Anatomy of larynx Inside out , from basic till applied clinical From scott brown , cummings and stamburger
Reading File
Finding Sources
Finding Sources
Anatomy of larynx Inside out , from basic till applied clinical From scott brown , cummings and stamburger Include images as well
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Anatomy of the Larynx — Inside Out, Basic to Clinical
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery (9th ed, Vol 1 & 2), Cummings Otolaryngology Head and Neck Surgery, K.J. Lee's Essential Otolaryngology
Note on Stamberger: The library database contains Scott-Brown, Cummings, and K.J. Lee's (the most practical ENT reference). Stamberger's Functional Endoscopic Sinus Surgery is available for sinus anatomy, but the larynx chapters in the database come from Scott-Brown and Cummings — all content below is directly from those authoritative ORL texts, supplemented by KJ Lee where it adds detail.
1. OVERVIEW AND TOPOGRAPHY
The larynx extends from the laryngeal inlet to the inferior border of the cricoid cartilage. At neutral lung volume and in the absence of respiration, it lies anterior to the 3rd–6th cervical vertebrae - slightly higher in women. Anatomically it extends from the tip of the epiglottis at C3 to the lower border of the cricoid at C6.
Sex differences:
- Angle of thyroid cartilage fusion: ~90° in men, ~120° in women
- AP diameter (post-puberty): ~36 mm in men, ~26 mm in women - largely due to the anterior-posterior doubling during male puberty
Paediatric larynx: Proportionally smaller, funnel-shaped, narrowest at the subglottis-trachea junction (clinically critical - even small oedema causes severe obstruction). The adult larynx is narrowest at the glottis. Laryngeal cartilages are softer in infants and collapse more easily on forced inspiration (Bernoulli effect). The larynx starts high under the tongue in infancy and descends with age.
- Scott-Brown's Otorhinolaryngology, Vol 2, p. 928
2. FRAMEWORK OF THE LARYNX
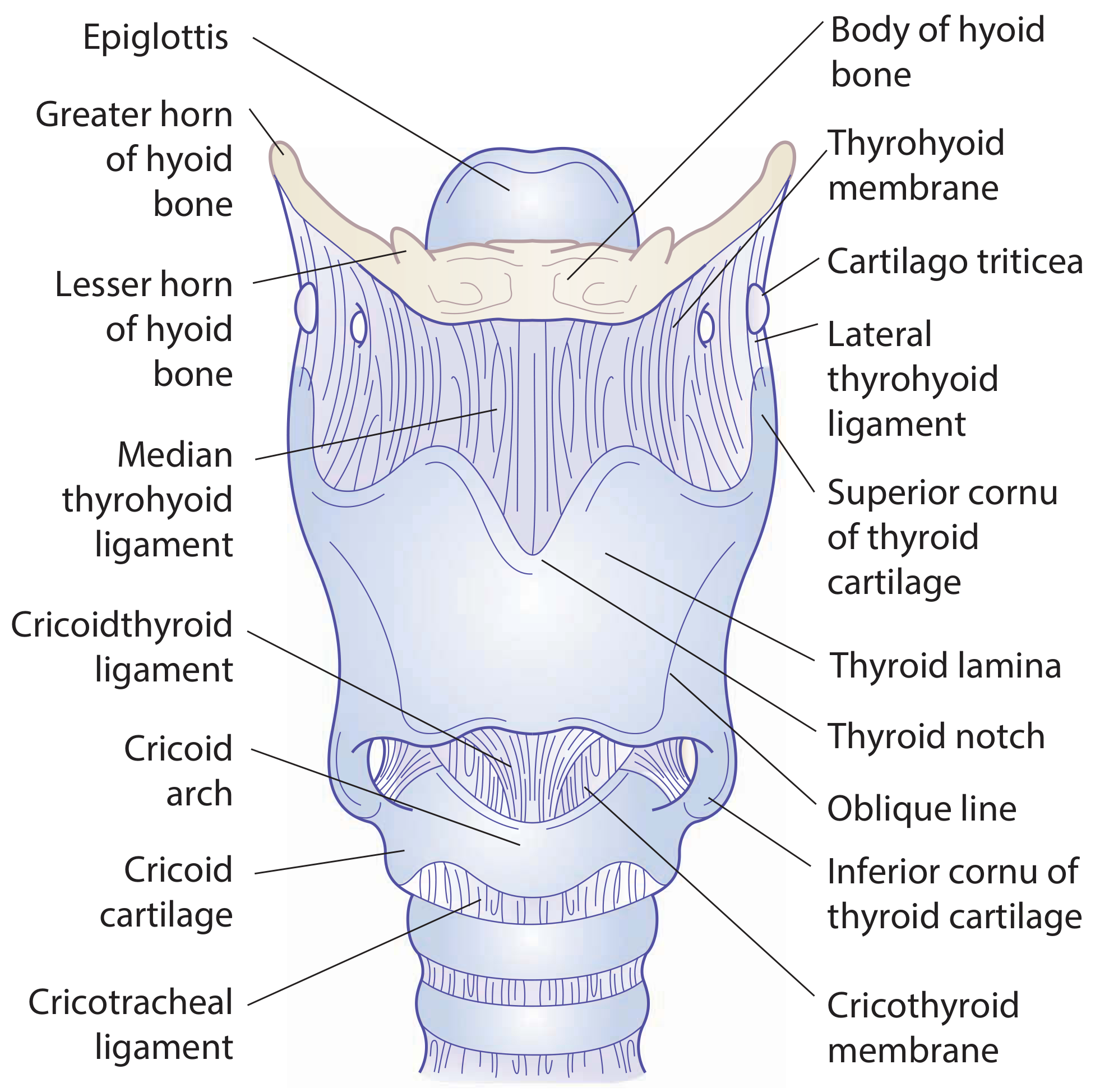
Figure: The complete laryngeal framework — anterior view. Scott-Brown's, p. 929
A. HYOID BONE
The hyoid is a U-shaped bone, the only bone in the body that does not articulate with another bone. It consists of:
- A body anteriorly
- Greater cornua projecting backwards on each side
- Lesser cornua - small conical eminences on the upper lateral aspect of the body, joined by fibrous band or synovial joint
Function: Suspended by suprahyoid muscles/ligaments from the skull base and mandible; provides superior attachment for extrinsic laryngeal muscles, thereby suspending the larynx in the neck.
