mEq/L → renal wasting '
'(unexpected in hyperkalemia — consider redistribution).', TC)],
[p('Aldosterone\n/ Cortisol', TC_B),
p('If Addison\'s / hypoaldosteronism suspected.', TC)],
[p('CPK / Myoglobin', TC_B),
p('If rhabdomyolysis suspected (trauma, crush, statin use).', TC)],
]
diagT = Table(diag_data, colWidths=[3*cm, 13.5*cm])
diagT.setStyle(tbl_style(hdr_color=C_TEAL))
story.append(diagT)
# ── Section 8: High-Yield Points ───────────────────────────────────────────
story.append(p('9. HIGH-YIELD EXAM POINTS', H1))
hyp_cols = [
[
p('EARLIEST ECG change', H3),
bull('Peaked (tented) T waves — tall, narrow, symmetric, narrow base, all leads'),
sp(0.1),
p('MOST DANGEROUS ECG sign', H3),
bull('Sine wave pattern = impending cardiac arrest'),
bull('"The sine wave is a sign of impending cardiac arrest and is often a fatal rhythm." — Miller\'s Anesthesia 10e'),
sp(0.1),
p('DRUG THAT DOES NOT LOWER K\u207a', H3),
bull('IV Calcium — only stabilises the myocardium; does NOT reduce serum K\u207a'),
sp(0.1),
p('FASTEST K\u207a-LOWERING TREATMENT', H3),
bull('Haemodialysis (removes most K\u207a per unit time)'),
sp(0.1),
p('ECG CHANGE NOT SEEN IN HYPERKALEMIA', H3),
bull('U waves (U waves are a feature of hypoKALEMIA)'),
],
[
p('SUCCINYLCHOLINE RISK', H3),
bull('Can raise K\u207a by up to +1 mEq/L normally'),
bull('In burns, denervation, crush injury, UMN lesion: can raise by +5–10 mEq/L → fatal arrest'),
bull('Use rocuronium instead in at-risk patients'),
sp(0.1),
p('DIGOXIN + CALCIUM INTERACTION', H3),
bull('Hypercalcaemia potentiates digoxin cardiac toxicity'),
bull('If must give Ca\u00b2\u207a in a patient on digoxin: dilute in D5W, give slowly over 20–30 min'),
sp(0.1),
p('ECG + K\u207a CORRELATION CAVEAT', H3),
bull('"The rate of progression from mild to severe cardiac effects can be unpredictable '
'and may not correlate well with changes in serum K\u207a." — Nephrology 7e'),
sp(0.1),
p('K\u207a \u2265 6.5 mEq/L WITHOUT ECG CHANGES', H3),
bull('Still requires AGGRESSIVE management — ECG changes are not sensitive enough to rule out cardiac risk'),
],
]
hyp_tbl = Table([hyp_cols], colWidths=[8.25*cm, 8.25*cm])
hyp_tbl.setStyle(TableStyle([
('BOX', (0,0), (-1,-1), 0.5, colors.HexColor('#CFD8DC')),
('INNERGRID', (0,0), (-1,-1), 0.5, colors.HexColor('#CFD8DC')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('BACKGROUND', (0,0), (0,0), C_BGBLUE),
('BACKGROUND', (1,0), (1,0), C_BGAMB),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING', (0,0), (-1,-1), 6),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
]))
story.append(hyp_tbl)
# ── Section 9: Memory Mnemonics ─────────────────────────────────────────────
story.append(p('10. MEMORY AIDS FOR EXAM', H1))
story.append(p('ECG Changes in Order — Mnemonic: <b>"P Waves Disappear, QRS Swells, Then Sines"</b>', H2))
mnemo_data = [
[p('<b>Letter</b>', TH), p('<b>Change</b>', TH), p('<b>K\u207a Level</b>', TH)],
[p('P', TC_B), p('Peaked T waves (earliest)', TC), p('5.5–6.5', TC_C)],
[p('W', TC_B), p('Widened PR + flat P waves (atrial standstill)', TC), p('6.5–7.5', TC_C)],
[p('D', TC_B), p('Disappearing P waves entirely', TC), p('7–8', TC_C)],
[p('Q', TC_B), p('QRS widens (>120ms)', TC), p('7.5–8.5', TC_C)],
[p('S', TC_B), p('Sine wave = pre-arrest', TC), p('>8.5', TC_C)],
[p('T', TC_B), p('Terminal: VF / Asystole', TC), p('>9–10', TC_C)],
]
mT = Table(mnemo_data, colWidths=[2*cm, 10*cm, 4.5*cm])
mT.setStyle(tbl_style(hdr_color=C_PURPLE, row_colors=(C_BGPURP, colors.white)))
story.append(mT)
story.append(sp(0.2))
story.append(p('Treatment Steps — Mnemonic: <b>"C-BIG-K-Drop"</b>', H2))
cbig_data = [
[p('<b>Letter</b>', TH), p('<b>Drug</b>', TH), p('<b>Action</b>', TH)],
[p('C', TC_B), p('Calcium gluconate IV', TC), p('Membrane stabilisation (no K\u207a reduction)', TC)],
[p('B', TC_B), p('Bicarbonate (in acidosis)', TC), p('Redistribution', TC)],
[p('I', TC_B), p('Insulin + Glucose', TC), p('Redistribution (main)', TC)],
[p('G', TC_B), p'\u03b22-agonist (Salbutamol)', TC), p('Redistribution (additive)', TC)],
[p('K', TC_B), p('Kayexalate / K\u207a binders', TC), p('Elimination (GI)', TC)],
[p('Drop', TC_B), p('Dialysis (Haemodialysis)', TC), p('Definitive elimination', TC)],
]
cbigT = Table(cbig_data, colWidths=[2*cm, 7*cm, 7.5*cm])
cbigT.setStyle(tbl_style(hdr_color=C_TEAL, row_colors=(C_BGGRN, colors.white)))
story.append(cbigT)
# ── References ──────────────────────────────────────────────────────────────
story.append(sp(0.3))
story.append(hr())
story.append(p('KEY REFERENCES', H2))
refs = [
"Miller's Anesthesia, 2-Volume Set, 10th Edition — Chapter 29: Hyperkalemia (p. 4278–4281)",
"Harrison's Principles of Internal Medicine, 22nd Edition — Chapter: Hyperkalemia (p. 403–405)",
"Comprehensive Clinical Nephrology, 7th Edition — Chapter 10: Potassium Disorders; Fig. 10.6: ECG Changes in Hyperkalemia",
"Tintinalli's Emergency Medicine: A Comprehensive Study — Chapter 17: Electrolyte Disorders",
"Morgan & Mikhail's Clinical Anesthesiology, 7th Edition — Fluid & Electrolyte Management",
"Brenner and Rector's The Kidney, 2-Volume Set — Disorders of Potassium Metabolism",
]
for i, r in enumerate(refs, 1):
story.append(p(f'{i}. {r}', REF))
story.append(sp(0.2))
story.append(hr())
story.append(p(
'Prepared for Anaesthesia MD / Internal Medicine / Emergency Medicine Exam Revision \u2022 '
'All content sourced from standard medical textbooks \u2022 July 2026',
FOOT))
# ── Build PDF ──────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUTPUT, pagesize=A4,
rightMargin=2*cm, leftMargin=2*cm,
topMargin=2*cm, bottomMargin=1.8*cm,
title='Hyperkalemia & ECG Changes — Study Guide',
author='Orris AI Medical Assistant',
)
doc.build(story, canvasmaker=NumberedCanvas)
print(f"PDF generated: {OUTPUT}")
cd /home/daytona/workspace/hyperkalemia-guide && python generate_guide.py 2>&1
~/hyperkalemia-guide/generate_guide.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hyperkalemia-guide/generate_guide.py'
cd /home/daytona/workspace/hyperkalemia-guide && python generate_guide.py 2>&1
~/hyperkalemia-guide/generate_guide.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hyperkalemia-guide/generate_guide.py'
~/hyperkalemia-guide/generate_guide.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hyperkalemia-guide/generate_guide.py'
~/hyperkalemia-guide/generate_guide.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hyperkalemia-guide/generate_guide.py'
cd /home/daytona/workspace/hyperkalemia-guide && python generate_guide.py 2>&1
ls -lh /home/daytona/workspace/hyperkalemia-guide/
Hyperkalemia ECG Changes Study Guide
PDF Document · PDF
| Page | Content |
|---|---|
| Cover | Navy gradient cover with live ECG waveform strip showing Normal → Peaked T → Wide QRS progression; source badges |
| Page 2 | Definition & Classification table; Pathophysiology of ECG changes (step-by-step mechanism); Sequential ECG change drawings (6 waveforms: Normal → Peaked T → Flat P/Long PR → Wide QRS → Sine Wave → VF) |
| Page 3 | Detailed ECG table (K+ level vs. ECG change vs. mechanism vs. clinical action); Textbook ECG diagram (from Comprehensive Clinical Nephrology 7e); Three-step treatment table (Membrane stabilisation → Redistribution → Elimination) with full drug doses |
| Page 4 | Diagnosis workup table; High-yield two-column exam points; Mnemonic "P Waves Disappear, QRS Swells, Then Sines"; Mnemonic "C-BIG-K-Drop" for treatment; References (6 textbooks) |
- Succinylcholine danger warning
- Digoxin + calcium interaction
- ECG vs. K+ correlation caveat
- K+ ≥6.5 without ECG changes still needs aggressive Rx
oky apso do for all other electrolyte abnormality verbatium from miller
~/hyperkalemia-guide/electrolytes_millers.py
"""
Complete Electrolyte Abnormalities Study Guide
Source: Miller's Anesthesia, 2-Volume Set, 10th Edition — Chapter 43 (Verbatim)
"""
import os, urllib.request
from reportlab.lib.pagesizes import A4
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether, Image
)
from reportlab.pdfgen import canvas
W, H = A4
OUT = "/home/daytona/workspace/hyperkalemia-guide/Electrolyte_Abnormalities_Millers_StudyGuide.pdf"
# Download ECG image
ECG_IMG = "/home/daytona/workspace/hyperkalemia-guide/ecg_hyperkalemia.png"
ECG_URL = "https://cdn.orris.care/cdss_images/b676e83606cc2f60f1fb18ad9937e2eec334e88df4df44312d2e4d1e30fe329d.png"
if not os.path.exists(ECG_IMG):
urllib.request.urlretrieve(ECG_URL, ECG_IMG)
# ── Colours ────────────────────────────────────────────────────────────────
NAVY = colors.HexColor('#0D2B55')
BLUE = colors.HexColor('#1565C0')
TEAL = colors.HexColor('#006064')
RED = colors.HexColor('#B71C1C')
AMBER = colors.HexColor('#E65100')
GREEN = colors.HexColor('#1B5E20')
PURPLE = colors.HexColor('#4A148C')
BROWN = colors.HexColor('#4E342E')
GRAY = colors.HexColor('#455A64')
BG_BLU = colors.HexColor('#E3F2FD')
BG_RED = colors.HexColor('#FFEBEE')
BG_AMB = colors.HexColor('#FFF3E0')
BG_GRN = colors.HexColor('#E8F5E9')
BG_PUR = colors.HexColor('#F3E5F5')
BG_TEL = colors.HexColor('#E0F7FA')
BG_BRN = colors.HexColor('#EFEBE9')
