Meningitis pathology notes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive, authoritative content from multiple Robbins textbooks. I have everything needed for thorough pathology notes on meningitis. Let me compile the full answer.
Meningitis - Pathology Notes
Sources: Robbins Pathologic Basis of Disease (9th ed.), Robbins & Kumar Basic Pathology, Bradley and Daroff's Neurology in Clinical Practice, Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Definition
Meningitis is an inflammatory process involving the leptomeninges and CSF within the subarachnoid space, usually infectious in origin. When inflammation extends into the underlying brain parenchyma, it is termed meningoencephalitis.
Non-infectious causes include:
- Chemical meningitis - reaction to an irritant (e.g., debris from a ruptured epidermoid cyst)
- Carcinomatous meningitis - metastatic cancer cells spreading to the subarachnoid space
Routes of CNS Entry
- Hematogenous spread - most common; usually via arterial circulation, but retrograde venous spread via facial vein anastomoses can occur
- Direct implantation - trauma, congenital malformations (e.g., meningomyelocele)
- Local extension - from infected adjacent structures (sinuses, teeth, skull, vertebrae, mastoid, middle ear)
- Peripheral nerve transport - viruses travel retrogradely (e.g., rabies, herpes zoster)
Classification
Infectious meningitis is classified into three broad types based on etiology and clinical evolution:
| Type | Usual Cause | CSF Cells |
|---|---|---|
| Acute pyogenic | Bacterial | Neutrophils (PMNs) |
| Aseptic | Viral | Lymphocytes |
| Chronic | TB, spirochetes, fungi | Lymphocytes/monocytes |
1. Acute Pyogenic (Bacterial) Meningitis
Organisms by Age Group
| Age Group | Common Organisms |
|---|---|
| Neonates | E. coli, group B streptococci |
| Adolescents/young adults | Neisseria meningitidis |
| Older adults | Streptococcus pneumoniae, Listeria monocytogenes |
Note: N. meningitidis and S. pneumoniae colonize the nasopharyngeal mucosa and gain entry via that route. Listeria is usually acquired via contaminated food.
Clinical Features
- Systemic signs of infection + meningeal irritation + neurologic impairment
- Headache, photophobia, irritability, clouding of consciousness, neck stiffness
- Kernig sign, Brudzinski sign
- CSF: increased pressure, abundant neutrophils, elevated protein, reduced glucose
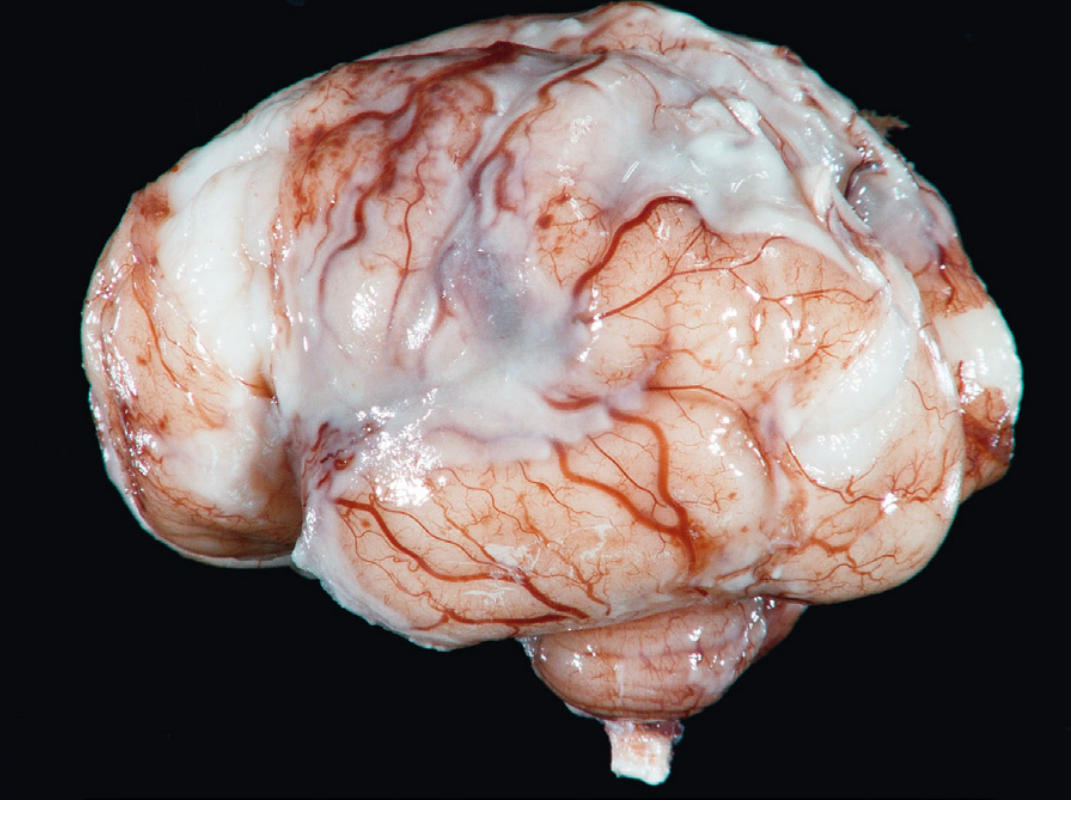
Gross Morphology (MORPHOLOGY)
- An exudate is evident within the leptomeninges over the surface of the brain
- Meningeal vessels are engorged and stand out prominently
- Distribution varies by organism:
- H. influenzae: exudate tends to be basal
- S. pneumoniae: densest over the cerebral convexities near the sagittal sinus
- Tracts of pus follow along blood vessels on the brain surface
- In fulminant cases: inflammation extends to the ventricles - ventriculitis
- The ventricles can be a portal for CSF involvement because the choroid plexus lacks a blood-brain barrier
Microscopic Morphology
- Neutrophils fill the subarachnoid space in severely affected areas
- In less severe cases: PMNs are predominantly around leptomeningeal blood vessels
- Gram stain reveals variable numbers of bacteria in untreated cases
- The pia is rarely breached in bacterial meningitis
- In fulminant cases: inflammatory cells (mostly neutrophils) infiltrate walls of leptomeningeal veins and may extend focally into the brain parenchyma (cerebritis)
- Secondary vasculitis and venous thrombosis may lead to hemorrhagic cerebral infarction
Sequelae / Complications
- Leptomeningeal fibrosis - may follow pyogenic meningitis and cause hydrocephalus (due to obstruction of CSF flow at arachnoid villi or cisterns)