Clinical: The hyoid can be fractured in blunt neck trauma (and in manual strangulation, forensically important). CT shows linear lucencies with displacement, best seen on bone windows in ossified cartilage.
B. THYROID CARTILAGE
Composed of two laminae fused anteriorly in the midline → the laryngeal prominence (Adam's apple).
- Fusion angle: ~90° men, ~120° women (hence more prominent in men)
- Posterior border of each lamina extends as superior cornu (long, narrow, curves up/back/medially - attached to lateral thyroid ligament) and inferior cornu (shorter, thicker, curves down/medially, articulates with cricoid via cricothyroid joint)
- Oblique line on the outer surface gives attachment to the inferior pharyngeal constrictor, sternothyroid, and thyrohyoid muscles
- The thyroid notch is at the upper border between the two laminae
C. CRICOID CARTILAGE
The cricoid is the only complete ring in the airway. It is the most important structural support of the larynx.
- Arch - narrow anteriorly (~5–7 mm tall)
- Lamina - broad posteriorly (~20–30 mm tall)
- Articulates with: the inferior cornua of thyroid (cricothyroid joint - pivot joint allowing rocking/gliding) and with the arytenoid cartilages (cricoarytenoid joint - saddle joint allowing gliding/rotation)
Cartilage type: Hyaline cartilage - begins to ossify from age ~20, therefore radiopaque on X-ray in adults. This is clinically significant for CT assessment of tumour invasion.
- Cummings, p. 2124
D. ARYTENOID CARTILAGES (paired)
Each arytenoid is a pyramidal structure with:
- Apex - articulates with the corniculate cartilage above; points posteromedially
- Vocal process - projects anteriorly; gives attachment to the vocal ligament
- Muscular process - projects laterally; gives attachment to the PCA and LCA muscles
- Body - bears the cricoarytenoid joint surface inferiorly
Cartilage type: Mixed - the vocal process and apex are elastic cartilage (does NOT ossify, not radiopaque). The body is hyaline (ossifies after ~20 years).
Movement: The cricoarytenoid joint allows:
- Rotation (abduction/adduction of vocal process)
- Gliding (anteroposterior and mediolateral) Combined movements determine glottic configuration.
E. EPIGLOTTIS
- Leaf-shaped, elastic cartilage (does NOT ossify)
- Attached inferiorly to the back of the thyroid angle via the thyroepiglottic ligament
- Attached superiorly to the hyoid via the hyoepiglottic ligament
- The petiolus (stalk) is the narrow inferior end
- Perforations in the epiglottis allow tumour to enter the pre-epiglottic space
F. MINOR CARTILAGES
- Corniculate (Santorini): Sits on the apex of the arytenoid; elastic cartilage; creates the corniculate tubercle seen endoscopically at the posterior laryngeal inlet