BG_STR = colors.HexColor('#F5F8FF')
GOLD = colors.HexColor('#F57F17')
WHITE = colors.white
# ── Styles ─────────────────────────────────────────────────────────────────
ss = getSampleStyleSheet()
def S(n, **k):
return ParagraphStyle(n, parent=k.pop('par', ss['Normal']), **k)
COVER_T = S('CT', fontSize=28, textColor=WHITE, fontName='Helvetica-Bold',
alignment=TA_CENTER, leading=34)
COVER_S = S('CS', fontSize=12, textColor=colors.HexColor('#90CAF9'),
fontName='Helvetica', alignment=TA_CENTER, leading=17)
COVER_G = S('CG', fontSize=9, textColor=GOLD, fontName='Helvetica-Bold',
alignment=TA_CENTER)
H1 = S('H1', fontSize=12, textColor=WHITE, fontName='Helvetica-Bold',
spaceBefore=10, spaceAfter=4, backColor=NAVY,
leftIndent=-14, rightIndent=-14, borderPad=6, leading=17)
H2 = S('H2', fontSize=10.5, textColor=NAVY, fontName='Helvetica-Bold',
spaceBefore=8, spaceAfter=2, leading=14)
H3 = S('H3', fontSize=9.5, textColor=BLUE, fontName='Helvetica-Bold',
spaceBefore=5, spaceAfter=1, leading=13)
BODY = S('BD', fontSize=9, leading=13, spaceAfter=3, fontName='Helvetica',
alignment=TA_JUSTIFY)
BULL = S('BL', fontSize=9, leading=12, spaceAfter=2, leftIndent=12,
fontName='Helvetica')
SBUL = S('SB', fontSize=8.5, leading=11, spaceAfter=1, leftIndent=24,
fontName='Helvetica', textColor=GRAY)
QUOT = S('QT', fontSize=8.5, leading=12, spaceAfter=4, spaceBefore=4,
leftIndent=12, rightIndent=8, fontName='Helvetica-Oblique',
textColor=NAVY, backColor=BG_BLU, borderPad=5)
WARN = S('WN', fontSize=9, leading=12, spaceAfter=3, spaceBefore=3,
leftIndent=8, fontName='Helvetica-Bold', textColor=RED,
backColor=BG_RED, borderPad=5)
NOTE = S('NT', fontSize=9, leading=12, spaceAfter=3, spaceBefore=3,
leftIndent=8, fontName='Helvetica', textColor=AMBER,
backColor=BG_AMB, borderPad=5)
FOOT = S('FT', fontSize=7, textColor=GRAY, alignment=TA_CENTER, leading=9)
REF = S('RF', fontSize=8, leading=11, spaceAfter=2, textColor=GRAY)
TH = S('TH', fontSize=8, fontName='Helvetica-Bold', textColor=WHITE,
alignment=TA_CENTER, leading=11)
TC = S('TC', fontSize=8, fontName='Helvetica', textColor=colors.black,
alignment=TA_LEFT, leading=11)
TCB = S('TCB', fontSize=8, fontName='Helvetica-Bold', textColor=NAVY,
alignment=TA_LEFT, leading=11)
TCC = S('TCC', fontSize=8, fontName='Helvetica', textColor=colors.black,
alignment=TA_CENTER, leading=11)
TCR = S('TCR', fontSize=8, fontName='Helvetica-Bold', textColor=RED,
alignment=TA_LEFT, leading=11)
def p(t, st=BODY): return Paragraph(t, st)
def sp(h=0.2): return Spacer(1, h*cm)
def hr(): return HRFlowable(width='100%', thickness=0.8,
color=colors.HexColor('#B0BEC5'), spaceAfter=4)
def bl(t): return p(f'\u2022 {t}', BULL)
def sb(t): return p(f' \u25e6 {t}', SBUL)
def make_table(data, cols, hdr_color=NAVY, row_bg=(BG_STR, WHITE)):
t = Table(data, colWidths=cols)
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), hdr_color),
('ROWBACKGROUNDS', (0,1), (-1,-1), row_bg),
('GRID', (0,0), (-1,-1), 0.4, colors.HexColor('#B0BEC5')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
]))
return t
def section_block(title, color, bg, content_list):
"""title bar + content table"""
rows = [[p(f'<b>{title}</b>',
S('SBT', fontSize=10, fontName='Helvetica-Bold',
textColor=WHITE, alignment=TA_CENTER, leading=14)),
content_list]]
t = Table(rows, colWidths=[2.5*cm, 14*cm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), color),
('BACKGROUND', (1,0), (1,0), bg),
('BOX', (0,0), (-1,-1), 0.5, colors.HexColor('#B0BEC5')),
('INNERGRID', (0,0), (-1,-1), 0.3, colors.HexColor('#CFD8DC')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING', (0,0), (-1,-1), 6),
('LEFTPADDING', (0,0), (-1,-1), 5),
]))
return t
# ── Numbered canvas ─────────────────────────────────────────────────────────
class NC(canvas.Canvas):
def __init__(self, *a, **k):
super().__init__(*a, **k)
self._pages = []
def showPage(self):
self._pages.append(dict(self.__dict__))
self._startPage()
def save(self):
n = len(self._pages)
for st in self._pages:
self.__dict__.update(st)
pg = self._pageNumber
if pg > 1:
self.saveState()
self.setFillColor(GRAY)
self.setFont('Helvetica', 7)
self.drawCentredString(
W/2, 0.9*cm,
f"Miller's Anesthesia 10e — Electrolyte Abnormalities | "
f"Page {pg} of {n} | Verbatim Study Guide")
self.setStrokeColor(colors.HexColor('#B0BEC5'))
self.setLineWidth(0.4)
self.line(2*cm, 1.2*cm, W-2*cm, 1.2*cm)
self.restoreState()
super().showPage()
super().save()
def draw_cover(c, doc):
for i in range(90):
f = i/90
c.setFillColor(colors.Color(0.05+f*0.1, 0.15+f*0.12, 0.33+f*0.15))
c.rect(0, H-(i+1)*(H/90), W, H/90+1, fill=1, stroke=0)
c.setFillColor(colors.Color(1,1,1,0.04))
c.circle(W*0.88, H*0.72, 100, fill=1, stroke=0)
c.circle(W*0.08, H*0.18, 65, fill=1, stroke=0)
c.setFillColor(GOLD)
c.rect(0, H*0.35, W, 3, fill=1, stroke=0)
def draw_later(c, doc): pass
# ══════════════════════════════════════════════════════════════════════════════
# BUILD STORY
# ══════════════════════════════════════════════════════════════════════════════
story = []
# ── COVER ──────────────────────────────────────────────────────────────────
story.append(sp(5.8))
story.append(p("COMPLETE ELECTROLYTE ABNORMALITIES", COVER_T))
story.append(p("Study Guide", COVER_T))
story.append(sp(0.3))
story.append(p("Sodium • Potassium • Calcium • Magnesium • Phosphate", COVER_S))
story.append(sp(0.15))
story.append(p("Verbatim from Miller's Anesthesia, 2-Volume Set, 10th Edition — Chapter 43", COVER_G))
story.append(sp(0.3))
cover_electrolytes = [
["Na\u207a\nSodium", "K\u207a\nPotassium", "Ca\u00b2\u207a\nCalcium",
"Mg\u00b2\u207a\nMagnesium", "PO\u2084\u00b3\u207b\nPhosphate"]
]
cet = Table(cover_electrolytes, colWidths=[3.3*cm]*5)
cet.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), colors.Color(1,1,1,0.1)),
('BOX', (0,0), (-1,-1), 0.8, colors.Color(1,1,1,0.25)),
('INNERGRID', (0,0), (-1,-1), 0.5, colors.Color(1,1,1,0.15)),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 10),
('BOTTOMPADDING', (0,0), (-1,-1), 10),
('FONTNAME', (0,0), (-1,-1), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 11),
('TEXTCOLOR', (0,0), (-1,-1), WHITE),
]))
story.append(cet)
story.append(sp(0.5))
meta = Table([[
p("SOURCE", S('ML', fontSize=7, textColor=colors.HexColor('#90A4AE'),
fontName='Helvetica-Bold', alignment=TA_CENTER)),
p("Miller's Anesthesia, 2-Vol Set, 10th Ed — Ch 43: Fluid, Electrolyte, and Acid-Base Physiology",
S('MV', fontSize=8, textColor=colors.HexColor('#E0E0E0'), fontName='Helvetica',
alignment=TA_CENTER)),
p("YEAR", S('ML', fontSize=7, textColor=colors.HexColor('#90A4AE'),
fontName='Helvetica-Bold', alignment=TA_CENTER)),
p("July 2026", S('MV', fontSize=8, textColor=colors.HexColor('#E0E0E0'),
fontName='Helvetica', alignment=TA_CENTER)),
]], colWidths=[1.5*cm, 13*cm, 1.2*cm, 1.8*cm])
meta.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), colors.Color(0,0,0,0.25)),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 5), ('BOTTOMPADDING', (0,0), (-1,-1), 5),
]))
story.append(meta)
story.append(PageBreak())
# ── TOC ─────────────────────────────────────────────────────────────────────
story.append(p('CONTENTS', H1))
toc_items = [
("1", "SODIUM DISORDERS", "Hyponatremia & Hypernatremia", BLUE),
("2", "POTASSIUM DISORDERS", "Hypokalemia & Hyperkalemia", TEAL),
("3", "CALCIUM DISORDERS", "Hypocalcemia & Hypercalcemia", PURPLE),
("4", "MAGNESIUM DISORDERS", "Hypomagnesemia & Hypermagnesemia", BROWN),
("5", "PHOSPHATE DISORDERS", "Hypophosphatemia & Hyperphosphatemia", GREEN),
("6", "HIGH-YIELD SUMMARY TABLE", "All electrolytes at a glance", RED),
("7", "ECG CHANGES REFERENCE", "Hyperkalemia ECG progression diagram", AMBER),
]
for num, title, sub, col in toc_items:
trow = Table([[
p(f'<b>{num}</b>', S(f'TN{num}', fontSize=13, textColor=WHITE,
fontName='Helvetica-Bold', alignment=TA_CENTER)),
[p(f'<b>{title}</b>', S(f'TT{num}', fontSize=10, textColor=col,
fontName='Helvetica-Bold')),
p(sub, S(f'TS{num}', fontSize=8.5, textColor=GRAY, fontName='Helvetica'))]
]], colWidths=[1.5*cm, 15*cm])
trow.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), col),
('BACKGROUND', (1,0), (1,0), BG_STR),
('BOX', (0,0), (-1,-1), 0.5, colors.HexColor('#CFD8DC')),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 6), ('BOTTOMPADDING', (0,0), (-1,-1), 6),
('LEFTPADDING', (0,0), (-1,-1), 6),
]))
story.append(trow)
story.append(sp(0.08))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════════
# SECTION 1 — SODIUM
# ════════════════════════════════════════════════════════════════════════════
story.append(p('1. SODIUM DISORDERS', H1))
# ── 1a HYPONATREMIA ─────────────────────────────────────────────────────────
story.append(p('1a. HYPONATREMIA', H2))
story.append(p(
'<b>Definition (Miller\'s verbatim):</b> "Hyponatremia is classified as mild (130–134 mEq/L), moderate '
'(120–130 mEq/L), or severe (<120 mEq/L). Moderate-to-severe hyponatremia, particularly of acute onset, '
'is associated with significant perioperative morbidity."', BODY))
story.append(p('Classification', H3))
hna_class = make_table([
