hodgkins lymphoma
Reading File
Finding Sources
Searching PubMed
"Hodgkin lymphoma"[MeSH Terms] AND treatment
Reading File
Reading File
Searching PubMed
"Hodgkin lymphoma"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have very comprehensive content from both textbooks. Let me compose the full answer.
Hodgkin Lymphoma
Definition & Overview
Hodgkin lymphoma (HL) is a B-cell lymphoma characterized by the presence of distinctive neoplastic Reed-Sternberg (RS) cells within an inflammatory background. It is divided into two major types:
- Classic Hodgkin Lymphoma (cHL) - ~90% of cases
- Nodular Lymphocyte-Predominant HL (NLPHL) - ~10% of cases
A hallmark feature is that tumor cells (RS cells) make up only a small fraction of the tumor mass; the bulk is a reactive inflammatory infiltrate. HL typically arises in a single lymph node or chain, then spreads in a stepwise, contiguous fashion to adjacent nodes.
- Robbins & Kumar Basic Pathology, p. 416
- Goldman-Cecil Medicine, Ch. 172
Epidemiology
- ~30,000 new cases/year in North America and Europe
- Age-adjusted incidence: ~2.7 per 100,000; mortality: 0.5 per 100,000
- Bimodal age distribution: early peak at ages 25-30 years, second peak >50 years
- Slightly more common in males; more frequent in Whites than Blacks; rare in Asian populations
- Cumulative lifetime risk: ~1 in 250-300 in North America
- In the Indian subcontinent, the age distribution is strongly shifted toward childhood
Etiology & Pathogenesis
EBV is the leading suspected causative agent:
- A history of infectious mononucleosis increases the likelihood of subsequent HL three-fold
- EBV is present in RS cells in up to 70% of mixed-cellularity cases and a smaller fraction of other cHL subtypes
- The integration site is identical in all RS cells in a given case (clonal), indicating infection precedes transformation
Cell of origin: Elegant microdissection studies revealed that every RS cell in a given case has the same immunoglobulin gene rearrangements with somatic hypermutation - confirming origin from germinal center B cells.
Immune evasion mechanisms:
- RS cells express high levels of PD-L1 and PD-L2 (chromosome 9p amplification), suppressing T-cell responses - this explains the remarkable efficacy of anti-PD-1 antibodies
- Loss of β2-microglobulin - failure to express class I MHC
- Secretion of immunosuppressive cytokines (IL-13 autocrine, TGF-β fibrogenic, IL-5 for eosinophil recruitment)
Morphology: Reed-Sternberg Cells
The Reed-Sternberg (RS) cell is the sine qua non of HL:
- Very large cell (15-45 μm in diameter)
- Enormous multilobate nucleus with exceptionally prominent nucleoli
