Thyroid gland
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Thyroid gland for physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive, textbook-sourced physiology content. Let me compile the full detailed answer.
Thyroid Gland - Physiology
Sources: Costanzo Physiology 7e, Ganong's Review of Medical Physiology 26e, Guyton & Hall Textbook of Medical Physiology
1. Overview
The thyroid gland secretes two active hormones - triiodothyronine (T3) and tetraiodothyronine/thyroxine (T4) - that affect virtually every organ system. It also secretes calcitonin from parafollicular (C) cells, important in calcium regulation. Thyroid disorders (deficiency and excess) are among the most common endocrinopathies, affecting 4-5% of the US population and more where iodine deficiency is prevalent. - Costanzo Physiology, p. 422
2. Hormones of the Thyroid Gland
The two active thyroid hormones differ by only a single iodine atom:
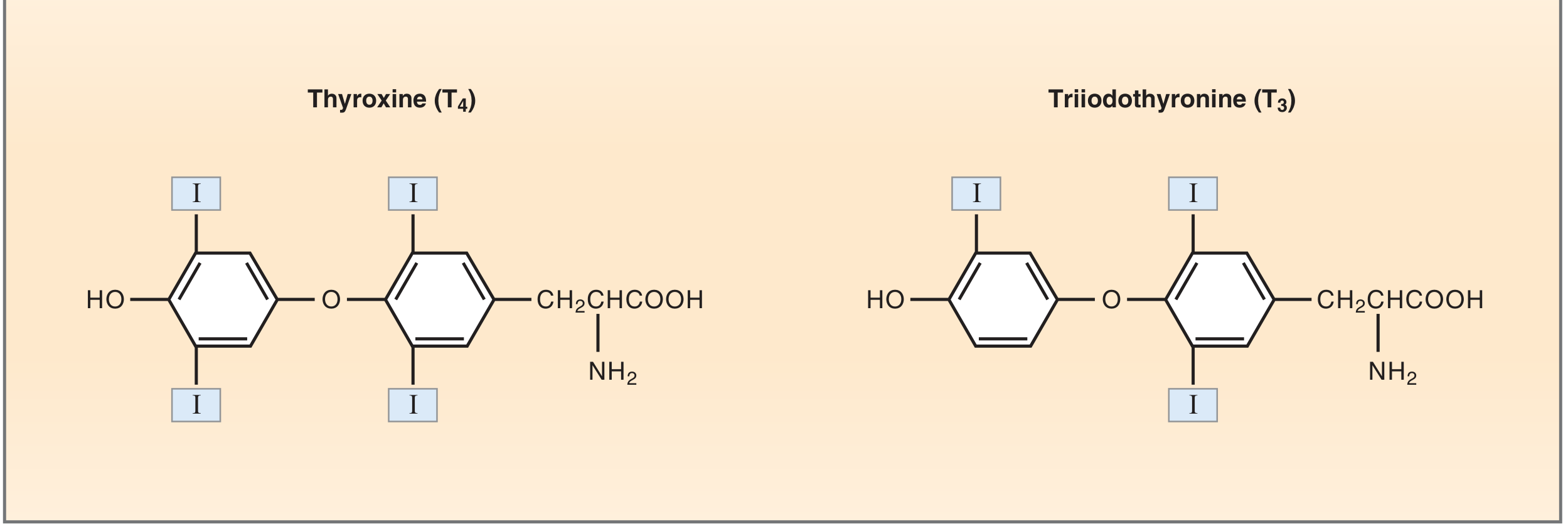
| Feature | T4 | T3 |
|---|---|---|
| Iodine atoms | 4 | 3 |
| % of thyroid output | ~90% | ~10% |
| Biological activity | Less active (prohormone) | 10x more active |
| Plasma half-life | ~7 days | ~1 day |
A third compound, reverse T3 (rT3), is formed from T4 but has no biological activity. - Costanzo Physiology, p. 423
3. Thyroid Follicle Structure
The functional unit is the thyroid follicle - a spherical structure 200-300 µm in diameter lined by follicular epithelial cells (thyrocytes), surrounding a central lumen filled with colloid.