- Chronic adhesive arachnoiditis - especially in pneumococcal meningitis; large quantities of organism-derived capsular polysaccharide produce a gelatinous exudate that promotes arachnoid fibrosis
2. Acute Aseptic (Viral) Meningitis
Definition
A clinical syndrome of meningeal irritation + fever + altered consciousness, with no organisms identified by bacterial culture. Usually viral, but may be bacterial, rickettsial, or autoimmune.
Etiology
- Enteroviruses - most common, accounting for ~80% of cases with identified pathogen
- Other agents: influenza species, lymphocytic choriomeningitis virus (LCMV)
- The etiologic agent is identified only in a minority of cases overall
CSF Findings (distinguish from bacterial)
| Feature | Bacterial (Pyogenic) | Viral (Aseptic) |
|---|---|---|
| WBC | Neutrophils dominant | Lymphocytic pleocytosis |
| Protein | Markedly elevated | Moderately elevated |
| Glucose | Reduced | Nearly always normal |
| Culture | Positive | Negative |
Course
- Less fulminant than pyogenic meningitis
- Usually self-limited, treated symptomatically
Chemical Meningitis (Aseptic variant)
- Caused by rupture of an epidermoid cyst into subarachnoid space, or introduction of a chemical irritant
- CSF: sterile, neutrophilic pleocytosis, increased protein, but normal glucose
3. Chronic Meningitis
Tuberculous Meningitis
Etiology: Mycobacterium tuberculosis - the leading cause of chronic meningitis worldwide
Key features:
- <50% of adults have a history of prior pulmonary TB
- Patients present with lethargy, stupor, or coma + nuchal rigidity
- May have a fulminant course despite being "chronic"
CSF:
- Elevated opening pressure
- 1-500 WBC, predominantly lymphocytes/monocytes (resembles aseptic meningitis)
- Protein >100 mg/dL
- Glucose decreased (but rarely <20 mg/dL)
- Organisms seen on smear in minority; cultures take weeks; PCR sensitivity 25-80%
Imaging: Contrast enhancement of meninges, often hydrocephalus
Pathology: Basal exudate with granuloma formation (caseating granulomas), involvement of cranial nerves at the base of the brain, obliterative endarteritis causing infarction
DDx: Sarcoidosis, leptomeningeal metastases, Wegener's granulomatosis, Behçet's disease - all can mimic TB meningitis due to low or absent cell counts
Prognosis: Untreated - usually fatal within a few weeks
Listeria Meningitis
- Predominantly in immunocompromised patients
- Can cause a chronic infection lasting weeks
- Predilection for brainstem - cystic lesions/abscesses causing cranial neuropathies
- Key point: responds to ampicillin, not to many broad-spectrum antibiotics used for bacterial meningitis - always include ampicillin when Listeria is in the differential
4. Fungal Meningitis
Cryptococcal Meningitis (Cryptococcus neoformans)
- Most common in immunocompromised (e.g., AIDS patients)
- Imaging may show gelatinous pseudocysts in basal ganglia on T2 MRI
- Complications include: hydrocephalus, infarction, cryptococcoma
- CSF CrAg (cryptococcal antigen) test: rapid, specific, sensitivity >90%
CSF Analysis Summary Table
| Type | Appearance | WBC | Protein | Glucose | Other |
|---|---|---|---|---|---|
| Normal | Clear | 0-5 lymph | 15-45 mg/dL | 60-80% serum | - |
| Bacterial | Turbid/purulent | Hundreds-thousands PMNs | Very high | Very low | + Culture, + Gram stain |
| Viral | Clear | Tens-hundreds lymph | Mildly high | Normal | - Culture |
| TB/Fungal | Xanthochromic/clear | Lymph/mono | High (>100) | Low | ZN/India ink/PCR/CrAg |
Key Complications of Meningitis
| Complication | Mechanism |
|---|---|
| Hydrocephalus | Leptomeningeal fibrosis blocking CSF reabsorption at arachnoid granulations or CSF flow through cisterns |