- The classic "owl-eye" appearance: two mirror-image nuclei/lobes, each with a large acidophilic inclusion-like nucleolus surrounded by a clear halo
- Immunophenotype: CD15+, CD30+, CD45-, B-cell markers-, T-cell markers-
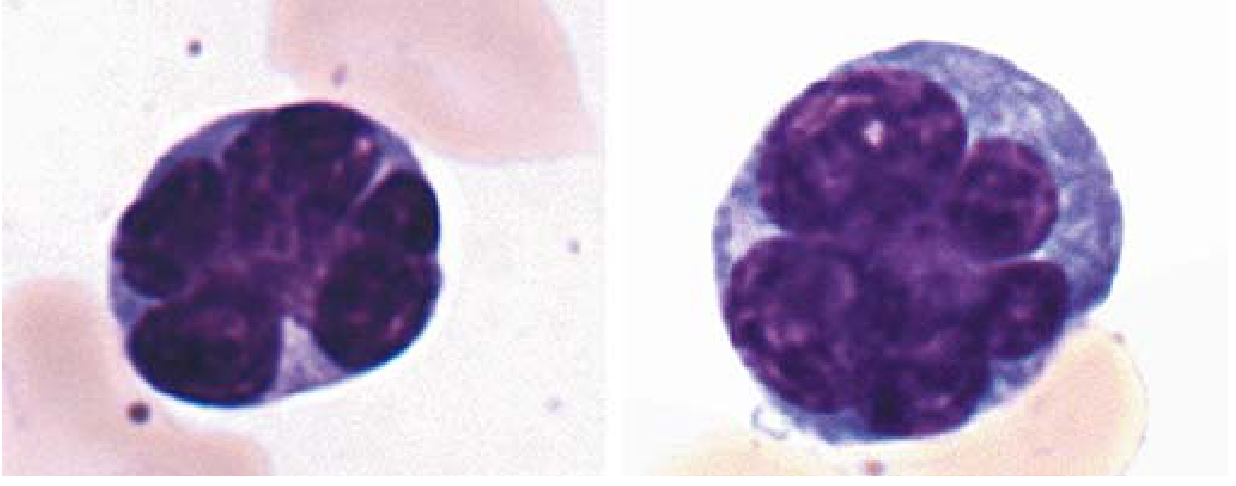
Classic RS cells with multilobed nuclei (Robbins & Kumar Basic Pathology, p. 418)
Classification: Five Subtypes
| Subtype | Frequency | Key Features |
|---|---|---|
| Nodular Sclerosis | Most common | Lacunar RS variant; collagen bands; young adults; mediastinal/supraclavicular; equal M:F; excellent prognosis |
| Mixed Cellularity | Second most common | Classic owl-eye RS cells; highest EBV association (70%); older adults; more advanced stage at presentation |
| Lymphocyte Rich | Uncommon | RS cells rare; predominantly lymphocytes; best prognosis |
| Lymphocyte Depletion | Rare | Most RS cells; fibrosis or diffuse sheets; worst prognosis; HIV-associated |
| Nodular Lymphocyte Predominant | ~10% | "Popcorn" (lymphocytic & histiocytic) RS variant; CD20+, CD15-, CD30-; germinal center B-cell markers |
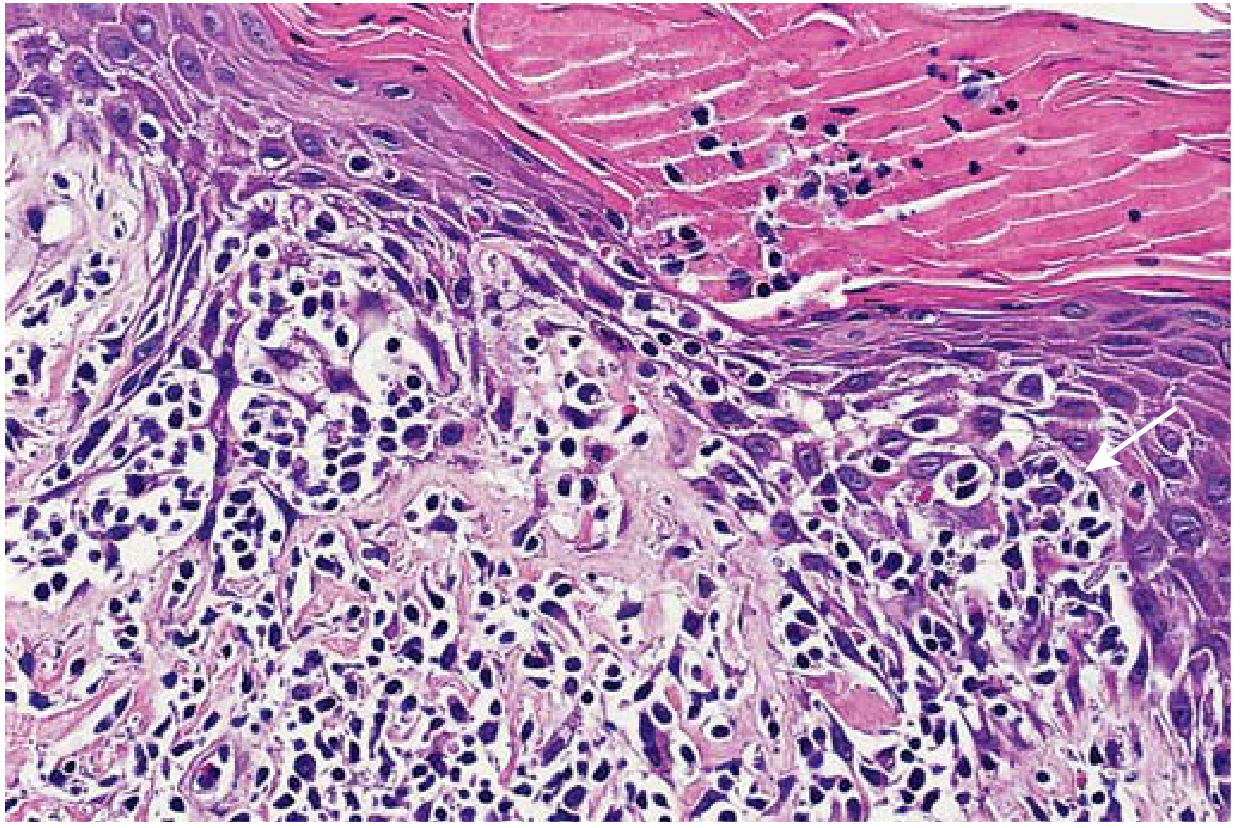
Nodular sclerosis HL: cellular nodules divided by dense collagen bands (Robbins & Kumar Basic Pathology)
Clinical Features
Classic presentation: Painless enlargement of one or more peripheral lymph node groups
- Most common: cervical, supraclavicular, and mediastinal nodes
- Mediastinal widening on CXR is common - especially in nodular sclerosis
- Contiguous spread distinguishes HL from NHL
B symptoms (present in ~30-40% of patients, signifying systemic disease):
- Unexplained fever >38°C (recurrent)
- Drenching night sweats
- Unexplained weight loss >10% of body weight in 6 months
Alcohol-induced pain at sites of disease - a curious but pathognomonic feature
Pel-Ebstein fever: cyclical fevers (days of fever alternating with afebrile periods) - classic but uncommon
Pruritis - generalized, sometimes severe
Staging: Ann Arbor System (Cotswold Modification)
| Stage | Definition |
|---|---|
| I | Single lymph node region or single extralymphatic site (IE) |
| II | Two or more regions on the same side of the diaphragm; IIe = limited extranodal extension |
| III | Node regions on both sides of the diaphragm; IIIs = splenic involvement |
| IV | Diffuse extralymphatic involvement (bone marrow, lung, bone, liver) |
Suffix A = no B symptoms; Suffix B = B symptoms present
Bulky disease: any mass ≥10 cm in largest diameter
Work-up & Staging Evaluation
- Complete history and physical examination (search for B symptoms, lymphadenopathy, organomegaly)
- CBC, ESR, LFTs, creatinine, albumin, serum protein electrophoresis
- Serology: HIV, Hepatitis B and C
- CT scan (neck, thorax, abdomen, pelvis) with contrast, slices ≤1 cm