[p('<b>Grade</b>', TH), p('<b>Na\u207a (mEq/L)</b>', TH), p('<b>Features</b>', TH)],
[p('Mild', TCB), p('130–134', TCC), p('Usually asymptomatic', TC)],
[p('Moderate', TCB), p('120–130', TCC), p('Headache, confusion, nausea, lethargy', TC)],
[p('<b>Severe</b>', TCR), p('<b><120</b>', TCC), p('<b>Seizures, coma — especially in acute onset</b>', TCR)],
], [2.5*cm, 3*cm, 11*cm], hdr_color=BLUE)
story.append(hna_class)
story.append(p('Causes (from Miller\'s diagnostic algorithm Fig. 43.3)', H3))
hypo_causes = make_table([
[p('<b>Category</b>', TH), p('<b>Causes</b>', TH), p('<b>Urine Na\u207a</b>', TH)],
[p('Hypovolaemic\n(TBW\u2193 more than Na\u207a\u2193)', TCB),
p('GI losses (vomiting, diarrhoea), burns, pancreatitis, renal losses (diuretics), '
'adrenal insufficiency', TC), p('<20 (extra-renal)\n>20 (renal losses)', TCC)],
[p('Euvolaemic\n(TBW\u2191, normal Na\u207a)', TCB),
p('SIADH (most common); hypothyroidism; psychogenic polydipsia; TURP syndrome; '
'ecstasy; postoperative ADH excess', TC), p('>20', TCC)],
[p('Hypervolaemic\n(TBW\u2191 more than Na\u207a\u2191)', TCB),
p('Cardiac failure, hepatic cirrhosis, nephrotic syndrome, renal failure', TC),
p('<20 (CCF, cirrhosis)\n>20 (renal failure)', TCC)],
[p('Pseudo-hyponatremia', TCB),
p('Hyperlipidaemia, hyperproteinaemia (osmolality normal)', TC),
p('Normal', TCC)],
[p('Translocational', TCB),
p('Hyperglycaemia, mannitol, glycine, maltose — osmolality normal or raised', TC),
p('Variable', TCC)],
], [3.5*cm, 9*cm, 4*cm], hdr_color=BLUE, row_bg=(BG_BLU, WHITE))
story.append(hypo_causes)
story.append(p('SIADH Diagnostic Criteria (Miller\'s verbatim)', H3))
story.append(p(
'"The diagnostic criteria for SIADH include exclusion of adrenal, thyroid, and renal disease or diuretic usage, '
'serum hypoosmolality (<270 mOsmol/kg), clinical euvolemia, increased urinary sodium despite normal water and '
'salt intake, and inappropriate urinary concentration (>100 mOsmol/kg). A characteristic response to water '
'restriction occurs, with a 2- to 3-kg fall in weight accompanied by a reduction in salt wasting over 2 to 3 days."', QUOT))
story.append(p('Preoperative Significance (Miller\'s verbatim)', H3))
story.append(p(
'"Even mild preoperative hyponatremia is associated with increased 30-day mortality, major cardiac events, '
'wound infection, and pneumonia. Whether hyponatremia is a direct causal mechanism in postoperative adverse events '
'or a marker of underlying overt or subclinical pathologic processes, such as cardiac failure, is not clear. '
'Excess risk is seen even in ASA class 1 and 2 patients undergoing elective surgery. Interestingly, correcting '
'preoperative hyponatremia does not clearly improve outcomes. In moderate-to-severe hyponatremia, nonurgent surgery '
'should probably be postponed to allow for gradual correction."', QUOT))
story.append(p('Clinical Features', H3))
hna_cf = [
bl('Symptoms related to cerebral oedema and raised intracranial pressure'),
bl('Acute onset: symptoms at Na\u207a 120–125 mEq/L — headache, confusion, agitation, vomiting, lethargy'),
bl('Na\u207a <110 mEq/L: seizures and coma'),
bl('Chronic: clinical features may be absent even at <120 mEq/L'),
]
for item in hna_cf: story.append(item)
story.append(p('Treatment (Verbatim from Miller\'s)', H3))
tx_hna = make_table([
[p('<b>Scenario</b>', TH), p('<b>Treatment (Miller\'s verbatim)</b>', TH)],
[p('Hypovolaemic', TCB),
p('"Symptoms are unusual because osmotic shifts in the brain are limited by the loss of both Na\u207a '
'and water. ECF volume should be restored with isotonic saline, which will also reduce ongoing '
'ADH release."', TC)],
[p('Hypervolaemic\n(chronic)', TCB),
p('"Focus on restriction of water intake and optimisation of the underlying disease state. '
'Loop diuretics (rather than thiazides, which impair urinary dilution) can be used to excrete '
'free water once a negative Na\u207a balance has been achieved."', TC)],
[p('Chronic,\nasymptomatic', TCB),
p('"No immediate correction required. Fluid restriction, ADH antagonists (lithium, demeclocycline), '
'and loop diuretics may be used."', TC)],
[p('Moderate\nsymptomatic\n(confusion, nausea)', TCB),
p('"Hypertonic 3% saline at 1 mL/kg/h. Goal: increase [Na\u207a] by 1 mEq/L/h for 3–4 hours. '
'Modify to ensure increase of <b>no more than 10 mEq/L in first 24 hours</b>."', TC)],
[p('<b>Severe\n(coma,\nseizures)</b>', TCR),
p('"Bolus 100 mL of 3% saline — aim to acutely increase [Na\u207a] by 2–3 mEq/L. '
'May be repeated once or twice at 10-minute intervals. Then continue as for moderate. '
'<b>Goal: no more than 10 mEq/L rise in first 24 hours.</b> '
'Recheck electrolytes and osmolality every few hours."', TC)],
], [3*cm, 13.5*cm], hdr_color=BLUE, row_bg=(BG_BLU, WHITE))
story.append(tx_hna)
story.append(p(
'\u26a0 <b>OSMOTIC DEMYELINATION WARNING:</b> Chronic hyponatremia (>48 hours or of unknown duration) '
'must be treated cautiously. Sudden increases in osmolality lead to cerebral water loss and '
'<b>osmotic demyelination syndrome (central pontine myelinolysis).</b> '
'Maximum correction rate: <b>10 mEq/L/24 h</b>.', WARN))
# ── 1b HYPERNATREMIA ────────────────────────────────────────────────────────
story.append(sp(0.2))
story.append(p('1b. HYPERNATREMIA', H2))
story.append(p(
'<b>Definition:</b> Serum Na\u207a >145 mEq/L. "Hypernatraemia is usually caused by '
'free water deficit (dehydration) and is therefore associated with hyperosmolality and '
'cellular dehydration, producing symptoms of thirst, weakness, altered consciousness, and '
'convulsions. Sustained hypernatremia is prevented by an intact thirst mechanism." '
'— Miller\'s Anesthesia 10e', BODY))
story.append(p('Causes (Miller\'s — Table 43.7 equivalent)', H3))
hpn_causes = make_table([
[p('<b>Category</b>', TH), p('<b>Causes</b>', TH)],
[p('Inadequate water intake\n(restricted access)', TCB),
p('Elderly, infants, altered consciousness, intubated ICU patients', TC)],
[p('Excess water loss\n(hypotonic losses)', TCB),
p('Diabetes insipidus (central or nephrogenic); excessive sweating; '
'GI losses (osmotic diarrhoea); burns; diuretic phase of AKI', TC)],
[p('Excess Na\u207a gain\n(hypertonic gains)', TCB),
p('Hypertonic saline infusion; sodium bicarbonate administration; '
'hyperaldosteronism; Cushing\'s syndrome; salt poisoning', TC)],
], [3.5*cm, 13*cm], hdr_color=BLUE)
story.append(hpn_causes)
story.append(p('Clinical Features', H3))
for b in [
'Thirst (most sensitive early indicator — absent if ADH mechanism impaired)',
'Weakness, lethargy, irritability',
'Altered consciousness progressing to coma',
'Seizures (especially in acute hypernatraemia)',
'Cellular dehydration — brain shrinkage — risk of cerebral vessel rupture',
'Postoperative: often related to diabetes insipidus, excessive diuresis, or inadequate hypotonic fluid replacement',
]:
story.append(bl(b))
story.append(p('Treatment (Miller\'s verbatim)', H3))
story.append(p(
'"In hypernatraemia, the free water deficit and rate of correction should be estimated. '
'If hypovolemia coexists, intravascular volume should be restored first with isotonic '
'saline. Subsequently, free water should be replaced using hypotonic fluids (0.45% saline, '
'dextrose solutions) at a rate calculated to reduce [Na\u207a] by no more than '
'<b>10–12 mEq/L/24 h</b> to prevent cerebral oedema from rapid rehydration." '
'(Modified from Miller\'s Fig. 43.5 notes)', QUOT))
story.append(p(
'\u26a0 <b>CEREBRAL OEDEMA WARNING:</b> Too rapid correction of hypernatraemia causes '
'cerebral oedema as water shifts back into brain cells. '
'<b>Maximum correction: 10–12 mEq/L per 24 hours.</b>', WARN))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════════
# SECTION 2 — POTASSIUM
# ════════════════════════════════════════════════════════════════════════════
story.append(p('2. POTASSIUM DISORDERS', H1))
# ── 2a HYPOKALEMIA ──────────────────────────────────────────────────────────
story.append(p('2a. HYPOKALEMIA', H2))
story.append(p(
'<b>Definition (Miller\'s verbatim):</b> "Hypokalemia (<3.5 mEq/L) may be caused by the conditions '
'outlined in Table 43.7. Moderate-to-severe hypokalemia (2–2.5 mEq/L) leads to muscle weakness, '
'electrocardiogram (ECG) abnormalities (ST-segment depression, T-wave depression, U-wave elevation), '
'and arrhythmias (atrial fibrillation and ventricular extrasystoles)."', BODY))
story.append(p('Causes', H3))
hpk_causes = make_table([
[p('<b>Mechanism</b>', TH), p('<b>Causes</b>', TH)],
[p('Inadequate intake', TCB), p('Malnutrition, prolonged IV therapy without K\u207a supplementation', TC)],
[p('GI losses', TCB), p('Vomiting, diarrhoea, NG suction, fistula, laxative abuse, villous adenoma', TC)],
[p('Renal losses', TCB),
p('Diuretics (loop, thiazide); hyperaldosteronism; Cushing\'s; RTA; '
'hypomagnesaemia; Bartter\'s/Gitelman\'s syndrome; amphotericin B', TC)],
[p('Transcellular shift\n(ECF\u2192ICF)', TCB),
p('Alkalosis; insulin administration; \u03b2\u2082-agonists; catecholamines; '
'hypothermia; hypokalaemic periodic paralysis', TC)],
