Epidural hemorrhage
Reading File
Finding Sources
Finding Sources
Searching PubMed
"epidural hematoma"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive, well-sourced content from multiple top textbooks and key images. Let me compose the full answer.
Epidural Hemorrhage (Epidural Hematoma)
Definition and Anatomy
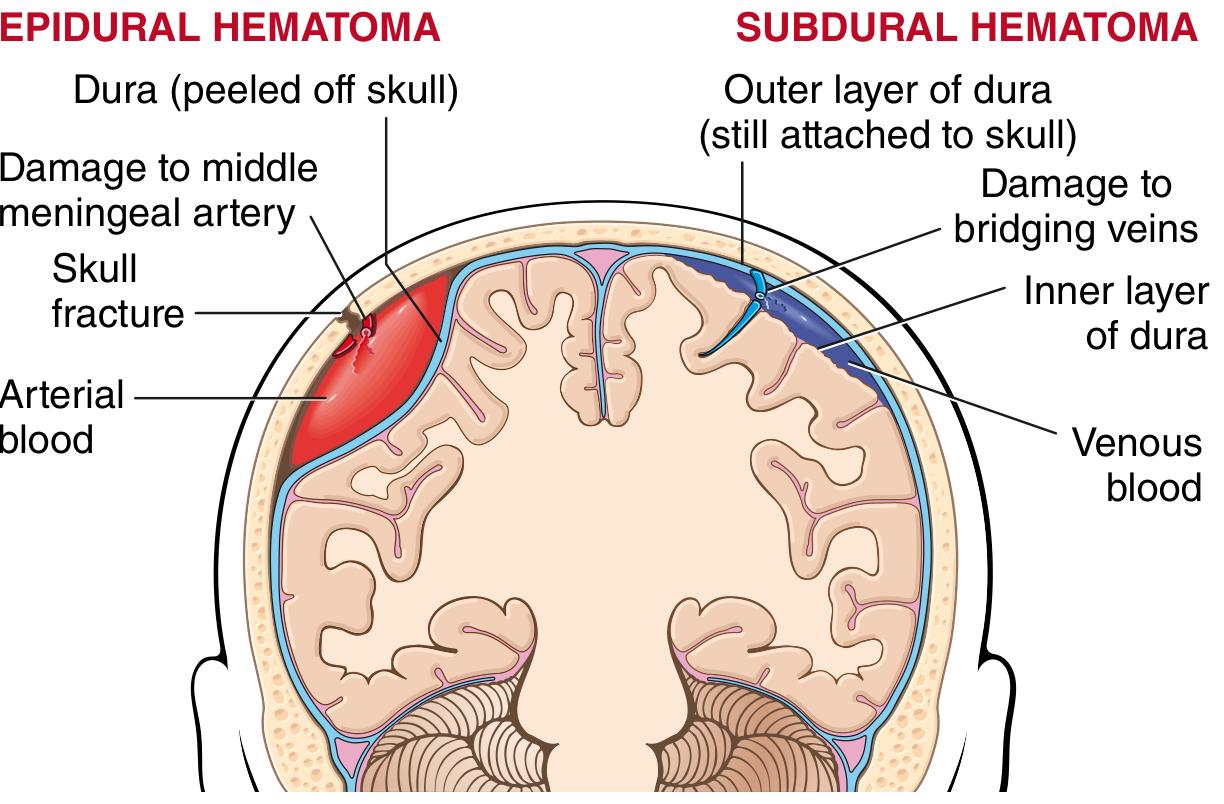
An epidural hematoma (EDH) is a collection of blood in the potential space between the skull and the dura mater. Because the outer layer of the dura normally serves as the periosteum of the inner skull table, this space does not exist under normal conditions - it forms only when a vessel bleeds with enough pressure to strip the dura away from the bone.
Etiology and Mechanism
Primary cause: Blunt trauma - most commonly to the temporal or temporoparietal region - causing a skull fracture that crosses the groove of the middle meningeal artery, lacerating it. The resulting high-pressure arterial bleeding strips the dura from the periosteum, creating an expanding hematoma.