| Cerebral infarction | Secondary vasculitis + venous thrombosis of leptomeningeal vessels |
| Subdural empyema | Extension of infection beneath the dura |
| Ventriculitis | Extension of exudate into ventricles in fulminant bacterial disease |
| Cerebritis / brain abscess | PMN infiltration extends through pia into parenchyma |
| Cranial nerve palsies | Especially in TB and cryptococcal meningitis (basal exudate) |
| Hearing loss | Cochlear damage from labyrinthitis or cochlear nerve involvement |
| SIADH | Hypothalamic involvement leading to hyponatremia |
| Adrenal hemorrhage | Waterhouse-Friderichsen syndrome in meningococcal septicemia |
Waterhouse-Friderichsen Syndrome
- Bilateral adrenal hemorrhage associated with meningococcal (N. meningitidis) septicemia
- Fulminant course with purpuric rash (petechiae/purpura from DIC), septic shock, adrenal insufficiency
- Pathology: bilateral massive adrenal hemorrhage, DIC
Robbins Pathologic Basis of Disease, pp. 1164-1165 | Robbins & Kumar Basic Pathology, p. 833 | Bradley and Daroff's Neurology in Clinical Practice, p. 1698 | Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 421
Brudzinski's sign
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have everything needed from the textbooks. Here is the complete answer:
Brudzinski's Sign
Definition: A clinical sign of meningeal irritation. It is positive when passive flexion of the neck causes spontaneous flexion of the hips and knees in a patient lying supine.
How to Elicit It
- Patient lies supine
- Examiner passively flexes the patient's neck (chin toward chest)
- Positive sign: the patient involuntarily flexes both hips and knees in response
Mechanism
Passive neck flexion stretches the inflamed meninges. Because the meninges are continuous along the neuraxis, this tension is transmitted caudally. Reflexive hip and knee flexion reduces traction on the inflamed meningeal/nerve root structures, relieving pain - this is the body's protective response to meningeal irritation.
Alongside Other Signs of Meningeal Irritation
| Sign | How elicited | Positive response |
|---|---|---|
| Nuchal rigidity | Passive neck flexion (chin to chest) | Resistance / inability to touch chin to chest - pathognomonic sign |
| Brudzinski's sign | Passive neck flexion (supine) | Spontaneous hip and knee flexion |
| Kernig's sign | Hip flexed 90°, attempt to passively extend the knee | Pain and resistance in the hamstrings |
Clinical Significance
- All three signs (nuchal rigidity, Kernig's, Brudzinski's) are classic signs of meningeal irritation seen in meningitis and subarachnoid hemorrhage
- Important caveat: sensitivity is approximately 30% or lower for diagnosing acute bacterial meningitis in adults - they can be absent despite confirmed meningitis
- The classic triad of fever + stiff neck + change in mental status is initially present in only a subset of patients
- May be absent or reduced in:
- Very young or elderly patients
- Immunocompromised individuals
- Patients with severely depressed mental status
- Cervical spine disease in older patients can cause false-positive nuchal rigidity
Confirmed By
Brudzinski's sign combined with other findings confirms meningitis - as Plum and Posner state: "Resistance to neck flexion in the presence of easy lateral movement suggests meningeal inflammation... Flexion of the legs upon flexing the neck (Brudzinski's sign) confirms meningitis."
Sources: Harrison's Principles of Internal Medicine 22e, p. 1163 | Neuroanatomy through Clinical Cases 3rd ed. | Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 98 | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.