- Cuneiform (Wrisberg): Lies in the aryepiglottic fold anterior to corniculate; elastic cartilage; creates the cuneiform tubercle
- Cartilago triticea: Small nodule in the lateral thyrohyoid ligament (seen in the framework image above)
3. LIGAMENTS AND MEMBRANES
The laryngeal framework image above shows the key membranes. The internal fibrous framework divides into two parts:
Fibroelastic Membrane - TWO LAYERS:
Upper part - Quadrilateral Membrane:
- Spans from epiglottis/aryepiglottic fold down to the false cords
- Lower free border forms the vestibular (false cord) ligament
- Upper free border is the aryepiglottic fold
Lower part - Conus Elasticus (Cricovocal Membrane):
- Arises from the upper border of the cricoid arch
- Fans upward and medially
- Upper free border (thickened) = the vocal ligament
- Anteriorly - the cricothyroid ligament (median cricothyroid membrane) - the key surgical landmark for emergency airway access (cricothyroidotomy)
External Membranes:
- Thyrohyoid membrane: Connects hyoid to the upper border of the thyroid cartilage. Pierced by the internal branch of the SLN and the superior laryngeal artery. The lateral (free) portion is thickened as the lateral thyrohyoid ligament (may contain cartilago triticea)
- Cricothyroid membrane: Between thyroid and cricoid anteriorly - the surgical landmark
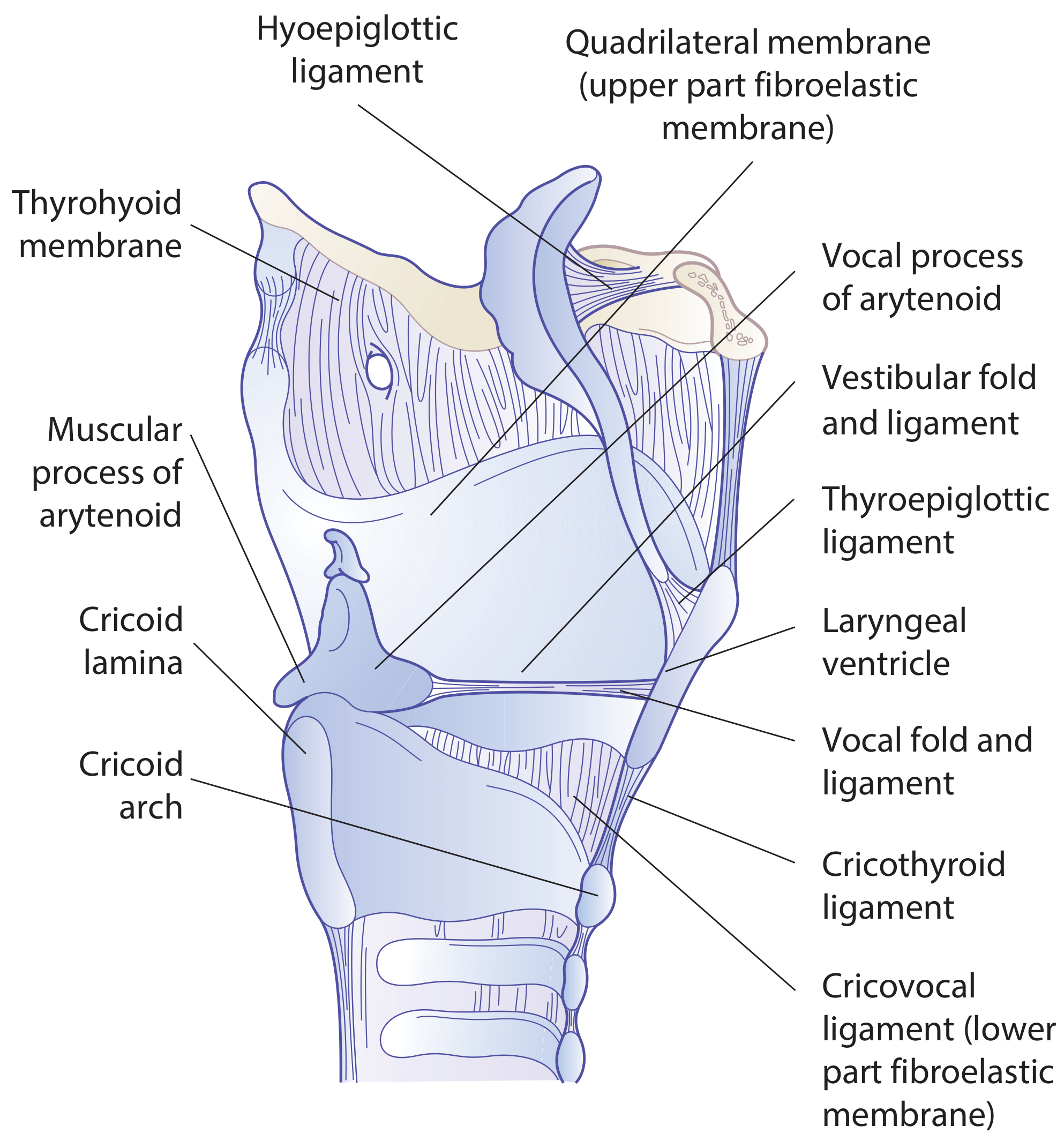
Figure: Sagittal section of the larynx. Scott-Brown's, p. 928
4. INTERNAL ANATOMY - THE THREE REGIONS
The larynx is divided into supraglottis, glottis, and subglottis by the true and false folds.
SUPRAGLOTTIS
- Extends from the epiglottis/aryepiglottic folds superiorly to a horizontal line through the apex of the laryngeal ventricle inferiorly
- Includes: (1) epiglottis (suprahyoid and infrahyoid portions), (2) aryepiglottic folds, (3) arytenoids, (4) false (vestibular) cords, (5) ventricle
- Embryological note: The supraglottis has a separate embryological origin from the glottis/subglottis - this explains why supraglottic and glottic cancers have different lymphatic drainage patterns
GLOTTIS
- From the ventricle apex to 5 mm below the free edge of the true vocal folds (or 1 cm below the ventricle apex)
- Includes: true vocal cords, anterior commissure, posterior commissure
SUBGLOTTIS
- From the lower boundary of the glottis to the inferior margin of the cricoid cartilage
- Anterior commissure (Broyle's tendon): The lower edges of the vocal folds converge anteriorly. Broyle's ligament attaches the vocal folds to the inner thyroid cartilage here - there is no perichondrium at this point, meaning tumour can invade the cartilage directly. Also, Broyle's ligament connects to the subglottis via the apex of a triangle with the epiglottis, so anterior commissure tumours readily involve the subglottis.
