Explain osteoarthritis in detaill...investigation clinical examination,, diagnosis, radology...differentiatte it wih rheumatoid arthritis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the full detailed answer.
Osteoarthritis: A Comprehensive Review
1. Definition
Osteoarthritis (OA), also called degenerative joint disease, is characterized by failed repair of synovial joint tissues after intra-articular stress. The resulting breakdown of cartilage and bone leads to symptoms of pain, stiffness, and functional disability. Although the term "osteoarthritis" implies an inflammatory disease, it is primarily a degenerative disorder of articular cartilage, with inflammation acting as a secondary contributor.
- Goldman-Cecil Medicine - OA is the most common disease of joints, affecting over 50 million people worldwide.
- Robbins & Kumar Basic Pathology, p. 790
2. Classification
| Type | Features |
|---|---|
| Primary (Idiopathic) | No apparent cause; an aging phenomenon. Affects few joints (oligoarticular). Typical distribution: knees, hips, lower lumbar/cervical spine, DIP/PIP joints, 1st CMC, 1st MTP |
| Secondary | Underlying cause identified. Single or multiple joints. Same radiological findings as primary |
Secondary causes (from Grainger & Allison's Diagnostic Radiology):
- Trauma (acute or chronic repetitive)
- Systemic metabolic: hemochromatosis, Wilson disease, ochronosis
- Endocrine: acromegaly, hypothyroidism, hyperparathyroidism, diabetes mellitus
- Crystal deposition: CPPD, gout
- Other: Paget disease, rheumatoid arthritis (burned out), bone/joint dysplasias
3. Epidemiology & Risk Factors
- Most common joint disease; prevalence increases exponentially after age 50 - ~40% of people >70 years are affected
- Women are disproportionately affected (especially hand OA and knee OA post-menopause)
- Primary OA has strong genetic predisposition; more common in women
- Risk factors: obesity (each pound lost has a multiplier unloading effect on both knees and hips), repetitive joint stress, prior trauma, muscle weakness, joint laxity
4. Pathogenesis
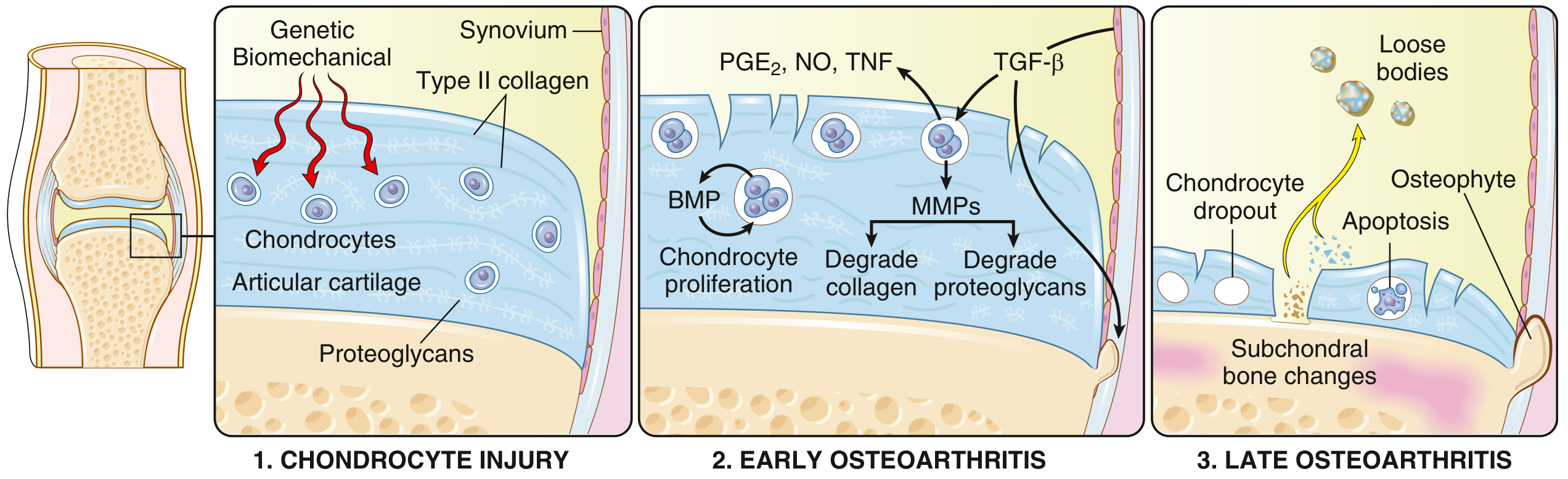
The principal mechanism is biomechanical stress leading to chondrocyte injury, with genetic predisposition (polymorphisms in matrix and signaling genes) as a modifier.