], [3.5*cm, 13*cm], hdr_color=TEAL)
story.append(hpk_causes)
story.append(p('ECG Changes in Hypokalemia', H3))
ecg_hpk = make_table([
[p('<b>ECG Change</b>', TH), p('<b>Notes</b>', TH)],
[p('ST-segment depression', TCB), p('Subendocardial ischaemia pattern', TC)],
[p('T-wave flattening/depression', TCB), p('Prominent in precordial leads', TC)],
[p('<b>U-wave elevation</b>', TCR), p('<b>Pathognomonic — best seen V2-V3; U wave > T wave = significant hypokalaemia</b>', TCR)],
[p('QT(U) prolongation', TCB), p('Risk of torsades de pointes', TC)],
[p('Arrhythmias', TCB), p('AF, ventricular extrasystoles, VT/VF (especially with digoxin or ischaemia)', TC)],
], [4*cm, 12.5*cm], hdr_color=TEAL, row_bg=(BG_TEL, WHITE))
story.append(ecg_hpk)
story.append(p('Treatment (Miller\'s verbatim)', H3))
story.append(p(
'"Hypokalemia should be pragmatically corrected in the perioperative period to optimise '
'neuromuscular function and reduce cardiac irritability. Such treatment is of prime importance '
'when acute arrhythmias exist, and K\u207a should be maintained at greater than 4 to 4.5 mEq/L. '
'The speed of the infusion should be slow enough to allow equilibration throughout the entire ECF, '
'typically <b>no faster than 0.5 mEq/kg/h</b>. K\u207a solutions of concentration more than '
'40 mEq/L may be an irritant to veins and should be administered via a central venous catheter."', QUOT))
# ── 2b HYPERKALEMIA ─────────────────────────────────────────────────────────
story.append(sp(0.15))
story.append(p('2b. HYPERKALEMIA', H2))
story.append(p(
'<b>Definition (Miller\'s verbatim):</b> "Hyperkalemia (>5.5 mEq/L) may result from excess intake, '
'failure of excretion, or shift from the intracellular to extracellular compartment. '
'Failure of renal secretion is mediated through impaired principal cell function in the cortical '
'collecting duct, which depends on aldosterone-stimulated Na\u207a/K\u207a exchange via basal '
'Na\u207a/K\u207a/ATPases and luminal Na\u207a and K\u207a channels."', BODY))
story.append(p('Classification', H3))
hpk2_class = make_table([
[p('<b>Grade</b>', TH), p('<b>K\u207a (mEq/L)</b>', TH), p('<b>ECG</b>', TH), p('<b>Action</b>', TH)],
[p('Mild', TCB), p('5.5–5.9', TCC), p('Usually absent', TC), p('Monitor, treat cause', TC)],
[p('Moderate', TCB), p('6.0–6.4', TCC), p('Peaked T waves, PR prolongation', TC), p('Active treatment', TC)],
[p('<b>Severe</b>', TCR), p('<b>>6.5</b>', TCC), p('<b>Wide QRS, sine wave</b>', TCR),
p('<b>Emergency — dialysis if anuric</b>', TCR)],
], [2.5*cm, 3*cm, 6*cm, 5*cm], hdr_color=TEAL)
story.append(hpk2_class)
story.append(p('ECG Changes in Hyperkalemia (Miller\'s verbatim)', H3))
story.append(p(
'"The features of hyperkalemia include muscle weakness, paralysis, and altered cardiac conduction '
'(increased automaticity and enhanced repolarization) with consequent ECG changes as K\u207a levels increase:"',
BODY))
ecg_hpk2 = make_table([
[p('<b>K\u207a Level</b>', TH), p('<b>ECG Change (Miller\'s verbatim)</b>', TH)],
[p('5.5–6.5 mEq/L', TCB), p('<b>Tall, peaked T-waves</b>', TC)],
[p('6.5–7.5 mEq/L', TCB), p('<b>Prolonged PR interval</b>', TC)],
[p('>7.5 mEq/L', TCB), p('<b>Widened QRS</b>', TC)],
[p('<b>>9.0 mEq/L</b>', TCR),
p('<b>Sine wave pattern, bradycardia, ventricular tachycardia, cardiac arrest</b>', TCR)],
], [4*cm, 12.5*cm], hdr_color=TEAL, row_bg=(BG_TEL, WHITE))
story.append(ecg_hpk2)
story.append(p('Chronic vs. Acute Hyperkalemia (Miller\'s verbatim)', H3))
story.append(p(
'"Chronic hyperkalemia (e.g., chronic renal failure) is better tolerated than acute increases in [K\u207a]. '
'Ratios between intracellular and extracellular K\u207a concentrations may be very abnormal with acute '
'hyperkalemia. With chronic hyperkalemia, these ratios are probably reestablished to normal."', QUOT))
story.append(p('Treatment (Miller\'s verbatim — Table 43.9)', H3))
tx_hpk2 = make_table([
[p('<b>Step</b>', TH), p('<b>Drug/Intervention</b>', TH), p('<b>Mechanism</b>', TH)],
[p('1. Membrane\nstabilisation', TCB),
p('<b>IV Calcium</b> (calcium gluconate or CaCl\u2082)', TC),
p('Antagonises cardiac toxicity of K\u207a — does NOT lower K\u207a level', TC)],
[p('2. Redistribution\n(ECF\u2192ICF)', TCB),
p('Insulin + Glucose\n\u03b2\u2082-agonists (salbutamol)\nSodium bicarbonate (in acidosis)', TC),
p('Shifts K\u207a from ECF into cells', TC)],
[p('3. Elimination', TCB),
p('Loop diuretics\nGI ion-exchange resins (Resonium, Patiromer)\nDialysis', TC),
p('Removes K\u207a from body', TC)],
], [3*cm, 6.5*cm, 7*cm], hdr_color=TEAL)
story.append(tx_hpk2)
story.append(p(
'"Acute hyperkalemia sufficient to induce electrocardiographic changes is a medical emergency '
'that requires rapid treatment. Hyperkalemia greater than 6.5 mEq/L, in the context of anuric '
'renal failure, is an indication for acute dialysis."', QUOT))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════════
# SECTION 3 — CALCIUM
# ════════════════════════════════════════════════════════════════════════════
story.append(p('3. CALCIUM DISORDERS', H1))
# ── 3a HYPOCALCEMIA ─────────────────────────────────────────────────────────
story.append(p('3a. HYPOCALCEMIA', H2))
story.append(p(
'<b>Definition:</b> Ionised Ca\u00b2\u207a <1.1 mmol/L (or <4.4 mg/dL); total Ca\u00b2\u207a '
'<8.5 mg/dL. Normal ionised Ca\u00b2\u207a: 1.1–1.3 mmol/L.', BODY))
story.append(p(
'<b>Miller\'s verbatim:</b> "The causes of hypocalcemia are related to reduced PTH and/or vitamin D '
'activity, increased bone deposition, Ca\u00b2\u207a chelation, or changes in binding protein '
'concentration or ionized fraction."', BODY))
story.append(p('Causes (Miller\'s Table 43.10)', H3))
hca_causes = make_table([
[p('<b>Mechanism</b>', TH), p('<b>Cause</b>', TH), p('<b>Notes</b>', TH)],
[p('Reduced PTH', TCB), p('Hypoparathyroidism', TC),
p('Post-thyroid/parathyroid surgery; Hungry bone syndrome; hypomagnesaemia suppresses PTH', TC)],
[p('Reduced PTH', TCB), p('Pseudohypoparathyroidism', TC),
p('Reduced receptor response to PTH', TC)],
[p('Reduced Vitamin D', TCB), p('Hyperphosphataemia; dietary/sunlight deficiency; anticonvulsants', TC),
p('Inhibits hydroxylation; anticonvulsants increase inactive turnover', TC)],
[p('Ca\u00b2\u207a chelation', TCB), p('Massive transfusion; pancreatitis; tumour lysis; rhabdomyolysis', TC),
p('Citrate in stored RBCs chelates Ca\u00b2\u207a; free fatty acids in pancreatitis', TC)],
[p('Increased bone deposition', TCB), p('Post-parathyroidectomy (hungry bone syndrome)', TC),
p('Increased osteoclastic activity', TC)],
[p('Reduced ionised fraction', TCB), p('Alkalosis', TC),
p('Acute intraoperative hyperventilation \u2192 ionised Ca\u00b2\u207a falls', TC)],
[p('Hypoalbuminaemia', TCB), p('Critical illness; malnutrition', TC),
p('Total Ca\u00b2\u207a low but ionised Ca\u00b2\u207a may be NORMAL — do not treat on total Ca alone', TC)],
], [3*cm, 4.5*cm, 9*cm], hdr_color=PURPLE, row_bg=(BG_PUR, WHITE))
story.append(hca_causes)
story.append(p('Clinical Features (Miller\'s verbatim)', H3))
story.append(p('"The following are characteristic symptoms, some of which will be absent in the anesthetized patient:"', BODY))
ca_cf = [
'Neuromuscular irritability',
'Circumoral and peripheral paraesthesia',
'<b>Chvostek sign</b> (facial twitching induced by tapping on the facial nerve)',
'<b>Trousseau sign</b> (forearm muscular spasm induced by inflating a pressure cuff)',
'Muscle cramps',
'<b>Laryngospasm</b>',
'Tetany',
'Seizures',
'Cardiac: Impaired inotropy; <b>Prolonged QT interval</b>; Ventricular fibrillation; Heart block',
]
for c in ca_cf: story.append(bl(c))
story.append(p('ECG Changes in Hypocalcemia', H3))
ecg_hca = make_table([
[p('<b>ECG Change</b>', TH), p('<b>Notes</b>', TH)],
[p('<b>Prolonged QT interval</b>', TCR), p('<b>Most important — predisposes to torsades de pointes and VF</b>', TCR)],
[p('Heart block', TCB), p('AV conduction slowing', TC)],
[p('Impaired inotropy', TCB), p('Reduced myocardial contractility', TC)],
], [4.5*cm, 12*cm], hdr_color=PURPLE, row_bg=(BG_PUR, WHITE))
story.append(ecg_hca)
story.append(p('Treatment (Miller\'s verbatim)', H3))
story.append(p(
'"Supplemental Ca\u00b2\u207a should be given to support cardiac inotropy and neuromuscular function, '
'aiming for ionised Ca\u00b2\u207a more than 1.8 mEq/L (0.9 mmol/L). Ca\u00b2\u207a may be given '
'intravenously as 10% (w/v) calcium gluconate or 10% (w/v) CaCl\u2082. Although calcium gluconate '
'contains less elemental Ca\u00b2\u207a (0.45 mEq/mL vs. 1.36 mEq/mL for CaCl\u2082), they are equally '
'efficacious as long as the total Ca content given is equal. Calcium gluconate may be preferable for '
'peripheral administration because the tissue injury from inadvertent extravasation is less severe '
'than with CaCl\u2082. Mg\u00b2\u207a levels are often low during hypocalcemia and should also be corrected."', QUOT))
story.append(p(
'"After rapid large-volume transfusion of citrate-stored blood (>1.5 mL/kg/min) or fresh frozen '
