Cervical stitch worms stitch procedure
Reading File
Finding Sources
Finding Sources
Searching PubMed
cervical cerclage procedure outcomes
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Let me compile the full answer.
Cervical Cerclage (Cervical Stitch) - Complete Procedure Guide
Cervical cerclage (commonly called a "cervical stitch") is a surgical procedure in which a suture is placed around the cervix to keep it closed during pregnancy. It is the primary treatment for cervical insufficiency - the inability of the cervix to retain a pregnancy to term due to structural or functional weakness.
Indications
Cerclage can be placed based on three different triggers:
| Type | Indication | Timing |
|---|---|---|
| History-Indicated (HIC) | Prior painless cervical dilation causing 2nd-trimester loss; prior exam-indicated cerclage | 11-15 weeks gestation |
| Ultrasound-Indicated | Prior preterm birth (16-36 weeks) + current cervical length <25 mm on TVU | Before 24 weeks |
| Physical Exam-Indicated | Painless cervical dilation on exam, <24 weeks, without labor/PROM/abruption/chorioamnionitis | Before 24 weeks |
Transabdominal cerclage is reserved for patients who have had a failed history-indicated transvaginal cerclage with subsequent preterm birth <33 weeks, or those with insufficient vaginal cervix due to müllerian anomalies or prior cervical surgery.
Contraindications
Absolute:
- Non-viable pregnancy
- Undiagnosed vaginal bleeding
- Ruptured membranes
- Active preterm labor
- Acute cervical or intrauterine infection
Relative:
- Known or suspected abnormal (chromosomally abnormal) pregnancy
- Prolapsed fetal membranes through the external os (higher risk of iatrogenic membrane rupture)
- Placenta previa with cervical dilation (controversial)
Equipment
- Bladder catheter
- Weighted vaginal speculum
- Deaver or right-angle retractor
- Ring forceps
- No. 5 Mersilene band (nonabsorbable suture) with curved needle - do not confuse with 5-0 suture, which is much smaller
- Pickups (Russian forceps)
- Metzenbaum scissors
- Needle driver
Pre-Procedure Work-Up
- Confirm intrauterine viability by ultrasound
- Rule out cervical infection (screen for gonorrhea/chlamydia)
- Consider amniocentesis for ultrasound-indicated or exam-indicated cerclage (to rule out subclinical chorioamnionitis)
- Fetal monitoring pre- and post-procedure
- Obtain informed consent
Step-by-Step Procedure (McDonald Technique)
The McDonald cerclage is the standard transvaginal technique - a purse-string suture placed in the mid-cervix.
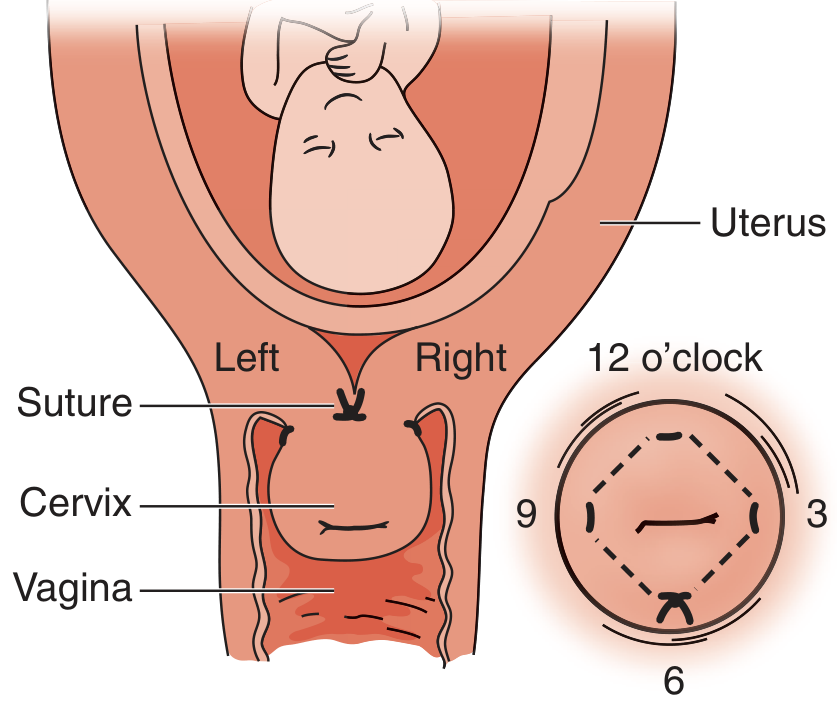
Fig: Cervical cerclage anatomy. The stitch is placed starting at 6 o'clock, passed counterclockwise through the cervical stroma at 3, 12, and 9 o'clock positions, then drawn tight as a purse-string. The knot rests posteriorly (6 o'clock) to minimize bladder irritation.