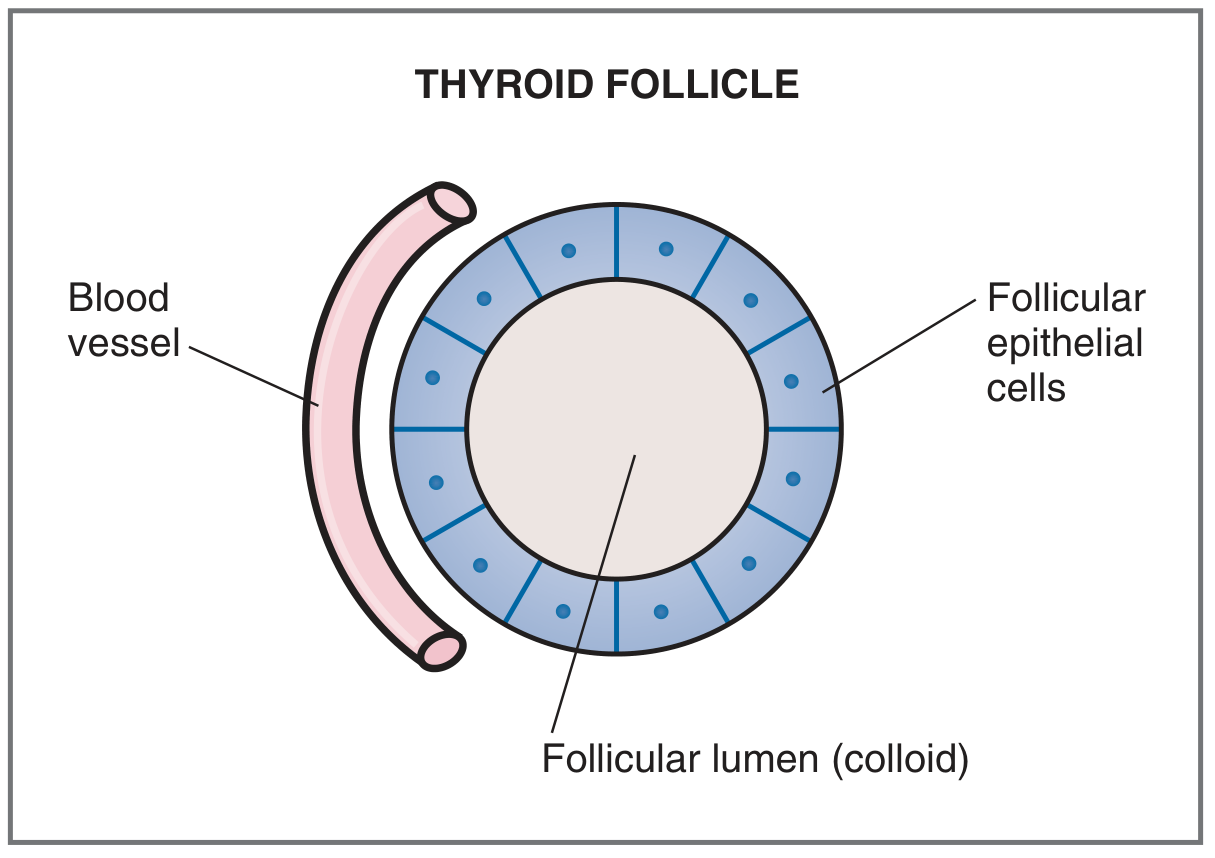
Key points about the follicle:
- The colloid consists primarily of thyroglobulin (TG), a large glycoprotein (~335 kDa, ~70 tyrosine residues) that is the precursor and storage form of thyroid hormones
- The thyroid is the only endocrine gland that stores its hormones in large extracellular quantities - enough supply for up to 2-3 months without new synthesis
- The gland has an exceptionally rich blood supply (~5x gland weight per minute) - Guyton & Hall, p. 930
4. Thyroid Hormone Synthesis
Synthesis is unique - it occurs partly intracellularly and partly extracellularly, involving three unusual features: (1) large amounts of iodine required, (2) storage outside the cell in the follicular lumen, (3) hormones are synthesized attached to a large protein (thyroglobulin). - Costanzo Physiology, p. 423
Step-by-Step Process
Step 1 - Iodide Trapping (Active Transport)
- Dietary iodide is absorbed from the GI tract and circulates in blood
- The sodium-iodide symporter (NIS) on the basolateral membrane co-transports 1 I⁻ with 2 Na⁺ into the thyrocyte (driven by Na⁺-K⁺ ATPase gradient)
- This concentrates iodide ~30x the blood level normally; up to 250x when maximally stimulated
- TSH is the most important regulator of NIS activity
- Iodide then exits across the apical membrane via pendrin (chloride-iodide counter-transporter) into the follicular lumen - Guyton & Hall, p. 930
Step 2 - Thyroglobulin Synthesis and Secretion
- Thyrocytes synthesize thyroglobulin in the RER and Golgi
- Thyroglobulin is secreted by exocytosis into the follicular lumen (an "exocrine" phase)
- Thyroglobulin contains ~70-140 tyrosine residues, but only 4-8 are normally incorporated into thyroid hormones - Ganong's, p. 370
Step 3 - Organification of Iodide
- At the apical membrane, thyroid peroxidase (TPO) oxidizes iodide (I⁻ → I⁰ or I₃⁻) using H₂O₂
- Oxidized iodine rapidly incorporates into tyrosine residues on thyroglobulin within the colloid
- This process is called "organification"
Step 4 - Iodotyrosine Coupling