- Scott-Brown's, p. 929; Cummings, p. 2124
5. VOCAL FOLD - LAYERED STRUCTURE
The vocal fold (preferred term over "vocal cord") is a layered structure - not a simple cord. This is the foundation of modern phonomicrosurgery.
| Layer | Structure |
|---|---|
| Epithelium | Non-keratinizing stratified squamous epithelium |
| Superficial lamina propria | "Reinke's space" - loose areolar tissue, gelatinous, prone to oedema |
| Intermediate lamina propria | Elastic fibres |
| Deep lamina propria | Collagen fibres |
| Intermediate + deep LP together | = The vocal ligament |
| Muscle | Thyroarytenoid/Vocalis muscle (the body of the fold) |
Reinke's space (superficial lamina propria) is loosely attached - this is why Reinke's oedema accumulates here and why submucosal tumours can spread extensively with minimal mucosal change.
Membranous vs cartilaginous vocal fold:
- Anterior 3/5 (anterior commissure to tip of vocal process) = membranous part - where vibration and pathology mainly occur
- Posterior 2/5 (vocal process to arytenoid face) = cartilaginous part
Macula flava: A small nodular structure at each end of the membranous fold, acting as a cushion to protect against mechanical damage from vibration.
6. THE LARYNGEAL VENTRICLE AND SACCULE
- The ventricle (of Morgagni) is the fusiform recess between the false cord above and the true cord below
- The saccule (appendix) is an upward diverticulum from the anterior part of the ventricle, projecting superolaterally between the vestibular fold and inner thyroid cartilage
- The saccule is lined with mucous glands that lubricate the vocal folds (which themselves have NO glands)
- Fibrous tissue surrounds the saccule
- Clinical: Dilatation of the saccule → laryngocele. Causes: increased intraglottic pressure (horn players, glass blowers) OR obstruction by inflammatory/neoplastic lesion. An internal laryngocele stays within the paraglottic space; an external (mixed) laryngocele pierces the thyrohyoid membrane and presents as a neck mass. The saccule can harbour occult cancers - must be actively inspected during diagnostic endoscopy.
7. SPACES WITHIN THE LARYNX
These contain fat, lymphatics and vessels, and represent critical pathways of tumour spread.
PRE-EPIGLOTTIC SPACE (PES)
- Wedge-shaped, point inferiorly
- Bounded: anteriorly by the thyrohyoid membrane/hyoid; posteriorly by the epiglottis
- Superiorly: hyoepiglottic ligament
- Tumour enters through perforations in the epiglottis or through the hyoepiglottic ligament
- Continuous laterally with the paraglottic space (no anatomical boundary between them)
PARAGLOTTIC SPACE (PGS)
- Bounded: laterally by thyroid cartilage; medially by conus elasticus + quadrangular membrane; posteriorly by piriform fossa mucosa
- Contains the laryngeal ventricle and saccules
- Tumours may spread extensively in this space with minimal mucosal changes - this is why submucosal tumour spread can be missed on endoscopy
- The paraglottic and pre-epiglottic spaces communicate freely - explaining why supraglottic cancers can cross midline via the pre-epiglottic space
- Scott-Brown's, p. 934-935
8. MUCOUS MEMBRANE AND EPITHELIUM
- Closely adherent (prone to perichondritis if inflamed): over posterior surface of epiglottis, corniculate/cuneiform cartilages, and over the vocal ligament
- Loosely adherent (prone to oedema): everywhere else - e.g. the aryepiglottic folds, false cords → this is why supraglottic oedema (angioedema, epiglottitis) can be life-threatening
Epithelial types:
- Pseudostratified ciliated columnar epithelium ("respiratory" type): Most of the larynx
- Non-keratinizing stratified squamous epithelium: Upper half of posterior epiglottis, upper aryepiglottic fold, posterior glottis, and the vocal folds themselves
Mucous glands: Freely distributed everywhere, especially on posterior epiglottis (indenting the cartilage) and at the saccules. The vocal folds have NO glands - they are lubricated entirely by saccular secretions. After radiation, saccular glands fail → vocal fold desiccation.
9. INTRINSIC MUSCLES OF THE LARYNX
All intrinsic muscles are innervated by the RLN, except the cricothyroid which is innervated by the external branch of the SLN.