- Obtain informed consent and document intrauterine viability.
- Anesthesia: General or regional (spinal). Local/paracervical block is avoided due to concerns about uterine blood flow alteration.
- Position the patient in dorsal lithotomy; prep and drape in sterile fashion.
- Drain the bladder (Foley catheter not required - one-time drain is sufficient).
- Place a weighted speculum in the posterior vagina.
- Place a Deaver or right-angle retractor anteriorly for bladder protection; hold carefully to avoid bladder trauma.
- Grasp the anterior lip of the cervix with ring forceps and displace it superiorly to expose the posterior cervix.
- Begin the stitch at 6 o'clock (posterior position) in the mid-portion of the cervix, equidistant between the ectocervix and the cervicovaginal junction - i.e., at the level of the internal os. Pass the needle through the mid-cervical stroma - not too shallow (will tear out when tightened) and not through the canal.
- Proceed counterclockwise (right-handed surgeons): pass the suture to 3 o'clock, exit, immediately re-enter the cervix in the same area, pass to 12 o'clock, exit, re-enter, pass to 9 o'clock, exit, re-enter, finally exit at 6 o'clock.
- Cinch down the suture like a purse-string - do not draw too tightly - and tie, leaving the ends long enough to grasp with ring forceps for later removal (typically 3 knots).
- A second cerclage lower than the first is sometimes placed but has no documented improvement in outcome and increases risk of membrane rupture and bladder perforation.
- Transfer to recovery on a fetal monitor to confirm fetal viability post-procedure.
- Discharge after adequate observation. Routine antibiotics and tocolytics are NOT routinely recommended.
Common Error: Placing the suture too shallowly so that it pulls through the tissue when cinched tight. Always pass the needle through the mid-cervical stroma.
Post-Procedure Care
- Acetaminophen is usually adequate for pain
- Expect significant vaginal discharge for several weeks
- Pelvic rest: limit physical activity for at least 1 week; abstain from vaginal intercourse for at least 1 week (often for the remainder of pregnancy)
- Increased frequency of prenatal visits
- Bed rest is NOT routinely recommended
Removal
The cerclage is left in place until 37 weeks gestation and is typically removed easily in the outpatient office:
- Place in examination position, insert speculum
- Grasp the knot with Russian pickups
- Elevate and cut the suture with Metzenbaum scissors
- Remove the stitch
If preterm labor occurs and tocolysis fails, the cerclage must be removed promptly to prevent cervical laceration. If removal is difficult in the office, do not force it - proceed to the operating room.
Risks and Complications
| Complication | Notes |
|---|---|
| Rupture of membranes | Up to 65% within 2 weeks in emergent/urgent cerclage |
| Chorioamnionitis | Up to 30% in high-risk (exam-indicated) cases |
| Suture displacement | Risk of migration |
| Uterine rupture | Rare but serious |
| Maternal septicemia | Especially with subclinical infection |
| Preterm labor/delivery | May be triggered by procedure |
| Fetal loss | All of the above can lead to loss |
| Bladder perforation | More likely with second suture placement |
Evidence Summary
- Overall cerclage reduces risk of early and late preterm birth (average RR = 0.77; 95% CI 0.66-0.89) per Cochrane review
- Benefit of HIC is primarily seen in women with 3 or more second-trimester losses; evidence is weaker for those with fewer prior losses
- Transabdominal cerclage is superior to transvaginal in patients with prior failed HIC (RCT evidence)
- No evidence supports cerclage in multiple gestations for primary preterm birth prevention
- 2025 meta-analysis (PMID 40829743, Berghella et al.): cerclage for short cervix ≤20 mm before 24 weeks in singleton gestations without prior spontaneous PTB decreases preterm birth
Sources:
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed., pp. 932-933
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, pp. 889-891
- Berghella V et al., Am J Obstet Gynecol MFM, 2025 [PMID 40829743]
- Mudrik A et al., Am J Obstet Gynecol MFM, 2025 [PMID 40541862] - guidelines on cerclage placement
This is a shared conversation. Sign in to Orris to start your own chat.