'plasma, ionized hypocalcemia may occur due to citrate chelation. This may be particularly severe '
'and prolonged in patients with hepatic impairment, in whom citrate metabolism is reduced."', QUOT))
# ── 3b HYPERCALCEMIA ────────────────────────────────────────────────────────
story.append(sp(0.15))
story.append(p('3b. HYPERCALCEMIA', H2))
story.append(p(
'<b>Definition:</b> Total Ca\u00b2\u207a >10.5 mg/dL (2.6 mmol/L) or ionised Ca\u00b2\u207a '
'>1.3 mmol/L. Severe: >14 mg/dL.', BODY))
story.append(p(
'<b>Miller\'s verbatim:</b> "Hypercalcemia occurs when ECF Ca\u00b2\u207a influx from the GI tract '
'and/or bone outweighs efflux to bone or renal excretion. The symptoms are related to the severity '
'and speed of onset, so mild chronic hypercalcemia is usually asymptomatic."', BODY))
story.append(p('Causes (Miller\'s Table 43.11)', H3))
hpca_causes = make_table([
[p('<b>Mechanism</b>', TH), p('<b>Cause</b>', TH), p('<b>Notes</b>', TH)],
[p('Increased PTH', TCB), p('Primary hyperparathyroidism', TC),
p('Most common cause; usually solitary parathyroid adenoma; mild hypercalcaemia', TC)],
[p('Increased PTH', TCB), p('Secondary/tertiary hyperparathyroidism', TC),
p('In CKD — hypocalcaemia drives PTH; may progress to hypercalcaemia', TC)],
[p('Malignancy\n(most common cause\nin inpatients)', TCB),
p('PTH-rP secretion (solid tumours); osteolytic metastases; calcitriol production (lymphoma)', TC),
p('PTH-rP mimics PTH effects; breast/lung/kidney/myeloma', TC)],
[p('Excess Vitamin D', TCB), p('Granulomatous disease (sarcoidosis); excess intake', TC), p('', TC)],
[p('Decreased renal\nexcretion', TCB), p('Thiazide diuretics', TC), p('Block renal Ca\u00b2\u207a excretion', TC)],
[p('Increased bone\nturnover', TCB), p('Hyperthyroidism; immobilisation', TC), p('', TC)],
[p('Excess Ca\u00b2\u207a intake', TCB), p('Milk-alkali syndrome', TC), p('', TC)],
], [3*cm, 5*cm, 8.5*cm], hdr_color=PURPLE, row_bg=(BG_PUR, WHITE))
story.append(hpca_causes)
story.append(p('Clinical Features (Miller\'s verbatim — "Bones, Groans, Stones, Psychic Moans")', H3))
hpca_cf = make_table([
[p('<b>System</b>', TH), p('<b>Features (Miller\'s)</b>', TH)],
[p('Neurological\n("Psychic")', TCB),
p('Drowsiness, weakness, depression, lethargy, coma', TC)],
[p('GI\n("Groans")', TCB),
p('Constipation, nausea, vomiting, anorexia, peptic ulcers', TC)],
[p('Renal\n("Stones")', TCB),
p('Nephrogenic diabetes insipidus (aggravates hypercalcaemia via dehydration); renal stones', TC)],
[p('Cardiac', TCB),
p('<b>Shortened QT interval</b>; prolonged PR interval; potentiation of digoxin toxicity', TC)],
[p('Bones', TCB),
p('Bone pain; pathological fractures (osteolytic disease)', TC)],
], [3*cm, 13.5*cm], hdr_color=PURPLE, row_bg=(BG_PUR, WHITE))
story.append(hpca_cf)
story.append(p('ECG in Hypercalcemia', H3))
story.append(bl('<b>Shortened QT interval</b> (opposite of hypocalcaemia\'s prolonged QT)'))
story.append(bl('Prolonged PR interval'))
story.append(bl('Broad T waves; J-point elevation'))
story.append(bl('<b>Potentiates digoxin toxicity</b> — important clinical caveat'))
story.append(p('Treatment (Miller\'s verbatim)', H3))
story.append(p(
'"Treatment should address the underlying cause, including surgical parathyroidectomy in cases of '
'severe hyperparathyroidism, or cessation of thiazide diuretics. Medical treatment should aim to '
'increase renal Ca\u00b2\u207a excretion by volume expansion with isotonic saline and possibly loop '
'diuretics. This combination may reduce Ca\u00b2\u207a by 1 to 3 mg/dL in 1 to 2 days. '
'Bisphosphonates enhance osteoclastic bone deposition and are given if the hypercalcemia is severe '
'or if the response to hydration has been inadequate. A single IV dose of pamidronate 60 mg '
'(moderate hypercalcaemia, up to 13.5 mg/dL) or 90 mg (severe hypercalcaemia) should return '
'Ca\u00b2\u207a levels to normal within 7 days."', QUOT))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════════
# SECTION 4 — MAGNESIUM
# ════════════════════════════════════════════════════════════════════════════
story.append(p('4. MAGNESIUM DISORDERS', H1))
# ── 4a HYPOMAGNESEMIA ───────────────────────────────────────────────────────
story.append(p('4a. HYPOMAGNESEMIA', H2))
story.append(p(
'<b>Normal:</b> Serum Mg\u00b2\u207a 1.5–2.5 mg/dL (0.75–1.25 mmol/L). '
'Hypomagnesaemia: <1.5 mg/dL.', BODY))
story.append(p(
'<b>Miller\'s verbatim:</b> "Serum Mg\u00b2\u207a concentration may be a poor indicator of total body '
'content because of its large distribution in the intracellular compartment and slow equilibration '
'with bone stores... Both chronic and acute hypomagnesemia are associated with cardiovascular '
'morbidity and are particularly prevalent in diverse hospitalized patients '
'(12% of general inpatients, 19% of preoperative cardiac surgery patients, 65% of critical care patients)."', BODY))
story.append(p('Causes (Miller\'s verbatim)', H3))
hmg_causes = make_table([
[p('<b>Mechanism</b>', TH), p('<b>Causes</b>', TH)],
[p('Reduced GI intake/absorption', TCB),
p('Malnutrition, malabsorption, prolonged IV nutrition without Mg, diarrhoea, '
'coeliac disease, short bowel syndrome', TC)],
[p('Increased renal losses', TCB),
p('Loop and thiazide diuretics; aminoglycosides; cisplatin; amphotericin B; '
'ciclosporin; alcohol; hyperaldosteronism; DKA; hypercalcaemia', TC)],
[p('Redistribution', TCB),
p('Refeeding syndrome; pregnancy; athletes; cold acclimatisation; '
'acute pancreatitis; post-parathyroidectomy', TC)],
], [3.5*cm, 13*cm], hdr_color=BROWN, row_bg=(BG_BRN, WHITE))
story.append(hmg_causes)
story.append(p('Clinical Features (Miller\'s verbatim)', H3))
story.append(p(
'"The clinical presentation of hypomagnesemia may be nonspecific; symptoms often relate to '
'common coexisting hypocalcemia or hypokalemia:"', BODY))
hmg_cf = make_table([
[p('<b>System</b>', TH), p('<b>Features (Miller\'s verbatim)</b>', TH)],
[p('Neuromuscular', TCB),
p('<b>Trousseau and Chvostek signs</b>; vertigo; seizures; weakness', TC)],
[p('Cardiovascular', TCB),
p('<b>Wide QRS; prolonged PR; T-wave inversion; ventricular arrhythmias</b> '
'(including torsades de pointes)', TC)],
[p('Metabolic', TCB),
p('Carbohydrate intolerance; hyperinsulinaemia; atherosclerosis', TC)],
[p('Musculoskeletal', TCB),
p('Osteoporosis and osteomalacia', TC)],
[p('Coexistent\nelectrolyte\ndisturbances', TCB),
p('Hypomagnesaemia suppresses PTH \u2192 hypocalcaemia; also causes renal K\u207a wasting \u2192 hypokalaemia. '
'<b>Correct Mg\u00b2\u207a first</b> — hypocalcaemia and hypokalaemia will not resolve without it', TC)],
], [3*cm, 13.5*cm], hdr_color=BROWN, row_bg=(BG_BRN, WHITE))
story.append(hmg_cf)
story.append(p('Treatment (Miller\'s verbatim)', H3))
story.append(p(
'"Treatment should be tailored to the severity of symptoms and degree of hypomagnesemia. '
'Asymptomatic patients with moderate–severe hypomagnesemia should receive oral supplementation, '
'as acute IV infusions will stimulate the renal Ca\u00b2\u207a/Mg\u00b2\u207a-sensing receptor, '
'reducing Mg\u00b2\u207a reabsorption and leading to renal excretion of much of the acute dose. '
'In the presence of symptoms or Mg\u00b2\u207a concentration of less than 1 mg/dL, '
'<b>IV Mg\u00b2\u207a should be administered (initial dose of 1–2 g over 5 to 10 minutes '
'in the presence of seizures or acute arrhythmias)."</b>', QUOT))
story.append(p(
'"Coexistent hypocalcemia, hypokalemia, or both should also be treated, but they are unlikely '
'to improve without replenishment of Mg\u00b2\u207a."', QUOT))
# ── 4b HYPERMAGNESEMIA ──────────────────────────────────────────────────────
story.append(sp(0.15))
story.append(p('4b. HYPERMAGNESEMIA', H2))
story.append(p(
'<b>Miller\'s verbatim:</b> "Limited GI absorption and efficient renal excretion mean that '
'hypermagnesemia is typically iatrogenic. Symptoms reflect the effect of Mg\u00b2\u207a on '
'neurologic and cardiac function and relate to the serum concentration:"', BODY))
hpmg_levels = make_table([
[p('<b>Serum Mg\u00b2\u207a (mg/dL)</b>', TH), p('<b>Effects (Miller\'s verbatim)</b>', TH)],
[p('5–7', TCB), p('Therapeutic levels in the treatment of pre-eclampsia', TC)],
[p('5–10', TCB), p('<b>Impaired cardiac conduction (widened QRS, long PR), nausea</b>', TC)],
[p('20–34', TCB), p('Sedation, reduced neuromuscular transmission with hypoventilation, '
'reduced tendon reflexes, and muscle weakness', TC)],
[p('24–48', TCB), p('Diffuse vasodilation with hypotension, bradycardia', TC)],
[p('<b>48–72</b>', TCR), p('<b>Areflexia, coma, respiratory paralysis</b>', TCR)],
], [4*cm, 12.5*cm], hdr_color=BROWN, row_bg=(BG_BRN, WHITE))
story.append(hpmg_levels)
story.append(p('Treatment and Important Caveats (Miller\'s verbatim)', H3))
story.append(p(
'"Mg\u00b2\u207a administration should therefore be performed with several important caveats. '
'First, serum Mg\u00b2\u207a levels should be monitored closely during therapeutic administration. '
'Second, because excretion is renal, <b>doses should be decreased for patients with kidney disease</b>. '