| Muscle | Origin | Insertion | Action | Clinical note |
|---|---|---|---|---|
| Posterior cricoarytenoid (PCA) | Lower/medial surface of cricoid lamina | Muscular process of arytenoid | Only abductor of the vocal folds | Bilateral paralysis → stridor/asphyxia. Activity synchronous with inspiration, precedes diaphragm by 40–100 ms |
| Lateral cricoarytenoid (LCA) | Superior border of cricoid arch | Muscular process of arytenoid | Adducts vocal fold (lowers, elongates, sharpens edge) | Fast muscle: peak contraction ~19 ms |
| Transverse arytenoid | Posterior surface of one arytenoid | Same point on other arytenoid | Adducts vocal folds (unpaired) | Only bilateral innervation of any intrinsic muscle |
| Oblique arytenoid | Muscular process | Apex of opposite arytenoid | Adducts, aids sphincteric closure | Continues as aryepiglottic muscle into fold |
| Thyroarytenoid (TA)/Vocalis | Back of thyroid angle + cricothyroid ligament | Vocal process + anterolateral arytenoid body | Shortens, thickens, lowers vocal fold; stiffens body, slackens cover | Vocalis = medial part, controls fine mass/tension. Atrophy → reduced fold volume + glottic incompetence. Fast: ~14 ms |
| Cricothyroid (CT) | Outer surface of cricoid arch | Inferior border/horn of thyroid cartilage | Elongates, tenses, and thins vocal folds (tilts cricoid/thyroid toward each other) | Only intrinsic muscle outside the cartilaginous framework. Innervated by external SLN, not RLN |