- Monoiodotyrosine (MIT): Tyrosine + 1 iodine atom (position 3)
- Diiodotyrosine (DIT): Tyrosine + 2 iodine atoms (positions 3 and 5)
- T4 (Thyroxine): DIT + DIT coupling (TPO-mediated oxidative condensation)
- T3: MIT + DIT coupling
- rT3: DIT + MIT (but outer ring iodination)
- Ganong's, p. 370 and Guyton & Hall, p. 931
Step 5 - Storage
- Thyroid hormones remain covalently attached to thyroglobulin in the colloid as a large hormone reservoir
Step 6 - Secretion (Endocrine Phase)
- When stimulated (by TSH), thyrocytes endocytose colloid containing thyroglobulin
- Lysosomes fuse with the endocytic vesicles; lysosomal proteases hydrolyze the peptide bonds
- Free T4 and T3 are released into the cytosol and then into capillaries
- MIT and DIT are deiodinated within the cell; iodine is recycled
- Ganong's, p. 370
5. Transport in Blood
Once released, thyroid hormones are highly protein-bound in plasma:
| Binding Protein | Binds |
|---|---|
| Thyroxine-binding globulin (TBG) | ~70% of T4; primary carrier |
| Transthyretin (prealbumin) | ~10-15% |
| Albumin | ~15-20% |
- Only the free (unbound) fraction is biologically active (~0.03% of T4; ~0.3% of T3)
- Total plasma levels can change with binding protein levels (e.g., high TBG in pregnancy increases total T4 but free T4 remains normal - patient is euthyroid)
- Ganong's, p. 372-373
6. Peripheral Metabolism: T4 → T3 Conversion
T4 is essentially a prohormone. Most biological activity comes from T3 produced in peripheral tissues.
Three deiodinase enzymes (all contain the rare amino acid selenocysteine):
| Enzyme | Location | Action |
|---|---|---|
| D1 | Liver, kidney, thyroid, pituitary | Converts T4 → T3 (maintains peripheral T3) |
| D2 | Brain, pituitary, brown fat | Converts T4 → T3 (local supply) |
| D3 | Brain, reproductive tissues | Converts T4/T3 → rT3 (inactivation) |
Quantitative breakdown in a normal adult:
- 87% of circulating T3 comes from peripheral T4 deiodination (only 13% directly secreted by the thyroid)
- 95% of circulating rT3 comes from peripheral deiodination
- Ganong's, p. 371