- Most common location: lateral temporal region (middle meningeal artery territory)
- Less commonly: parieto-occipital region or posterior fossa, where a venous sinus tear is more likely
- In children: the skull is deformable, so temporary displacement can lacerate a vessel even without a fracture
Less common causes:
- Laceration of a dural venous sinus (bleeds more slowly; course may resemble subdural hematoma)
- Eosinophilic granuloma, metastatic skull/dural tumors (e.g., hepatocellular carcinoma), or craniofacial infections such as sinusitis
- Robbins & Cotran Pathologic Basis of Disease, p. 1162
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 245-246
Classic Clinical Presentation
The "textbook" triad is:
- Significant head trauma (often to thin temporal bone - baseball, pool cue, fall)
- Brief loss of consciousness or altered sensorium
- A lucid interval (minutes to hours) followed by rapid neurologic deterioration
However, this classic triad occurs in only 15-20% of patients ("talk and die" patients). The majority (~70%) are picked up on CT with minimal or no loss of consciousness. About half of pediatric cases involve a fall of less than 0.5 meters.
Symptoms of expansion:
- Headache of increasing severity
- Vomiting, drowsiness, confusion
- Seizures (sometimes focal/unilateral)
- Hemiparesis with hyperreflexia and Babinski sign
- Ipsilateral pupil dilation (third nerve compression from uncal herniation)
- Cushing response: rising systolic BP + bradycardia
- As coma deepens: bilateral spasticity, decerebrate rigidity
Signs of basal skull fracture to look for (since the fracture often involves the skull base):
- Battle's sign (post-auricular ecchymosis)
- Raccoon eyes (periorbital ecchymosis)
- Hemotympanum
- Tintinalli's Emergency Medicine, p. 1732
- Plum and Posner, p. 246-247
Imaging
CT Scan (modality of choice)
- Appears as a biconvex (lens-shaped / football-shaped) hyperdense mass between the skull and brain, typically in the temporal region
- Convex on both surfaces - this distinguishes it from subdural hematoma, which is concave on the brain-facing surface
- Look for an associated skull fracture crossing the middle meningeal groove on bone windows
- A vertex hematoma can be missed on axial cuts - coronal reconstructions are needed
- MRI is not required for EDH diagnosis but may be needed to assess underlying contusions and edema

CT demonstrating the characteristic biconvex shape and focal location of an epidural hematoma - Tintinalli's Emergency Medicine
- Plum and Posner, p. 247
- Tintinalli's Emergency Medicine, p. 1732
Pathophysiology of Deterioration
High-pressure arterial bleeding does not tamponade easily, so blood continues to accumulate. The expanding hematoma:
- Compresses the underlying temporal lobe
- Stretches and tears pain-sensitive meninges and vessels at the middle fossa base (headache)
- Causes uncal herniation - ipsilateral pupil dilation (CN III compression) followed by complete ophthalmoparesis
- Compresses the midbrain - bilateral Babinski signs, spasticity
- Ultimately: respiratory arrest if not evacuated
Herniation can occur within hours of injury - this is the key reason EDH is a neurosurgical emergency.
- Robbins & Cotran, p. 1162
- Adams and Victor's Principles of Neurology, p. (Ch. 34)
Treatment
Surgical (definitive)
Emergency surgical evacuation is the treatment for any EDH causing brain displacement or impairment of consciousness. Options:
- Craniotomy (preferred) with drainage of the hematoma and ligation of the bleeding vessel
- Burr holes in emergency situations when craniotomy is not immediately possible
Prognosis is excellent when surgery is performed promptly, because the underlying brain parenchyma is often uninjured. Even approximately one-third of patients with a fixed, dilated pupil preoperatively can achieve a good recovery with prompt surgery.
Factors determining outcome:
- Time from injury to surgical evacuation (most important)
- Age
- Depth of coma
- Degree of midline shift
- Hematoma size
If coma, bilateral Babinski signs, decerebrate rigidity, or bilateral spasticity have already supervened before operation, it indicates midbrain compression has occurred; prognosis is less favorable but not hopeless.
Conservative management
Small epidural hemorrhages without neurologic symptoms or signs can be managed conservatively with serial CT scanning and close clinical surveillance. Many small clots enlarge gradually over 1-2 weeks and are then absorbed. However, even "mild" cases require careful follow-up, as occasionally hematoma development is delayed.