- Scott-Brown's Table 58.2, p. 932; Cummings, p. 723; KJ Lee, p. 909–912
Muscle fibre types (Cummings, p. 729):
- PCA: ~equal type 1 and type 2A (aerobic, fatigue-resistant; peak contraction ~40 ms)
- TA: ~40% type 1, 55% type 2A, 5% type 2B
- LCA: fast (peak ~19 ms)
- CT: majority type 1 (aerobic) - peak ~50 ms
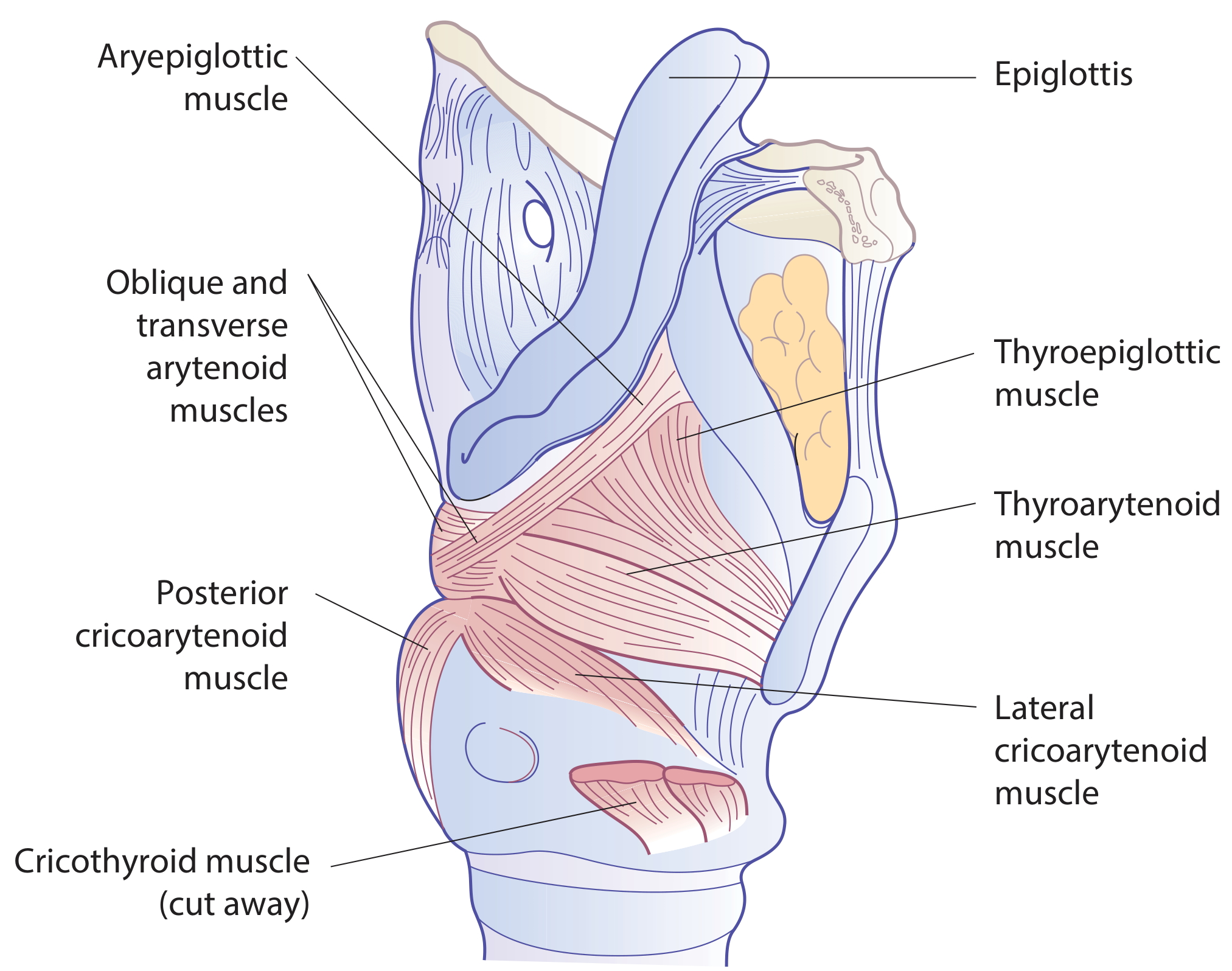
Figure: Lateral view with thyroid cartilage removed - intrinsic muscles. Scott-Brown's, p. 932
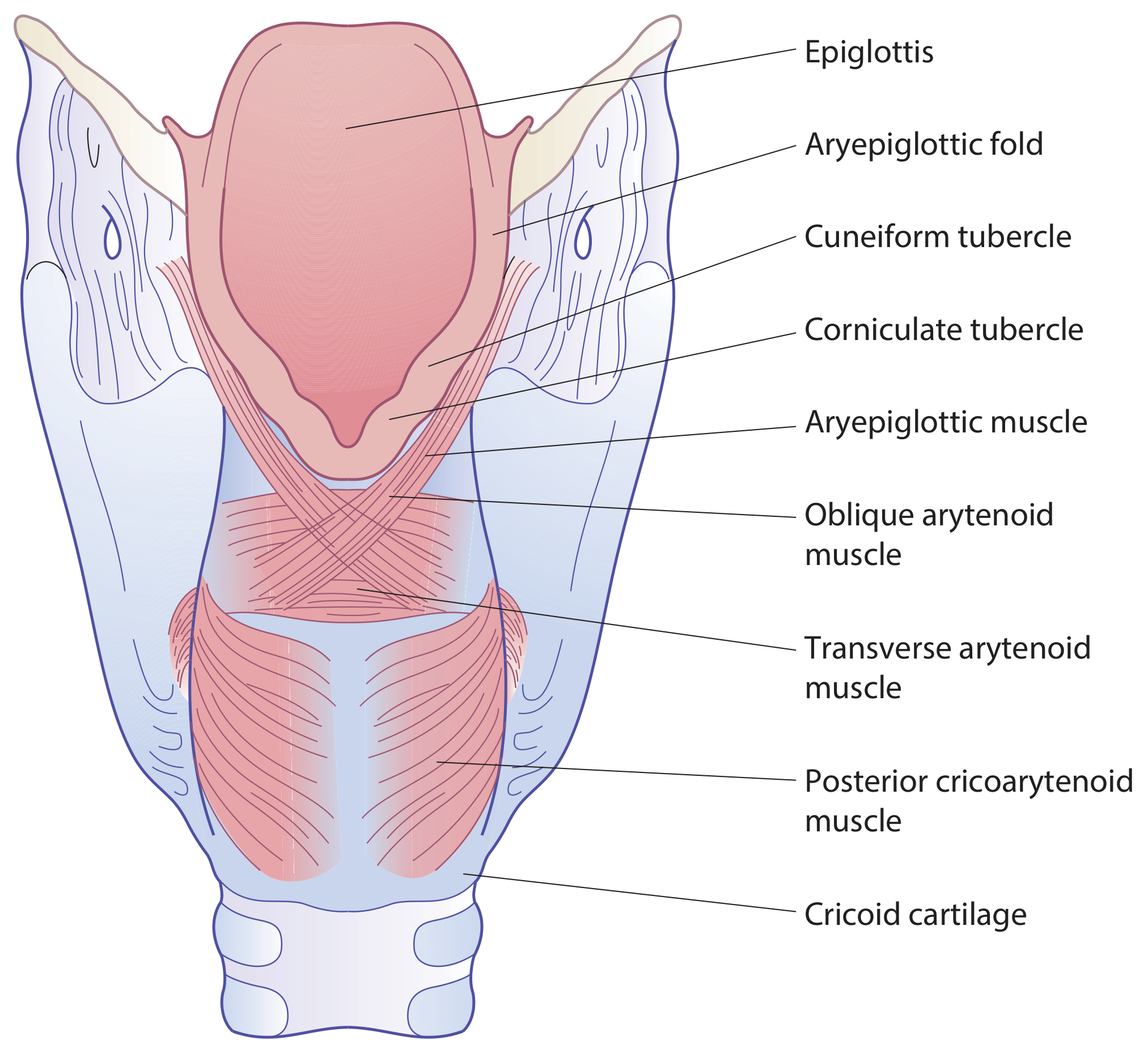
Figure: Posterior view of larynx. Scott-Brown's, p. 932
10. EXTRINSIC MUSCLES
Connect the larynx to surrounding structures. Divided into depressors and elevators.
Depressors (strap muscles):
| Muscle | Innervation |
|---|---|
| Sternohyoid | Ansa cervicalis (C2, C3) |
| Thyrohyoid | C1 (via hypoglossal nerve) |
| Omohyoid | Ansa cervicalis (C2, C3) |
| Sternothyroid | Ansa cervicalis (C2, C3) |
Elevators:
| Muscle | Innervation |
|---|---|
| Geniohyoid | C1 |
| Digastric (anterior belly) | CN V3 |
| Digastric (posterior belly) | CN VII |
| Mylohyoid | CN V3 |
| Stylohyoid | CN VII |
Pharyngeal constrictors:
- Inferior constrictor: arises from oblique line of thyroid cartilage - its lowermost circular fibres = cricopharyngeus (upper oesophageal sphincter), attaching to posterolateral cricoid. Clinically important in dysphagia and Zenker's diverticulum.