Conditions that shift conversion toward rT3 (↓ T3):
Pregnancy, fasting, physiologic stress, hepatic/renal failure, β-blocker use
Conditions that increase T4 → T3 conversion:
Obesity
7. Regulation of Secretion - The HPT Axis
The hypothalamic-pituitary-thyroid (HPT) axis regulates thyroid hormone secretion via classic negative feedback:
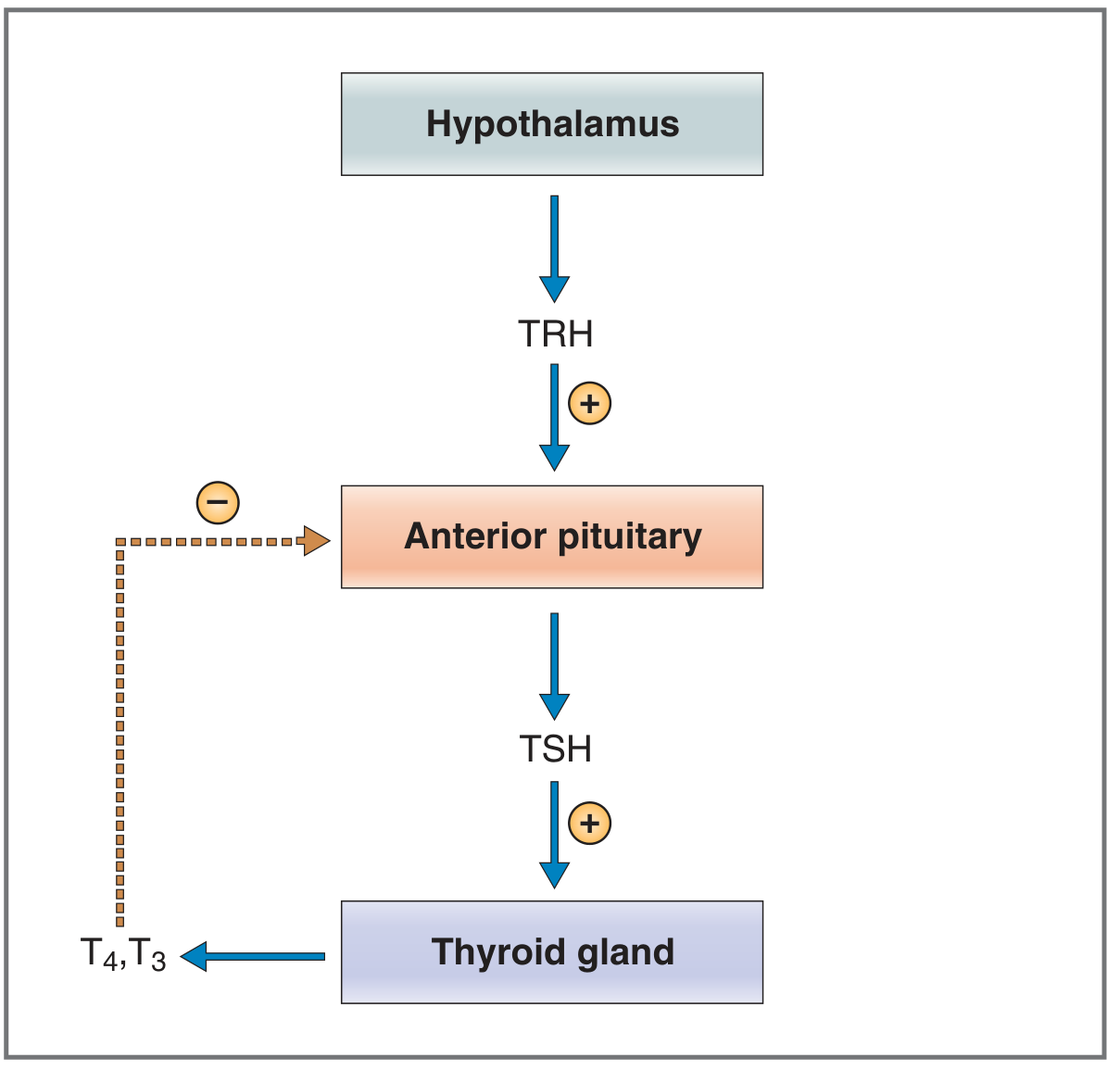
TRH (Thyrotropin-Releasing Hormone)
- Tripeptide secreted by paraventricular nuclei of the hypothalamus
- Stimulates thyrotrophs of anterior pituitary to secrete TSH
- Also stimulates prolactin secretion
TSH (Thyroid-Stimulating Hormone)
- Glycoprotein; secreted by anterior pituitary thyrotrophs
- Actions on thyroid: stimulates NIS (iodide trapping), thyroglobulin synthesis, organification, endocytosis of colloid, and thyroid cell growth (trophic)
- Binds TSH receptor (GPCR) → activates Gs → ↑ cAMP → protein kinase A pathway
- Higher TSH concentrations also activate G-PLC pathway
Negative Feedback
- Free T3 (converted from T4 in anterior pituitary by local D2 deiodinase) down-regulates TRH receptors on thyrotrophs
- Reduces sensitivity to TRH stimulation → decreases TSH secretion
- This reciprocal system maintains a steady-state of thyroid hormone output
Additional inhibitors of TSH/TRH signaling:
- Somatostatin (inhibits TRH action)
- Dopamine
- High-dose glucocorticoids
- Costanzo Physiology, p. 426 and Ganong's, p. 373
Factors affecting thyroid hormone secretion (summary):
| Stimulatory | Inhibitory |
|---|---|
| TSH | Iodine deficiency |
| Thyroid-stimulating immunoglobulins (TSI/Graves') | Wolff-Chaikoff effect (excess I⁻) |
| Increased TBG (pregnancy) | Perchlorate, thiocyanate (block NIS) |
| Propylthiouracil/Methimazole (block TPO) | |
| Decreased TBG (liver disease) |
8. Mechanism of Action at Target Cells
T3 is the active intracellular mediator. The mechanism is genomic:
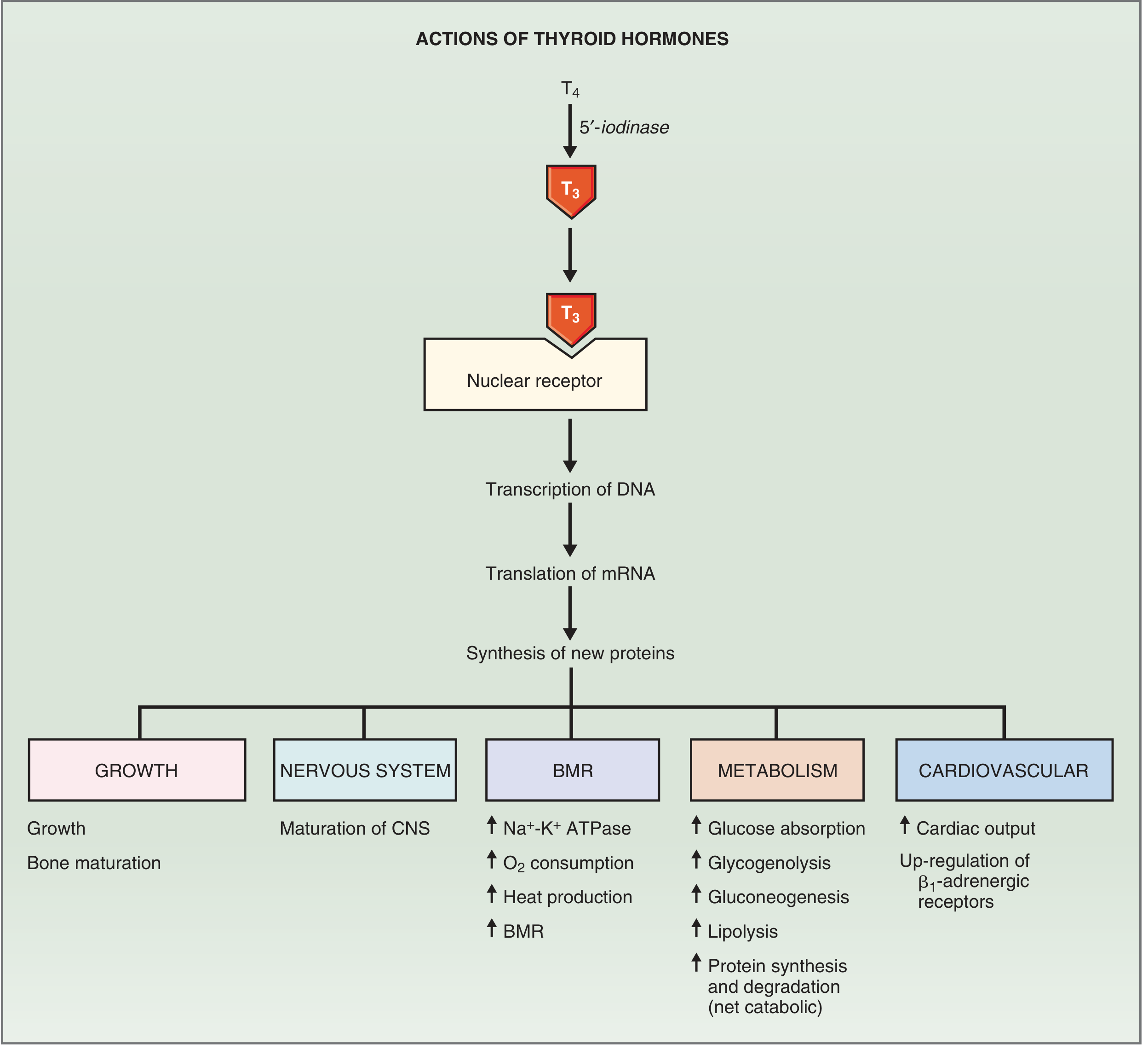
- T4 enters target cell and is converted to T3 by 5'-deiodinase (D1 or D2)
- T3 enters the nucleus and binds to a thyroid hormone nuclear receptor (TR-alpha or TR-beta)