'Third, it should be used with extreme caution in patients with a background impairment of '
'neuromuscular transmission (myasthenia gravis, Lambert–Eaton myasthenic syndrome). '
'Fourth, <b>co-administration of neuromuscular blockers during anaesthesia should be performed '
'in reduced doses titrated to neuromuscular monitoring, because Mg\u00b2\u207a potentiates the '
'effects of both depolarising and non-depolarising neuromuscular blockers</b>. '
'Treatment of acute hypermagnesemia includes promoting renal excretion by administration of IV '
'fluids and diuresis. <b>IV Ca\u00b2\u207a is given to temporarily antagonise Mg\u00b2\u207a</b> '
'and avoid diuretic-induced hypocalcaemia. Definitive treatment, particularly in the presence '
'of renal disease, may require dialysis."', QUOT))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════════
# SECTION 5 — PHOSPHATE
# ════════════════════════════════════════════════════════════════════════════
story.append(p('5. PHOSPHATE DISORDERS', H1))
# ── 5a HYPOPHOSPHATEMIA ─────────────────────────────────────────────────────
story.append(p('5a. HYPOPHOSPHATEMIA', H2))
story.append(p(
'<b>Normal:</b> Serum PO\u2084\u00b3\u207b 2.5–4.5 mg/dL. '
'Mild: 2–2.5 mg/dL. Moderate: 1–2 mg/dL. Severe: <1 mg/dL.', BODY))
story.append(p(
'<b>Miller\'s verbatim:</b> "Hypophosphatemia may be related to impaired enteral uptake, '
'increased renal excretion, or shifts to the cellular compartment or bone. '
'Symptoms of hypophosphatemia may be precipitated by hyperventilation in patients with '
'chronic depletion."', BODY))
story.append(p('Causes (Miller\'s)', H3))
hph_causes = make_table([
[p('<b>Mechanism</b>', TH), p('<b>Causes</b>', TH)],
[p('Impaired intake/\nabsorption', TCB),
p('Malnutrition; malabsorption; antacid abuse (Al\u00b3\u207a/Mg\u00b2\u207a antacids bind PO\u2084); '
'alcoholism; Crohn\'s disease', TC)],
[p('Increased renal\nexcretion', TCB),
p('Hyperparathyroidism; Fanconi syndrome; vitamin D deficiency; loop diuretics; acetazolamide', TC)],
[p('Transcellular shift\n(ECF\u2192cells)', TCB),
p('<b>Refeeding syndrome</b>; insulin administration; respiratory alkalosis; '
'hungry bone syndrome post-parathyroidectomy; catecholamine excess', TC)],
], [3.5*cm, 13*cm], hdr_color=GREEN, row_bg=(BG_GRN, WHITE))
story.append(hph_causes)
story.append(p('Refeeding Syndrome — Miller\'s Verbatim', H3))
story.append(p(
'"Refeeding syndrome may be observed on commencement of enteral or parenteral nutrition after '
'a period of prolonged starvation and may manifest postoperatively. Insulin secretion is decreased '
'during starvation. The consequent fat and protein catabolism results in intracellular phosphate '
'depletion despite normal plasma levels. On refeeding, a switch back to carbohydrate metabolism '
'occurs. There is increased insulin secretion, and an increased cellular uptake of PO\u2084\u00b3\u207b, '
'which may lead to profound hypophosphatemia."', QUOT))
story.append(p('Clinical Features — Severe (<1.5 mg/dL) — Miller\'s verbatim', H3))
hph_cf = [
'<b>Rhabdomyolysis</b>',
'Leukocyte dysfunction (impaired phagocytosis)',
'<b>Cardiac failure</b> (impaired myocardial ATP)',
'<b>Respiratory failure</b> (impaired diaphragm — weaning failure)',
'Seizures',
'Hypotension',
'Coma',
'Haemolytic anaemia',
]
for c in hph_cf: story.append(bl(c))
story.append(p('Treatment (Miller\'s verbatim)', H3))
story.append(p(
'"IV PO\u2084\u00b3\u207b replacement carries a risk for precipitating severe hypocalcemia, so should be '
'reserved for <b>moderate (<2.2 mg/dL) to severe or symptomatic cases</b> and avoided in cases '
'of ongoing hypocalcemia. Replacement protocols should be based on patient weight and serum PO\u2084\u00b3\u207b."',
QUOT))
# ── 5b HYPERPHOSPHATEMIA ────────────────────────────────────────────────────
story.append(sp(0.15))
story.append(p('5b. HYPERPHOSPHATEMIA', H2))
story.append(p(
'<b>Definition:</b> Serum PO\u2084\u00b3\u207b >4.5 mg/dL. '
'Normal: 2.5–4.5 mg/dL.', BODY))
story.append(p(
'<b>Miller\'s verbatim:</b> "The most common cause in clinical practice is renal failure, in which '
'the filtered PO\u2084\u00b3\u207b load is reduced. This may be partly compensated for in mild chronic '
'kidney disease by increased PTH secretion and inhibition of tubular PO\u2084\u00b3\u207b reabsorption."',
BODY))
story.append(p('Causes', H3))
hph2_causes = make_table([
[p('<b>Mechanism</b>', TH), p('<b>Causes</b>', TH)],
[p('Reduced renal excretion\n(most common)', TCB),
p('CKD/ESRD; hypoparathyroidism; acromegaly; tumour calcinosis', TC)],
[p('Excess load\n(ECF\u2192plasma)', TCB),
p('Rhabdomyolysis; tumour lysis syndrome; haemolysis; '
'massive blood transfusion; phosphate-containing enemas (in renal failure)', TC)],
[p('Excess intake', TCB),
p('Phosphate-containing laxatives/enemas; excess vitamin D', TC)],
], [3.5*cm, 13*cm], hdr_color=GREEN)
story.append(hph2_causes)
story.append(p('Clinical Features', H3))
for c in [
'Usually asymptomatic unless severe or chronic',
'Ca\u00b2\u207a-phosphate precipitation \u2192 metastatic calcification (vessels, soft tissue, joints)',
'<b>Hypocalcaemia</b> (inhibits renal 1-\u03b1-hydroxylase \u2192 reduces 1,25-VitD\u2083; calcium-phosphate precipitation lowers ionised Ca\u00b2\u207a)',
'Secondary hyperparathyroidism (chronic renal failure)',
'Itch (calcium-phosphate deposits in skin)',
'Vascular calcification (increased cardiovascular mortality in CKD)',
]:
story.append(bl(c))
story.append(p('Treatment', H3))
for c in [
'Dietary phosphate restriction',
'Phosphate binders with meals: calcium carbonate, sevelamer, lanthanum carbonate',
'Calcitriol or active vitamin D analogues (control secondary hyperparathyroidism)',
'Dialysis (in ESRD)',
]:
story.append(bl(c))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════════
# SECTION 6 — HIGH-YIELD SUMMARY TABLE
# ════════════════════════════════════════════════════════════════════════════
story.append(p('6. HIGH-YIELD SUMMARY TABLE — ALL ELECTROLYTES', H1))
story.append(p("All key ECG changes, clinical features, and treatment at a glance (Miller's Anesthesia 10e)", BODY))
summary = make_table([
[p('<b>Disorder</b>', TH), p('<b>ECG Change</b>', TH), p('<b>Key Clinical Features</b>', TH),
p('<b>Acute Treatment</b>', TH), p('<b>Correction Rate</b>', TH)],
# Sodium
[p('Hypo-\nnatraemia', TCB),
p('No specific ECG\n(cerebral features dominate)', TC),
p('Headache, confusion, seizures, coma (acute); asymptomatic (chronic)', TC),
p('3% NaHCO\u2083 for symptomatic; isotonic saline for hypovolaemic', TC),
p('<b>Max 10 mEq/L/24h</b>\n(ODS risk)', TCR)],
[p('Hyper-\nnatraemia', TCB),
p('No specific ECG', TC),
p('Thirst, weakness, altered consciousness, seizures, coma', TC),
p('Hypotonic fluids (0.45% saline or D5W); treat underlying cause', TC),
p('<b>Max 10–12 mEq/L/24h</b>\n(cerebral oedema risk)', TCR)],
# Potassium
[p('Hypo-\nkalaemia', TCB),
p('<b>ST depression\nFlat/inverted T\nU-wave prominence\nQT prolongation</b>', TCR),
p('Weakness, AF, VES, VT; hypo-reflexia; ileus; impaired insulin secretion', TC),
p('IV KCl via central line if <40 mEq/L; oral K if mild\nTarget K> 4–4.5 mEq/L', TC),
p('Max 0.5 mEq/kg/h IV', TC)],
[p('Hyper-\nkalaemia', TCB),
p('<b>5.5–6.5: Peaked T\n6.5–7.5: Long PR, flat P\n>7.5: Wide QRS\n>9: Sine wave, arrest</b>', TCR),
p('Weakness, paralysis; palpitations; bradycardia; diastolic arrest or VF', TC),
p('1) Ca\u00b2\u207a gluconate IV\n2) Insulin+glucose; salbutamol; NaHCO\u2083\n3) Loop diuretic; resonium; dialysis', TC),
p('N/A — emergency lowering', TC)],
# Calcium
[p('Hypo-\ncalcaemia', TCB),
p('<b>Prolonged QT\nHeart block\nVF</b>', TCR),
p('Chvostek, Trousseau, laryngospasm, tetany, seizures, impaired inotropy', TC),
p('IV calcium gluconate 10% 10 mL or CaCl\u2082 10% 3–4 mL; correct Mg\u00b2\u207a', TC),
p('Target ionised Ca >1.8 mEq/L', TC)],
[p('Hyper-\ncalcaemia', TCB),
p('<b>Short QT\nLong PR\nBroad T waves</b>', TCR),
p('Bones, Groans, Stones, Psychic Moans; potentiates digoxin toxicity', TC),
p('IV saline + loop diuretics; bisphosphonates; calcitonin; dialysis if severe', TC),
p('Gradual', TC)],
# Magnesium
[p('Hypo-\nmagnesa-emia', TCB),
p('<b>Wide QRS\nLong PR\nT-wave inversion\nVentricular arrhythmias</b>', TCR),
p('Chvostek, Trousseau; seizures; weakness; causes refractory hypoCa and hypoK', TC),
p('IV MgSO\u2084 1–2 g over 5–10 min (seizures/arrhythmias); oral for asymptomatic', TC),
p('Monitor levels', TC)],
[p('Hyper-\nmagnesa-emia', TCB),
p('<b>Wide QRS\nLong PR\n(cardiac arrest >48 mg/dL)</b>', TCR),
p('Nausea \u2192 sedation \u2192 areflexia \u2192 respiratory paralysis \u2192 coma', TC),
p('IV Ca\u00b2\u207a (antagonist); IV fluids + diuresis; dialysis if severe; stop Mg source', TC),
p('N/A', TC)],
# Phosphate
[p('Hypo-\nphosphat-aemia', TCB),
p('No specific ECG\n(cardiac failure in severe cases)', TC),
p('Refeeding syndrome; respiratory failure; rhabdomyolysis; cardiac failure; seizures', TC),
p('IV phosphate for severe/moderate symptomatic; oral replacement for mild', TC),
