Classify general anesthetics. Discuss the mechanism of action, uses and adverse effects of ketamine
Reading File
Finding Sources
Finding Sources
Searching PubMed
ketamine mechanism anesthesia NMDA
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the complete answer.
Classification of General Anesthetics & Ketamine
Classification of General Anesthetics
General anesthetics are broadly divided into two major groups based on route of administration:
I. Inhalational (Volatile) Anesthetics
These pass into the bloodstream at the alveolar-capillary interface and exert CNS effects. They are liquids at room temperature that evaporate easily for delivery as gases.
A. Volatile (Halogenated) Agents
| Agent | Key Feature |
|---|---|
| Isoflurane | FDA approved 1979; most widely used; minimal metabolism (<2%); pungent, unsuitable for inhalation induction |
| Sevoflurane | Rapid onset; low pungency, suitable for inhalational induction (especially children); <5% metabolism |
| Desflurane | Fastest onset/emergence; highly pungent (airway irritation), not suitable for mask induction; minimal metabolism (0.02%) |
| Halothane | Older agent; suitable for mask induction (low pungency); high catecholamine sensitization; >20% hepatic metabolism; hepatotoxicity risk |
| Enflurane | Older agent; medium metabolism (<10%); epileptiform EEG changes |
| Diethyl ether | Historical; very slow induction; largely obsolete |
Key pharmacodynamic properties shared by volatile agents: dose-dependent vasodilation, myocardial depression, and all are triggers for malignant hyperthermia in susceptible patients. All act as greenhouse gases with ozone-layer toxicity.
B. Gaseous Agent
- Nitrous oxide (N₂O): Weak potency (insufficient as sole anesthetic), rapid onset/offset, minimal metabolism, no sensitization to catecholamines. Used adjunctively as a carrier gas to reduce the MAC of volatile agents.
II. Intravenous (IV) Anesthetics
Used for induction and/or maintenance; often combined with inhalational agents in balanced anesthesia.
| Drug Class | Examples |
|---|---|
| Barbiturates | Thiopental, methohexital |
| Propofol | Propofol (alkylphenol) |
| Benzodiazepines | Midazolam, diazepam |
| Opioids (adjuncts) | Fentanyl, morphine, remifentanil |
| Dissociative agents | Ketamine |
| Etomidate | Etomidate (imidazole) |
| Alpha-2 agonists | Dexmedetomidine |
Modern anesthetic practice is "balanced": induction with IV agents, maintenance with inhalational or total intravenous anesthesia (TIVA), supplemented by analgesics, muscle relaxants, and anxiolytics. — Sabiston Textbook of Surgery
Ketamine
Chemistry & Pharmacokinetics