- The T3-receptor complex binds to thyroid hormone response elements (TREs) on DNA (often as a heterodimer with RXR - retinoid X receptor)
- Stimulates transcription → new mRNAs → new protein synthesis
- New proteins mediate all physiological effects - Costanzo Physiology, p. 428
9. Physiological Effects of Thyroid Hormones
a) Basal Metabolic Rate (BMR)
- Most pronounced effect: ↑ BMR, ↑ O₂ consumption, ↑ heat production
- Mechanism: induction of Na⁺-K⁺ ATPase in most tissues → more ATP consumed → more O₂ required → more heat generated
- This is the basis of "calorigenesis" - Costanzo Physiology, p. 428
b) Metabolism
- Carbohydrate: ↑ GI glucose absorption, ↑ glycogenolysis, ↑ gluconeogenesis (potentiates catecholamines and glucagon)
- Fat: ↑ lipolysis (releases free fatty acids), ↑ cholesterol synthesis AND degradation (net: ↓ cholesterol - hypothyroidism → hypercholesterolaemia)
- Protein: Both synthesis and degradation increased, but net effect is catabolic → decreased muscle mass at high levels
- Key enzymes induced: cytochrome oxidase, α-glycerophosphate dehydrogenase, malic enzyme, proteolytic enzymes
c) Cardiovascular System
- ↑ Heart rate and ↑ contractility → ↑ cardiac output
- Mechanism: induction of cardiac β₁-adrenergic receptors, cardiac myosin heavy chain, and sarcoplasmic reticulum Ca²⁺-ATPase
- Also causes peripheral vasodilation (due to ↑ tissue O₂ demand and heat) → ↓ SVR
- Net: ↑ pulse pressure, bounding pulse (classic hyperthyroid sign)
d) Growth and Development
- Acts synergistically with growth hormone (GH) and somatomedins (IGF-1) to promote linear bone growth
- Promotes ossification, fusion of bone plates, and bone maturation
- In hypothyroidism: bone age < chronological age
e) Central Nervous System (CNS)
- Critical age-dependent effects:
- Perinatal period: Essential for CNS maturation. Hypothyroidism → irreversible mental retardation (cretinism) - this is why neonatal thyroid screening is mandatory