Patients with a negative initial CT should be cautioned to remain under observation of a family member for 24 hours, with instructions to return immediately if they cannot be awakened.
- Adams and Victor's Principles of Neurology, treatment section (Ch. 34)
- Plum and Posner, p. 247
Key Comparisons: EDH vs. Subdural Hematoma
| Feature | Epidural Hematoma | Subdural Hematoma |
|---|---|---|
| Bleeding source | Middle meningeal artery (arterial) | Bridging veins (venous) |
| Location | Between skull and dura | Between dura and arachnoid |
| CT shape | Biconvex (lens-shaped) | Concave (crescent-shaped) |
| Speed of onset | Rapid (hours) | Variable (acute to chronic) |
| Lucid interval | Classic (but minority) | Less typical |
| Brain injury | Often absent | Often concurrent contusion |
| Skull fracture | Usually present | Less common |
| Prognosis with Rx | Excellent if early | More variable |
Summary
Epidural hemorrhage is an arterial neurosurgical emergency caused most often by middle meningeal artery laceration from temporal skull fracture. The classic lucid-interval presentation is seen in a minority; most cases are now detected on CT with mild or no symptoms. The hallmark CT finding is a biconvex hyperdense mass, typically temporal. Prompt surgical evacuation is life-saving and yields excellent outcomes when performed before uncal herniation is complete. Small, asymptomatic hematomas may be observed with serial imaging.
When uncal herniation occurs initially does it compress the ipsilateral cerebellar peduncle?
Finding Sources
Reading File
Reading File
Great detail from both sources. Here is the full answer:
Uncal Herniation: Which Structure Gets Compressed?
No - the initial compression is not of the cerebellar peduncle. The uncus herniates downward through the tentorial notch (incisura), not toward the posterior fossa. The structures it compresses are in the midbrain, not the cerebellum.
Here is the sequence:
1. First: Ipsilateral CN III (oculomotor nerve)
The dorsal surface of the oculomotor nerve lies very close to the medial edge of the temporal lobe. This is why the earliest sign of uncal herniation is ipsilateral pupil dilation - the parasympathetic pupilloconstrictor fibers travel on the outside of CN III and are compressed first, even before consciousness changes. The pupil may initially respond sluggishly, then progressively dilates and becomes fixed and nonreactive.
2. Then: Ipsilateral cerebral peduncle
As herniation advances, the herniating uncus compresses the ipsilateral cerebral peduncle against the tentorial edge. The cerebral peduncles are the descending corticospinal tracts in the midbrain. This compression produces contralateral hemiparesis (corticospinal fibers haven't yet crossed at this level).
"Contralateral hemiparesis develops as the ipsilateral peduncle is compressed against the tentorium."
- Rosen's Emergency Medicine, p. 373
3. Kernohan Notch - the "false-localizing" exception
In a minority of cases, the herniation pushes the opposite (contralateral) cerebral peduncle against the far edge of the tentorial hiatus. This produces ipsilateral hemiparesis - weakness on the same side as the dilated pupil and the mass lesion. This is Kernohan notch syndrome, a false-localizing sign that can mislead the clinician into thinking the lesion is on the wrong side.
4. Late: Full midbrain compression
With continued herniation, direct brainstem compression produces:
- Bilateral decerebrate posturing
- Sustained hyperventilation
- Hemodynamic instability
- Coma, and ultimately brainstem failure
Summary Table
| Stage | Structure Compressed | Clinical Sign |
|---|---|---|
| Early | Ipsilateral CN III | Ipsilateral sluggish then dilated, fixed pupil |
| Intermediate | Ipsilateral cerebral peduncle | Contralateral hemiparesis, Babinski |
| Kernohan notch variant | Contralateral cerebral peduncle | Ipsilateral (false-localizing) hemiparesis |
| Late | Full midbrain / brainstem | Bilateral decerebration, coma, respiratory arrest |
The cerebellar peduncles are not involved in uncal (transtentorial) herniation. Cerebellar peduncle compression would occur in a different context - e.g., a posterior fossa mass directly compressing the brainstem, or tonsillar herniation through the foramen magnum.
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, pp. 216-218
- Rosen's Emergency Medicine, p. 373
This is a shared conversation. Sign in to Orris to start your own chat.