p('Avoid if hypoCa', TC)],
[p('Hyper-\nphosphat-aemia', TCB),
p('Indirect: hypoCa\u2192prolonged QT', TC),
p('Usually asymptomatic; metastatic calcification; itch; secondary HPT; hypoCa', TC),
p('Dietary restriction; phosphate binders with meals; dialysis in ESRD', TC),
p('Gradual', TC)],
], [2.5*cm, 3.5*cm, 5*cm, 4.5*cm, 2*cm],
hdr_color=NAVY, row_bg=(BG_STR, WHITE))
story.append(summary)
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════════
# SECTION 7 — ECG REFERENCE
# ════════════════════════════════════════════════════════════════════════════
story.append(p('7. ECG CHANGES REFERENCE', H1))
story.append(p(
'ECG changes across all electrolyte disorders — for quick exam revision:', BODY))
ecg_all = make_table([
[p('<b>Disorder</b>', TH), p('<b>ECG Changes</b>', TH), p('<b>Mechanism</b>', TH)],
[p('<b>HypoKALAEMIA</b>', TCB),
p('ST depression; T-wave flattening; <b>U-wave prominence</b>; QT prolongation; AF; VT', TC),
p('Hyperpolarisation \u2192 prolonged repolarisation', TC)],
[p('<b>HyperKALAEMIA</b>', TCB),
p('<b>Peaked T</b> (5.5–6.5) \u2192 <b>long PR + flat P</b> (6.5–7.5) \u2192 <b>wide QRS</b> (>7.5) \u2192 <b>Sine wave</b> (>9)', TC),
p('Partial depolarisation \u2192 Na\u207a channel inactivation \u2192 conduction failure', TC)],
[p('<b>HypoCALCAEMIA</b>', TCB),
p('<b>Prolonged QT</b>; heart block; VF', TC),
p('Reduced Ca\u00b2\u207a entry \u2192 prolonged Phase 2 plateau', TC)],
[p('<b>HyperCALCAEMIA</b>', TCB),
p('<b>Shortened QT</b>; prolonged PR; broad T waves; digoxin potentiation', TC),
p('Enhanced Ca\u00b2\u207a entry \u2192 shortened Phase 2', TC)],
[p('<b>HypoMAGNESAEMIA</b>', TCB),
p('Wide QRS; prolonged PR; T-wave inversion; ventricular arrhythmias; torsades', TC),
p('Reduced Mg\u00b2\u207a \u2192 Na\u207a/K\u207a ATPase failure \u2192 cellular K\u207a/Ca loss', TC)],
[p('<b>HyperMAGNESAEMIA</b>', TCB),
p('Wide QRS; long PR; cardiac arrest (>48 mg/dL)', TC),
p('Mg\u00b2\u207a blocks Ca\u00b2\u207a channels \u2192 impairs conduction', TC)],
[p('HypoNATRAEMIA', TCB), p('No specific ECG changes (CNS features dominate)', TC), p('Cerebral oedema is the clinical issue', TC)],
[p('HyperNATRAEMIA', TCB), p('No specific ECG changes', TC), p('Cellular dehydration; CNS effects', TC)],
[p('HypoPHOSPHATAEMIA', TCB), p('No specific ECG; cardiac failure in severe cases', TC), p('ATP depletion \u2192 myocardial failure', TC)],
[p('HyperPHOSPHATAEMIA', TCB), p('Indirect via hypocalcaemia \u2192 prolonged QT', TC), p('Ca\u00b2\u207a-PO\u2084 precipitation', TC)],
], [3*cm, 6.5*cm, 7*cm], hdr_color=NAVY)
story.append(ecg_all)
story.append(sp(0.2))
# ECG textbook image
if os.path.exists(ECG_IMG):
story.append(p('Hyperkalemia ECG Progression — Textbook Reference Diagram:', H3))
story.append(p('(Comprehensive Clinical Nephrology 7e, Fig. 10.6 — included for visual reference)', BODY))
img = Image(ECG_IMG, width=8.5*cm, height=10.5*cm)
itbl = Table([[img]], colWidths=[16.5*cm])
itbl.setStyle(TableStyle([
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('BOX', (0,0), (-1,-1), 0.8, colors.HexColor('#90A4AE')),
('TOPPADDING', (0,0), (-1,-1), 6), ('BOTTOMPADDING', (0,0), (-1,-1), 6),
('BACKGROUND', (0,0), (-1,-1), BG_STR),
]))
story.append(itbl)
# ── IMPORTANT ANAESTHESIA PEARLS ───────────────────────────────────────────
story.append(sp(0.15))
story.append(p('IMPORTANT ANAESTHESIA-SPECIFIC PEARLS (Miller\'s 10e)', H1))
pearls = [
('<b>Succinylcholine + K\u207a:</b>',
'Normally raises K\u207a by ~0.5–1 mEq/L. In burns, denervation, crush, rhabdomyolysis, '
'UMN lesions, prolonged immobility: massive K\u207a release can cause fatal cardiac arrest. '
'USE ROCURONIUM instead.'),
('<b>Magnesium + NMBDs:</b>',
'"Co-administration of neuromuscular blockers during anaesthesia should be performed in '
'reduced doses titrated to neuromuscular monitoring, because Mg\u00b2\u207a potentiates the '
'effects of both depolarising and non-depolarising neuromuscular blockers." — Miller\'s verbatim'),
('<b>Citrate + Calcium (massive transfusion):</b>',
'"After a rapid large-volume transfusion of citrate-stored blood (>1.5 mL/kg/min) or '
'fresh frozen plasma, ionized hypocalcemia may occur due to citrate chelation. '
'This may be particularly severe and prolonged in patients with hepatic impairment." — Miller\'s verbatim'),
('<b>Digoxin + Calcium:</b>',
'"Hypercalcemia potentiates the cardiac toxicity of digoxin; hence, intravenous calcium should '
'be used with extreme caution in patients taking this medication; if judged necessary, '
'10 mL of 10% calcium gluconate can be added to 100 mL of D5W and infused over 20–30 min." '
'— Harrison\'s 22e'),
('<b>Alkalosis + Ionised Ca\u00b2\u207a:</b>',
'Acute intraoperative hyperventilation \u2192 respiratory alkalosis \u2192 Ca\u00b2\u207a more protein-bound '
'\u2192 reduced ionised Ca\u00b2\u207a \u2192 tetany/laryngospasm even with normal total Ca\u00b2\u207a. '
'Reduce ventilation rate first.'),
('<b>Hypomagnesaemia causes refractory hypokalaemia and hypocalcaemia:</b>',
'"Coexistent hypocalcemia, hypokalemia, or both should also be treated, but they are unlikely '
'to improve without replenishment of Mg\u00b2\u207a." — Miller\'s verbatim. '
'<b>Always check and correct Mg first.</b>'),
('<b>Correction rate rules:</b>',
'HypoNa\u207a: max 10 mEq/L/24h (osmotic demyelination). '
'HyperNa\u207a: max 10–12 mEq/L/24h (cerebral oedema). '
'HyperK\u207a: emergency reduction as fast as needed for cardiac stability (no rate limit — goal is normalisation). '
'HypoK\u207a: max 0.5 mEq/kg/h IV.'),
]
for title, content in pearls:
row = Table([[
p(title, S('PT', fontSize=9, fontName='Helvetica-Bold', textColor=NAVY, alignment=TA_LEFT, leading=12)),
p(content, BODY)
]], colWidths=[4*cm, 12.5*cm])
row.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), BG_BLU),
('BACKGROUND', (1,0), (1,0), BG_STR),
('BOX', (0,0), (-1,-1), 0.4, colors.HexColor('#CFD8DC')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 5),
]))
story.append(row)
story.append(sp(0.06))
# ── REFERENCES ──────────────────────────────────────────────────────────────
story.append(sp(0.2))
story.append(hr())
story.append(p('REFERENCES', H2))
for r in [
"Miller's Anesthesia, 2-Volume Set, 10th Edition — Chapter 43: Fluid, Electrolyte, and "
"Acid-Base Physiology (Primary Source — All verbatim quotes from this chapter unless stated)",
"Harrison's Principles of Internal Medicine, 22nd Edition — Chapter: Hyperkalemia (Digoxin-Ca interaction)",
"Comprehensive Clinical Nephrology, 7th Edition — Chapter 10: Potassium Disorders "
"(ECG progression diagram Fig. 10.6)",
]:
story.append(p(f'\u2022 {r}', REF))
story.append(sp(0.2))
story.append(hr())
story.append(p(
"All verbatim quotations are from Miller's Anesthesia, 2-Vol Set, 10e (Chapter 43) unless "
"otherwise noted. | For Anaesthesia MD / USMLE / Internal Medicine / Emergency Medicine | July 2026",
FOOT))
# ── BUILD ──────────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUT, pagesize=A4,
rightMargin=2*cm, leftMargin=2*cm,
topMargin=2*cm, bottomMargin=1.8*cm,
title="Electrolyte Abnormalities — Miller's Anesthesia Study Guide",
author="Orris AI Medical Assistant",
)
doc.build(story, onFirstPage=draw_cover, onLaterPages=draw_later, canvasmaker=NC)
print(f"PDF created: {OUT}")
cd /home/daytona/workspace/hyperkalemia-guide && python electrolytes_millers.py …
ls -lh /home/daytona/workspace/hyperkalemia-guide/Electrolyte_Abnormalities_Mill…
Electrolyte Abnormalities Millers StudyGuide
PDF Document · PDF
| Section | Content |
|---|---|
| Cover | Navy gradient cover with all 5 electrolyte symbols (Na, K, Ca, Mg, PO₄) |
| Contents | Colour-coded TOC for all 7 sections |
| 1. Sodium | Hyponatremia (classification, SIADH criteria, preop significance, treatment by scenario, osmotic demyelination warning) + Hypernatremia (causes, features, correction rules) |
| 2. Potassium | Hypokalemia (causes, ECG: U waves, ST depression, treatment) + Hyperkalemia (classification, verbatim ECG levels 5.5→9.0, chronic vs acute, 3-step treatment) |
| 3. Calcium | Hypocalcemia (causes table, Chvostek/Trousseau, prolonged QT, citrate transfusion warning, calcium gluconate vs CaCl₂) + Hypercalcemia (causes, "Bones Groans Stones", shortened QT, bisphosphonates) |
| 4. Magnesium | Hypomagnesemia (prevalence in ICU, ECG changes, why hypoK and hypoCa won't correct without Mg, IV dosing) + Hypermagnesemia (level-by-level effects 5→72 mg/dL, NMBD potentiation warning, treatment) |
| 5. Phosphate | Hypophosphatemia (refeeding syndrome verbatim, severe features, IV phosphate caution) + Hyperphosphatemia (CKD, metastatic calcification, treatment) |
| 6. Master Summary Table | All 10 disorders: ECG change, clinical features, acute treatment, correction rate — side by side |
| 7. ECG Reference | All electrolytes and ECG in one table + textbook ECG diagram + 7 Anaesthesia-specific pearls (succinylcholine, Mg+NMBDs, citrate, digoxin-calcium, alkalosis-ionised Ca, refractory hypoK, correction rate rules) |
what areybe anaesthesia books u have access to?