- KJ Lee, p. 910
11. NERVE SUPPLY
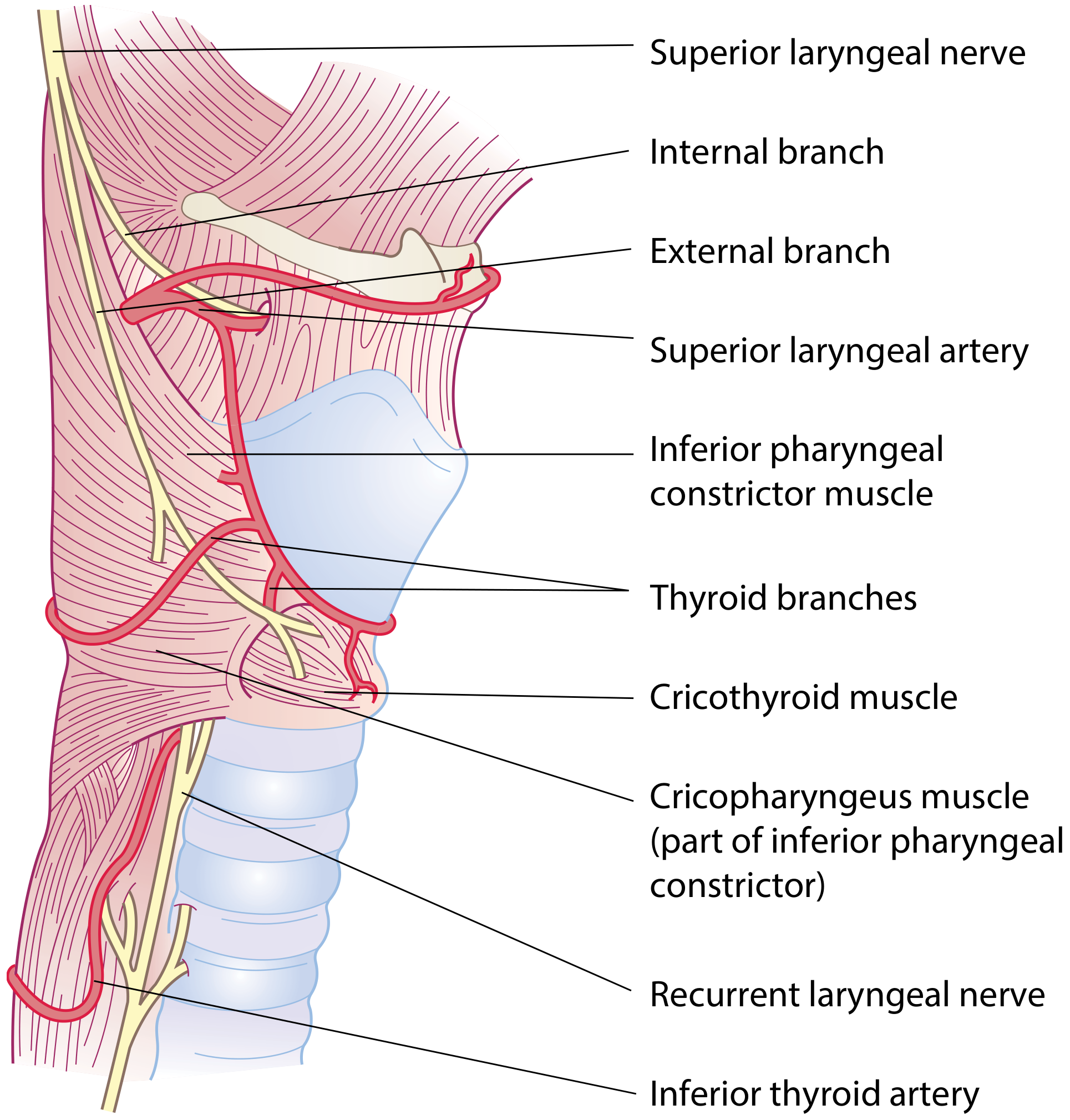
Figure: Nerve and blood supply of the larynx. Scott-Brown's, p. 935
Superior Laryngeal Nerve (SLN)
- Arises from the inferior (nodose) ganglion of the vagus
- Receives a branch from the superior cervical sympathetic ganglion
- Descends lateral to the pharynx, behind the internal carotid artery
- At the level of the greater horn of the hyoid, divides into:
External branch (motor):
- Innervates cricothyroid muscle
- Also innervates inferior constrictor
- Runs close to the superior thyroid artery near the upper thyroid pole → at risk during thyroidectomy (Joll's triangle)
- Injury: loss of high-pitched voice, inability to project voice, vocal fatigue
Internal branch (sensory + secretomotor):
- Larger
- Pierces the thyrohyoid membrane just above the superior laryngeal artery
- Upper branch: mucosa of lower pharynx, epiglottis, valleculae, vestibule
- Lower branch: descends in the medial wall of the piriform fossa beneath mucosa → aryepiglottic fold + laryngeal mucosa down to the level of the vocal folds
- Carries afferent fibres from neuromuscular spindles and stretch receptors
- Ends by piercing the inferior constrictor and unites with ascending RLN branch = Galen's anastomosis (purely sensory)
- Clinical use: SLN block can be achieved by injecting local anaesthetic at the piriform fossa mucosa - provides excellent anaesthesia for awake fibreoptic intubation
Recurrent Laryngeal Nerve (RLN)
- Motor to ALL intrinsic muscles except cricothyroid
- Sensory below the vocal folds
Course differences (clinically critical):
- Right RLN: Loops around the right subclavian artery, ascends in the tracheo-oesophageal groove
- Left RLN: Longer course - loops around the aortic arch (at the level of the ligamentum arteriosum), ascends in the tracheo-oesophageal groove
Entry into larynx: The RLN enters beneath the lower border of the inferior constrictor (cricopharyngeus), passing deep to the cricothyroid joint. It is often in close proximity to the inferior thyroid artery - relationship is variable:
- Left RLN: more likely posterior to the artery
- Right: equal chance in any of three positions relative to artery
- Up to 30% of RLNs branch extralaryngeally before entering - increases injury risk
Surgical identification:
- Lateral approach (safest): Beahr's triangle - inferior thyroid artery (superior), trachea (medial), common carotid artery (lateral)
- Superior approach: At cricothyroid junction - useful in cancer surgery, reoperations, or when non-recurrent RLN is suspected
Non-recurrent RLN: Occurs on the right side in ~1% when the right subclavian artery arises anomalously from the descending aorta (arteria lusoria). The RLN then runs directly from the vagus to the larynx without looping - easily injured if not anticipated.