Ketamine is a phencyclidine (PCP) derivative — a chiral compound administered as a racemic mixture of S(+) and R(−) enantiomers. The S(+) enantiomer is 3–4× more potent than R(−), has shorter duration, and is cleared more rapidly. Esketamine (pure S-enantiomer) is the FDA-approved form for treatment-resistant depression.
Bioavailability by route:
- IV: 100% (onset 30–60 sec, duration 10–15 min)
- IM: 93% (onset ~5 min)
- Intranasal: 25–50%
- Oral/rectal: ~16%
Induction doses: 1–2 mg/kg IV; 4–6 mg/kg IM
Metabolism: Hepatic, via CYP3A4 > CYP2C9 > CYP2B6 → norketamine (active metabolite, 20–30% potency), excreted renally. Alpha redistribution half-life = 11 min; beta elimination = 2.5 hrs. — Barash Clinical Anesthesia, 9e
Mechanism of Action
Ketamine's neuropharmacology is complex and multi-receptor:
1. Primary: NMDA Receptor Antagonism
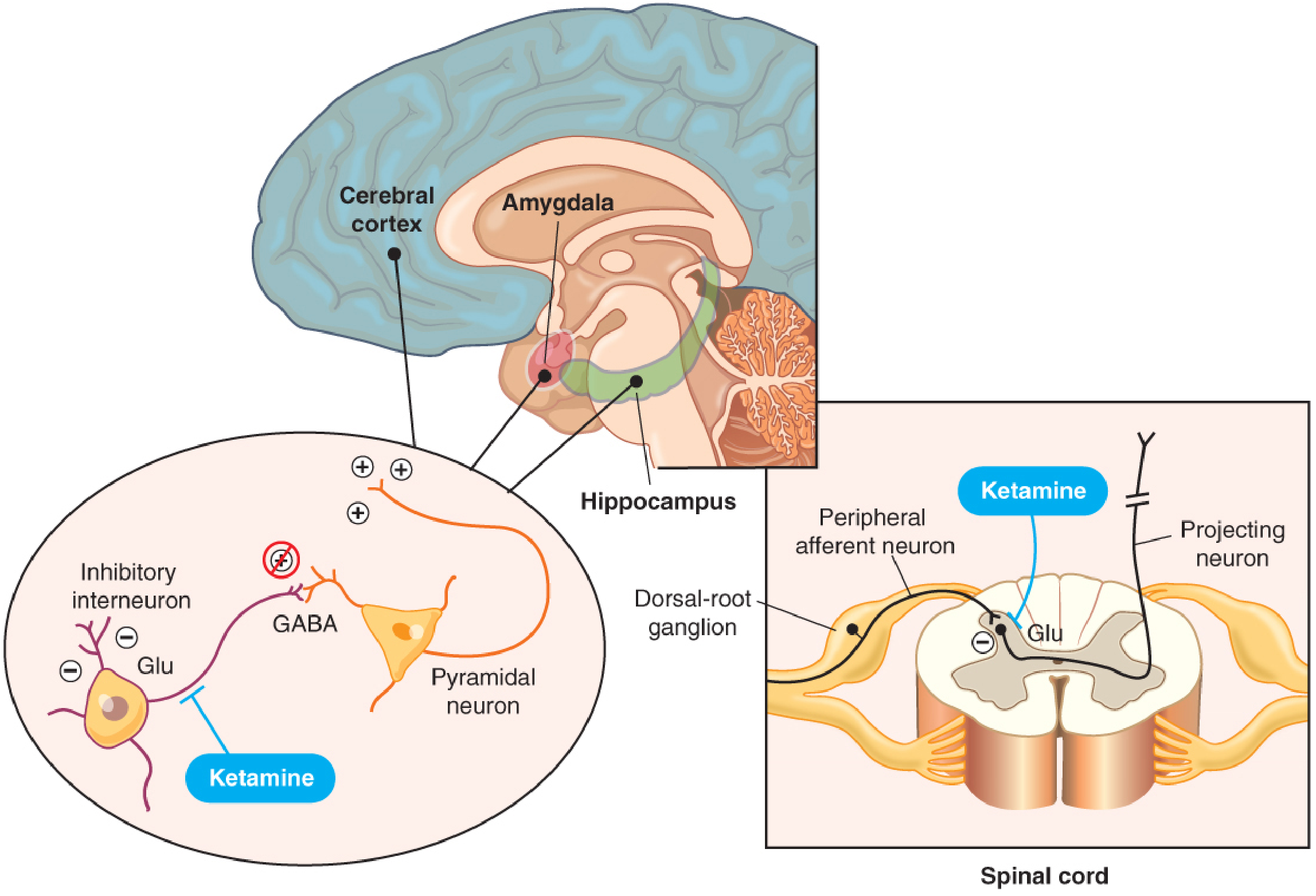
Ketamine acts as a noncompetitive NMDA (N-methyl-D-aspartate) receptor antagonist — binding to the PCP binding site within the NMDA ion channel, decreasing channel opening time. This antagonism is more profound when the channel has been previously opened by glutamate ("open-channel block"). — Barash Clinical Anesthesia, 9e
Preferential binding sites:
- Inhibitory GABA interneurons in the cortex, amygdala, and hippocampus → loss of inhibitory control → uncoordinated neuronal hyperactivity → unconsciousness
- NMDA receptors on dorsal horn neurons (spinal cord) → blocks nociceptive glutamate signals from peripheral afferent neurons → profound analgesia
This produces a functional dissociation between the thalamocortical and limbic systems, suppressing thalamocortical pathways while activating the limbic system — the basis of dissociative anesthesia.
2. Additional Receptor Interactions
| Receptor | Effect |
|---|---|
| Opioid receptors (μ, δ, κ) | Weak binding; does not fully account for analgesia |
| Noradrenergic neurons | Stimulation + catecholamine reuptake inhibition → hyperadrenergic state (↑NE, DA, serotonin) → contributes to hypnosis, analgesia, cardiovascular stimulation |
| Cholinergic/muscarinic | Anticholinergic physostigmine can reverse hypnotic effects |
| Sigma receptors | Contributes to psychomimetic effects |
3. Anti-Wind-up Effect
Ketamine prevents central sensitization and wind-up (amplification of repeated nociceptive NMDA stimulation) — the basis of its anti-hyperalgesic and opioid-sparing effects. — Miller's Anesthesia, 10e
Clinical Uses
1. Induction and Maintenance of Anesthesia
Ketamine produces a trance-like cataleptic state: patients are unconscious with eyes open, maintain spontaneous respiration, and do not react to noxious stimuli. EEG shows active/epileptiform patterns (not clinical seizures).