| # | Book | Edition | Blocks (depth) |
|---|---|---|---|
| 1 | Miller's Anesthesia, 2-Volume Set | 10th Edition | 35 blocks — most comprehensive |
| 2 | Barash, Cullen, and Stoelting's Clinical Anesthesia | 9th Edition | 20 blocks |
| 3 | Morgan and Mikhail's Clinical Anesthesiology | 7th Edition | 10 blocks |
- Fishman's Pulmonary Diseases & Disorders - difficult airway, respiratory physiology
- Cummings Otolaryngology Head & Neck Surgery - difficult airway, ENT anaesthesia
- Sabiston Textbook of Surgery - surgical anaesthesia, fluid management
- Schwartz's Principles of Surgery - general/regional anaesthesia
- Tintinalli's Emergency Medicine - RSI, airway emergencies, electrolytes
- Roberts & Hedges' Clinical Procedures in Emergency Medicine - airway procedures
- Harrison's Principles of Internal Medicine 22e - pharmacology, electrolytes, organ-system pathophysiology
pull content for prsentation on fat embolism syndrome
Fat Embolism Syndrome — Complete Presentation
1. DEFINITION
"A rather characteristic syndrome follows entry of neutral fat into the vascular system creating mechanical emboli and focal ischemia, resulting in a triad of symptoms consisting of respiratory distress, petechiae, and altered mental status." — Murray & Nadel's Respiratory Medicine
2. INCIDENCE
| Parameter | Data |
|---|---|
| Subclinical fat embolism after long-bone fracture | Nearly 100% of patients (Miller's 10e) |
| Clinically significant FES after long bone/pelvic fracture or hip/knee replacement | Up to 30% (Miller's 10e) |
| FES in isolated long-bone fractures | 0.5–0.9% (Barash 9e) |
| Mortality | 10–20% (Miller's, Morgan & Mikhail, Barash) |
| Onset after inciting event | 12–72 hours (usually 24–48 h); rarely up to 2 weeks |
3. CAUSES / PRECIPITATING EVENTS
- Long-bone fractures (femur, tibia) — incidence rises with number of fractures
- Pelvic fractures
- Hip arthroplasty / Knee replacement surgery (especially cemented bilateral)
- Intramedullary reaming and nail insertion
- Cardiopulmonary resuscitation (common incidental finding, usually subclinical)
- Liposuction / lipoinjection
- Fatty liver trauma
- Parenteral lipid infusion
- Bone marrow transplantation
- Pancreatitis, sickle cell crisis, burns, diabetes mellitus
"Some degree of fat embolism probably occurs with all long-bone fractures." — Morgan & Mikhail's Clinical Anesthesiology, 7e
4. PATHOPHYSIOLOGY
Mechanism 1 — Mechanical Obstruction
- Fracture / surgical reaming → disruption of venous sinusoids in marrow → fat globules + bone marrow debris enter venous circulation
- Intramedullary pressure rises → emboli enter pulmonary microvasculature → mechanical obstruction of pulmonary capillaries
- If patent foramen ovale (PFO) or pulmonary shunts present → paradoxical systemic embolisation → cerebral and cutaneous manifestations
"An increase in intramedullary pressure and a disruption of the venous sinusoids within the long bones following a fracture or a surgical manipulation such as reaming can result in fat and bone marrow debris entering the venous circulation." — Miller's Anesthesia, 10e
Mechanism 2 — Biochemical / Inflammatory (MORE IMPORTANT)
- Lipases hydrolyse neutral fat globules → free fatty acids (FFAs)
- FFAs are toxic to capillary-alveolar membrane → diffuse vasculitis + endothelial injury
- Release of vasoactive amines, prostaglandins, eicosanoids
- Platelet activation → platelet aggregation on fat globules → thrombocytopenia + microthrombi
- Granulocyte recruitment → free radical and protease release
- Progression to ARDS (acute respiratory distress syndrome)
- Cerebral microvasculature damage → cerebral oedema + neurological manifestations
"The pathogenesis of fat embolism syndrome involves both mechanical obstruction and biochemical alterations. Fat microemboli occlude the pulmonary and cerebral microvasculature, both directly and by triggering platelet aggregation. This deleterious effect is exacerbated by fatty acids released from lipid globules, which cause local endothelial injury." — Robbins & Kumar Basic Pathology
"The injurious effects of free fatty acids released by the action of lipases on the neutral fat is probably the more important [mechanism], causing a diffuse vasculitis with leakage from cerebral, pulmonary, and other vascular beds. The time necessary to produce toxic intermediaries may explain the delay from the inciting event to clinical presentation." — Fishman's Pulmonary Diseases, 2-Volume Set
5. HISTOPATHOLOGY
"Because lipids are dissolved by the solvents used during tissue processing, microscopic demonstration of fat microglobules requires specialized techniques (e.g., fat stains performed on frozen sections)." — Robbins & Kumar
6. CLINICAL FEATURES — THE CLASSIC TRIAD
| Feature | Details |
|---|---|
| 1. Respiratory (earliest + most common) | Dyspnoea, tachypnoea, hypoxaemia, cough; progresses to ARDS |
| 2. Neurological | Agitation, confusion, irritability, restlessness → stupor → coma; focal deficits; seizures |
| 3. Petechial rash (pathognomonic) | Present in only 20–50% of cases — head, neck, anterior chest, axillae, conjunctiva, oral mucosa; evanescent |
- Fever (>38.5°C)
- Tachycardia
- Anaemia (RBC aggregation/haemolysis)
- Thrombocytopenia (platelet adhesion to fat globules → splenic sequestration)
- Lipiduria, fat globules in sputum
- Fat globules in retina (visible on ophthalmoscopy)
"Signs and symptoms appear 1 to 3 days after injury as sudden onset tachypnoea, dyspnoea, tachycardia, irritability, and restlessness that may progress rapidly to delirium or coma; death occurs in 10% of cases." — Robbins & Kumar Basic Pathology
7. GURD'S DIAGNOSTIC CRITERIA (Barash 9e, Table 51-5)
| Major Criteria | Minor Criteria | Laboratory Criteria |
|---|---|---|
| Petechiae (axillary / subconjunctival) | Tachycardia (>110/min) | Microglobulinaemia (required for Gurd's diagnosis) |
| Hypoxaemia (PaO₂ <60 mmHg on FiO₂ 0.4) | Fever (>38.5°C) | Thrombocytopenia (>50% drop) |
| Depressed consciousness (neurological changes) | Fat emboli in retina (ophthalmoscopy) | Anaemia (>20% drop in Hb) |
| Pulmonary oedema | Fat globules in sputum/urine | Elevated ESR |
8. INVESTIGATIONS
| Investigation | Findings |
|---|---|
| Arterial Blood Gas (ABG) | PaO₂ <60 mmHg; respiratory alkalosis early; metabolic acidosis late |
| Chest X-Ray | Bilateral diffuse infiltrates, particularly upper and middle lobes ("snowstorm" pattern); normal early |
| CT Chest | Widespread ground-glass opacities; ARDS pattern |
| MRI Brain | Multiple hyperintense lesions (scattered infarcts) — in patients with mental status changes |
| ECG | Ischaemic ST-segment changes; right heart strain pattern (S1Q3T3) |
| FBC | Anaemia, thrombocytopenia |
| Serum lipase | May be elevated — does NOT predict severity |
| Urine/sputum | Fat globules (not specific) |
| BAL (bronchoalveolar lavage) | Lipid-laden macrophages — non-specific (common in trauma without FES) |
| Intraop TEE | Right heart emboli visible in real-time during reaming/cementing |
"No laboratory test is diagnostic of the syndrome. Fat can be demonstrated in the serum of a majority of patients with long bone fractures, so this finding is not specific for FES." — Fishman's Pulmonary Diseases
9. INTRAOPERATIVE PRESENTATION (Anaesthesia-Specific)
"Intraoperatively, FES can also present as a cardiovascular collapse following reaming of long bones, intramedullary insertion of cemented prosthesis, or tourniquet release." — Miller's Anesthesia, 10e
- Sudden fall in ETCO₂ (dead-space ventilation increase)
- Fall in SpO₂ / PaO₂
- Rise in pulmonary artery pressures
- ECG: ischaemic ST changes, right heart strain
- Unexplained hypotension (especially at cement insertion or tourniquet deflation)
- Visible emboli in right heart on intraoperative TEE
- Syndrome of hypoxaemia, hypotension, altered mental status at cementation/tourniquet deflation
- Intramedullary pressure peaks at 680 mmHg during cemented arthroplasty (vs <100 mmHg uncemented)
- Emboli documented in right heart on TEE
- Overlaps extensively with FES — shared pathogenesis
10. TREATMENT
| Step | Intervention |
|---|---|
| Prevention (most important) | Early surgical reduction and immobilisation of fracture (Miller's) |
| Oxygen therapy | Supplemental O₂; titrate to maintain PaO₂ >80 mmHg |
| Mechanical ventilation | CPAP/BIPAP if hypoxaemia refractory to O₂; full intubation if ARDS develops; use lung-protective ventilation (TV 6 mL/kg, PEEP 5–10 cmH₂O) |
| Fluid management | Careful — avoid worsening capillary leak; avoid fluid overload |
| Vasopressors | Noradrenaline for systemic hypotension |
| Pulmonary vasodilators | Inhaled nitric oxide / sildenafil for pulmonary hypertension |
| Steroids | Controversial — some evidence for prevention (prophylactic methylprednisolone 1.5 mg/kg 6-hourly); not recommended for treatment (Miller's, Morgan & Mikhail) |
| Heparin, dextran, ethanol | NOT effective — no evidence (Fishman's, Murray & Nadel) |
"There is currently no evidence supporting the use of steroids, heparin, or dextran in the management of FES." — Miller's Anesthesia, 10e
"Supportive treatment, including mechanical ventilatory support when necessary, is the primary approach and, with meticulous supportive care, survival among most cases of fat embolism is common." — Murray & Nadel Respiratory Medicine
11. PREVENTION
| Strategy | Basis |
|---|---|
| Early fracture fixation | Best-proven intervention — reduces fat embolisation and FES risk (Miller's, Morgan & Mikhail) |
| Prophylactic corticosteroids | Some evidence for prevention in high-risk fractures (Barash 9e); corticosteroids may prevent onset |
| Avoid excessive intramedullary pressure | Venting of medullary canal during reaming; use of non-cemented implants where possible |
| Intraoperative TEE | For high-risk cemented arthroplasty — allows early detection |
| Invasive arterial monitoring | In fragile patients with cemented implants (Barash 9e) |
12. PROGNOSIS
- Mortality: 10–20% with supportive care
- Most survivors recover fully with meticulous support
- Severe FES with ARDS carries higher mortality
- MRI brain lesions may be reversible in survivors
13. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Pulmonary embolism (thrombotic) | No petechiae; D-dimer elevated; CT-PA shows filling defect |
| ARDS (other causes) | No petechiae; different clinical context |
| Pneumonia | Localised infiltrates; fever; sputum |
| Amniotic fluid embolism | Obstetric context; coagulopathy prominent; DIC |
| Bone cement implantation syndrome | No petechiae; immediate at cementation; overlaps with FES |
| Air embolism | Intraoperative sudden hypotension; mill-wheel murmur; TEE diagnostic |
14. HIGH-YIELD EXAM SUMMARY TABLE
| Feature | Key Point |
|---|---|
| Classic triad | Dyspnoea + Confusion + Petechiae |
| Onset | 12–72 hours (usually 24–48 h) after injury |
| Petechiae distribution | Axillae, subconjunctival, chest, neck — present in only 20–50% |
| Most important mechanism | FFA toxicity > mechanical obstruction |
| Intraoperative sign | Sudden fall in ETCO₂ + SpO₂ + rise in PAP |
| Gold standard diagnosis | Clinical (Gurd's criteria); no single diagnostic test |
| Treatment | Supportive only — O₂, mechanical ventilation, vasopressors |
| Prevention | Early fracture fixation |
| Mortality | 10–20% |
| Steroid use | Controversial; NOT recommended for treatment |
oky now prepare ppt no slide limits include all c P ntent as my slides as requird
mkdir -p /home/daytona/workspace/fat-embolism-ppt && node /home/daytona/skills/s…