Galen's anastomosis: Junction of the descending internal SLN branch with the ascending RLN - purely sensory, but important in explaining bilateral sensory innervation of the interarytenoid region.
- Scott-Brown's, p. 935-936
12. BLOOD SUPPLY
Arterial
Three sources (all from the thyroid arterial system):
-
Superior laryngeal artery - branch of superior thyroid artery - passes deep to the thyrohyoid muscle, pierces the thyrohyoid membrane with the internal SLN to supply the upper larynx
- Risk during endoscopic supraglottic resections as it enters the paraglottic space at the anterior end of the aryepiglottic fold
-
Inferior laryngeal artery - branch of inferior thyroid artery - ascends on the trachea with the RLN, enters the larynx beneath the lower border of the inferior constrictor
-
Cricothyroid artery - branch of superior thyroid artery - crosses the upper part of the cricothyroid ligament (up to 5 branches). Can be injured during cricothyroidotomy or during resection of anterior commissure cancers.
The laryngeal arteries form a communicating plexus in the paraglottic space - source of brisk bleeding during endolaryngeal surgery.
Venous
- Superior laryngeal veins → superior thyroid or facial vein → internal jugular vein
- Inferior laryngeal veins → inferior thyroid veins → brachiocephalic vein
- Scott-Brown's, p. 936
13. LYMPHATIC DRAINAGE
The vocal folds act as a watershed - separating the upper and lower lymphatic systems. There are no lymphatics in the plane of the vocal fold itself.
| Region | Drainage |
|---|---|
| Supraglottis | Vessels accompany the superior laryngeal vein, pierce the thyrohyoid membrane → upper deep cervical nodes (Level II/III) |
| Subglottis | → Prelaryngeal (Delphian) node → paratracheal nodes (Level VI) → lower deep cervical nodes |
| Glottis (true vocal folds) | Essentially no lymphatics in this plane → early glottic cancers do not readily spread to lymph nodes |
Clinical importance:
- Glottic cancers (T1/T2) rarely have nodal metastases - voice change causes early presentation
- Supraglottic cancers present late and have bilateral nodal drainage (midline structures drain bilaterally)
- Subglottic cancers drain to Level VI - paratracheal dissection required
- Scott-Brown's, p. 936; Cummings p. 2124-2126
14. RADIOLOGICAL ANATOMY
From Cummings (p. 2124):
On lateral X-ray:
- The anterior commissure may approach within 1 cm of the skin surface - important for radiation planning
- Vocal cords attach to thyroid cartilage at the "figure-of-eight" appearance on plain lateral film
- Anatomical boundaries of supraglottis, glottis and subglottis are readily visualised on lateral X-ray
Cartilage ossification on CT:
- Thyroid, cricoid, most of arytenoid body = hyaline cartilage - ossifies from ~age 20 → radiopaque, visible on CT bone windows
- Epiglottis, corniculate, cuneiform cartilages, apex and vocal process of arytenoid = elastic cartilage - does NOT ossify → NOT radiopaque
This distinction matters for CT staging of laryngeal cancer:
- Ossified cartilage: CT highly sensitive for frank cortical destruction (irregular erosion, sclerosis, or lysis)
- Non-ossified cartilage: CT less reliable for invasion - use MRI
Fat planes on CT/MRI:
- Pre-epiglottic fat, paraglottic fat, aryepiglottic fold fat - critical landmarks on axial CT/MRI for assessing deep invasion
- Loss of fat plane = tumour spread into that space
- Cummings, p. 2124
15. CLINICAL APPLIED SUMMARY
| Structure | Clinical Application |
|---|---|
| Broyle's ligament (anterior commissure) | No perichondrium here - direct cartilage invasion; subglottic extension of glottic tumour |
| Reinke's space | Reinke's oedema (from smoking, hypothyroidism, reflux); submucosal tumour spread |
| Paraglottic space | Tumours spread here "silently" with little mucosal change; involvement = T3 disease |
| Pre-epiglottic space | Tumour spread through epiglottic perforations; determines extent of supraglottic resection |
| Laryngeal ventricle/saccule | Laryngocele formation; occult carcinoma in saccule |
| Cricothyroid membrane | Emergency surgical airway (cricothyroidotomy); cricothyroid artery branches can bleed |
| Internal SLN in piriform fossa | Site for SLN nerve block during awake intubation |
| PCA muscle | The ONLY abductor - bilateral injury = respiratory distress |
| RLN branching (~30%) | Increases surgical injury risk during thyroidectomy/neck dissection |
| Non-recurrent RLN (~1%, right) | Must be anticipated in thyroid surgery, especially with vascular anomaly |
| Supraglottic lymphatics | Bilateral drainage; early nodal spread; N0 neck must be treated electively |
| Glottic lymphatics | Absent = early presentation (hoarseness) + rare nodal spread = high cure rates |
| Subglottic drainage | Level VI/paratracheal - missed if central neck not addressed |
| Cartilage ossification | Determines CT vs MRI sensitivity for tumour invasion |
| Infantile narrow subglottis | Post-intubation subglottic stenosis; post-extubation stridor in children |
Key references used:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, Chapter 58 (p. 928–937)
- Cummings Otolaryngology Head and Neck Surgery, Chapters 8 & 110 (pp. 180, 723–734, 2124–2126)
- K.J. Lee's Essential Otolaryngology, Chapter on Larynx (pp. 909–912)
This is a shared conversation. Sign in to Orris to start your own chat.