- FDG-PET/CT - now mandatory for staging and response assessment; has replaced bone marrow biopsy for staging (more sensitive for detecting BM involvement)
- Excisional lymph node biopsy for diagnosis
Treatment
Limited-Stage Disease (Stage I-II, non-bulky)
- ABVD chemotherapy × 2 cycles + involved-field radiotherapy (ISRT)
- Cure rates >90-95% for nonbulky stage IA/IIA
- Interim PET/CT guides whether radiation is needed
Advanced-Stage Disease (Stage III-IV or bulky)
- ABVD × 6 cycles (standard) or escalated BEACOPP (more toxic, higher early CR rate)
- PET-adapted therapy allows de-escalation in PET-negative responders
- Cure rates ~75-80%
ABVD regimen: Doxorubicin (Adriamycin) + Bleomycin + Vinblastine + Dacarbazine
BEACOPP (escalated): Bleomycin + Etoposide + Adriamycin + Cyclophosphamide + Vincristine (Oncovin) + Procarbazine + Prednisone
Relapsed/Refractory Disease
- Salvage chemotherapy (e.g., ICE, DHAP, GDP)
- High-dose chemoradiation (BEAM) + autologous hematopoietic cell transplantation (ASCT)
- ~33% of refractory and ~66% of relapsed patients can be cured with this approach
- Brentuximab vedotin (anti-CD30 antibody-drug conjugate) as post-ASCT consolidation - reduces relapses by ~1/3
- Checkpoint inhibitors (nivolumab, pembrolizumab - anti-PD-1): >70% objective response rate in multiply relapsed disease; very effective given PD-L1 overexpression on RS cells
- CAR-T cells targeting CD30 - investigational
Late Complications of Treatment
| Complication | Notes |
|---|---|
| Secondary malignancies | Lung cancer, breast cancer (especially post-mantle field RT), NHL, AML/MDS |
| Cardiac disease | Coronary artery disease, cardiomyopathy (anthracyclines + mediastinal RT) |
| Pulmonary toxicity | Bleomycin-induced pneumonitis/fibrosis |
| Hypothyroidism | After neck/mediastinal RT; regular TSH monitoring required |
| Infertility | Gonadal damage from alkylating agents (BEACOPP > ABVD) |
| Dental caries | After oropharyngeal/neck irradiation |
| Relapse | 10-30% of patients; requires close follow-up |
Prognosis
HL is one of the most curable malignancies:
- Stage I-II: >90-95% cure
- Stage III-IV: ~75-80% long-term disease-free survival
- Patients event-free at 2 years have an excellent long-term outcome
- The major challenge is minimizing treatment toxicity while maintaining cure rates
The development of anti-PD-1 immunotherapy (exploiting the biology of PD-L1 overexpression on RS cells) represents a major advance, particularly for relapsed/refractory disease.
Sources: Robbins & Kumar Basic Pathology, pp. 416-419; Goldman-Cecil Medicine, Ch. 172 (Connors & Savage); Cummings Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.