- Adults: Hypothyroidism → listlessness, somnolence, impaired memory, slowed reflexes; Hyperthyroidism → hyperexcitability, hyperreflexia, irritability
f) Sympathetic Nervous System Interaction
- Thyroid hormones up-regulate β₁-adrenergic receptors on myocardium and other tissues
- Effects of thyroid hormones on heart rate, cardiac output, lipolysis, and gluconeogenesis are synergistic with catecholamines
- Clinical significance: β-blockers (propranolol) effectively relieve many symptoms of hyperthyroidism (tachycardia, tremor) - Costanzo Physiology, p. 429
10. Calcitonin (from C Cells)
- Secreted by parafollicular (C) cells derived from neural crest (via ultimobranchial body)
- Released in response to elevated blood Ca²⁺
- Action: inhibits osteoclast activity → ↓ bone resorption → ↓ plasma Ca²⁺
- In humans, this role is less physiologically important than parathyroid hormone (PTH) and vitamin D for calcium homeostasis - Ganong's, p. 369
11. Pathophysiology Summary
| Feature | Hypothyroidism | Hyperthyroidism |
|---|---|---|
| BMR | ↓ (weight gain, cold intolerance) | ↑ (weight loss, heat intolerance) |
| Heart rate | Bradycardia | Tachycardia |
| Reflexes | Slow (delayed relaxation) | Hyperreflexia |
| Cholesterol | ↑ | ↓ |
| CNS | Fatigue, somnolence, poor memory | Anxiety, tremor, insomnia |
| Skin/hair | Dry skin, coarse hair, myxedema | Warm, moist skin; fine hair |
| TSH level | ↑ (primary) / ↓ (secondary) | ↓ (primary) / ↑ (secondary) |
| Common causes | Hashimoto's thyroiditis, iodine deficiency | Graves' disease, toxic adenoma |
Key take-home points:
- T4 is the main secretory product but is a prohormone; T3 is the active hormone
- The thyroid is unique in extracellular, long-term hormone storage (2-3 months reserve)
- Synthesis requires iodine, thyroglobulin, and thyroid peroxidase - block any one and you block hormone production
- Free T3 exerts negative feedback on the anterior pituitary
- Thyroid hormones act genomically via nuclear receptors to increase Na⁺-K⁺ ATPase and β₁-adrenergic receptors in key tissues
This is a shared conversation. Sign in to Orris to start your own chat.