Advantages for induction:
- Cardiovascular stimulation (↑HR, ↑BP, ↑CO) → ideal for hemodynamically unstable patients, trauma, hypovolemic shock
- No adrenal suppression (unlike etomidate controversy)
- Preserves pharyngeal and laryngeal reflexes + respiratory drive → safer when airway manipulation is undesirable
- Bronchodilator — reduces airway resistance; suitable for asthmatic patients
- Can be given IM → useful in uncooperative/combative patients or field settings
Disadvantages: Raises ICP via ↑CBF and ↑CMR; however, systematic reviews confirm ketamine does not increase ICP in ventilated patients receiving adjunctive sedatives. — Miller's Anesthesia, 10e
2. Procedural Sedation
Widely used in emergency medicine and pediatrics for painful procedures (fracture reduction, wound care, burn dressing changes) due to rapid onset, preserved airway reflexes, and IM route availability. — Barash Clinical Anesthesia, 9e
3. Analgesia
- Acute postoperative pain: Sub-anesthetic doses (0.1–0.5 mg/kg) reduce pain scores and decrease opioid requirements. Most effective when given as a pre-incision bolus + postoperative infusion.
- Chronic pain (CRPS, cancer pain): Decreases pain scores and opioid consumption, though effects are time-limited.
- Intranasal ketamine: Reduces breakthrough pain in chronic/neuropathic pain — comparable to morphine PCA after spine surgery when combined with intranasal midazolam.
4. Treatment-Resistant Depression (TRD)
Ketamine produces rapid antidepressant effects within 1 hour, including reduction in suicidal ideation. Duration lasts days to ~2 weeks after a single infusion. Administered IV at 0.5 mg/kg over 40 minutes (sub-anesthetic). Esketamine (Spravato®) nasal spray is FDA-approved for TRD under supervised administration. — Goodman & Gilman's, 14e
5. Refractory Status Epilepticus
Ketamine is of substantial benefit — provides seizure control despite its proconvulsant potential at sub-anesthetic levels. — Miller's Anesthesia, 10e
6. Bronchospasm / Asthma
Ketamine's bronchodilatory properties (via catecholamine release and direct smooth muscle relaxation) make it the induction agent of choice in status asthmaticus requiring intubation.
Adverse Effects
| System | Effect |
|---|---|
| CNS | Emergence delirium/reaction, hallucinations, bizarre vivid dreams, mood alteration, nystagmus, dose-dependent ↑CMR and ↑CBF |
| Cardiovascular | ↑HR, ↑BP, ↑PVR (via catecholamine release) — problematic in coronary artery disease, severe right heart failure; direct myocardial depression if catecholamine reserves depleted (e.g., prolonged critical illness) |
| Psychiatric | Psychomimetic effects, dissociative experiences; risk of precipitating psychosis in susceptible individuals; used illicitly as a club drug ("Special K") due to amnesia and hallucinogenic properties |
| GI | Nausea and vomiting (especially at high doses) |
| Secretions | Hypersalivation, bronchial secretions (co-administer antisialagogue, e.g., atropine or glycopyrrolate) |
| ICP | Increases ICP in awake, non-ventilated patients with intracranial pathology — use cautiously as sole agent; safe when combined with benzodiazepines, propofol, or isoflurane |
| Tolerance/dependence | Tolerance develops with long-term use (especially in burn patients); abuse potential — esketamine must be administered under healthcare supervision |
| Emergence reaction | Agitation, delirium, hallucinations during recovery (more common in adults, with large doses, without premedication) — attenuated by pre-/co-administration of benzodiazepines |
Drug interactions: CNS depressants (alcohol, benzodiazepines, barbiturates) potentiate sedation. MAOIs, stimulants, and sympathomimetics can cause dangerous ↑BP and ↑HR. — Katzung's Basic and Clinical Pharmacology, 16e
Contraindications / Caution
- Uncontrolled hypertension or severe coronary artery disease
- Patients with known adverse (psychiatric) reactions to ketamine
- Open globe injury (raises intraocular pressure)
- Intracranial hypertension when used as sole agent without concomitant sedation
- Schizophrenia or psychosis-prone individuals
Recent evidence update: A 2025 systematic review (PMID 40767004) confirms ketamine's expanding therapeutic role beyond anesthesia — particularly in chronic pain and psychiatric disorders — consistent with the above library content.
Sources: Barash Clinical Anesthesia 9e | Miller's Anesthesia 10e | Goodman & Gilman's Pharmacological Basis of Therapeutics 14e | Katzung's Basic and Clinical Pharmacology 16e | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.