Sequence of Events:
Stage 1 - Chondrocyte Injury:
- Biomechanical stress damages chondrocytes
- Genetic and mechanical factors interact
- Type II collagen network disruption begins
Stage 2 - Early OA:
- Chondrocytes proliferate in response to matrix loss
- Secrete matrix metalloproteinases (MMPs) that degrade type II collagen
- Water content of matrix increases; proteoglycan concentration falls
- Cytokines involved: TGF-beta, IL-1, IL-6, TNF, PGE2, nitric oxide
- Horizontal collagen fibers cleave, producing surface fissures and clefts
Stage 3 - Late OA:
-
Chondrocyte dropout and apoptosis
-
Full-thickness cartilage sloughing
-
Dislodged pieces form loose bodies ("joint mice")
-
Exposed subchondral bone is burnished by friction - polished ivory appearance = bone eburnation
-
Microfractures allow synovial fluid into subchondral regions (ball-valve mechanism) → subchondral cysts
-
Marginal osteophytes form (new cartilage outgrowths that ossify via neurovasular invasion, driven by BMP and TGF-beta)
-
Synovium becomes edematous with scattered chronic inflammatory cells (mild, unlike RA)
-
Capsule stretches, becomes edematous and may become fibrotic
-
Robbins & Kumar Basic Pathology, p. 790-791; Harrison's Principles of Internal Medicine 22E, p. 2995-2996
5. Clinical Features
5A. Symptoms (History)
| Symptom | Detail |
|---|---|
| Joint pain | Activity-related early in disease; comes on during/just after use, gradually resolves. Becomes continuous and nocturnal in advanced disease |
| Morning stiffness | Present but brief - <30 minutes (key distinguishing feature from RA where it is >1 hour) |
| Crepitus | Felt and heard on joint movement |
| Limitation of range of motion | Progressive |
| Buckling/giving way | Especially knees (from quadriceps weakness) |
| Locking | Suggests loose bodies |
- Pain in weight-bearing joints when walking, stair climbing, arising from chair
- Knee pain on stair climbing often indicates patellofemoral compartment involvement (not actively articulating until knee is flexed ~35°)
- Episodic early, triggered by overuse; becomes constant later as central and peripheral sensitization develops
- Spinal osteophytes can compress nerve roots causing radicular pain, muscle spasms, atrophy, and neurological deficits
5B. Joints Commonly Involved
- Hips, knees (most common weight-bearing joints)
- Lower lumbar and cervical vertebrae
- DIP joints (Heberden nodes) and PIP joints (Bouchard nodes) of fingers - more common in women
- 1st carpometacarpal (CMC) joint (thumb base)
- 1st metatarsophalangeal (MTP) joint
5C. Physical Examination Findings
| Sign | Detail |
|---|---|
| Bony enlargement | Firm, non-tender swelling from osteophytes (Heberden/Bouchard nodes at DIP/PIP) |
| Crepitus | Audible/palpable on passive motion |
| Restricted range of motion | Loss of internal rotation of hip on passive movement is a key early sign |
| Joint-line tenderness | Tenderness directly over the joint line (vs. outside it in bursitis) |
| Varus/valgus deformity | In knee OA (medial or lateral compartment predominantly affected) |
| Joint effusion | Small to moderate; non-inflammatory fluid |
| Muscle wasting | Disuse atrophy around affected joint |
| No warmth/redness | Absent or minimal, unlike RA |
| 'Grip and grind' test | For elbow OA - crepitus over radiocapitellar joint on rotation with fist clenched |
Key point: Joint deformity may develop, but joint fusion (ankylosis) does not occur in OA (unlike RA).
6. Investigations
6A. Blood Tests
"No blood tests are routinely indicated for workup of patients with OA unless symptoms and signs suggest inflammatory arthritis." - Harrison's Principles of Internal Medicine 22E
| Test | Expected Result in OA |
|---|---|
| ESR / CRP | Normal or mildly elevated |
| Rheumatoid Factor (RF) | Negative |
| ACPA (anti-CCP) | Negative |
| ANA | Negative |
| Serum uric acid | Normal (unless concomitant gout) |
| FBC / metabolic panel | Usually normal |
| No serum antibodies | Characteristic feature of OA |
Blood tests are ordered mainly to exclude inflammatory arthritis (RA, gout, pseudogout, lupus).
6B. Synovial Fluid Analysis
This is more helpful diagnostically than an X-ray:
| Parameter | OA | Inflammatory Arthritis |
|---|---|---|
| Appearance | Clear, viscous, yellow | Turbid, thin |
| WBC count | <1000 /µL (non-inflammatory) | >2000 /µL (often >50,000 in septic) |
| Crystals | None (or CPPD in late disease) | Present in gout/pseudogout |
| Glucose | Normal | May be low in septic |
- WBC >1000/µL suggests inflammatory arthritis or gout/pseudogout (identified by crystals)
- Harrison's Principles 22E, p. 2996
6C. Radiology
Plain Radiography (X-ray) - Primary Imaging Tool
X-rays are not indicated routinely in early OA. They are ordered when:
- Joint pain and physical findings are atypical for OA
- Pain persists after treatment
- Surgical planning is needed
Classic X-ray findings in OA (mnemonic: JOSS):
| Feature | Description |
|---|---|
| J - Joint space narrowing | Asymmetric (affects loaded compartment first), from cartilage loss |
| O - Osteophytes | Marginal bony outgrowths; most important hallmark |
| S - Subchondral sclerosis | Increased bone density beneath thinned cartilage (eburnation) |
| S - Subchondral cysts | Geode cysts from synovial fluid forced into bone |
Additional findings:
- Loose bodies ("joint mice")
- Joint deformity (varus/valgus)
- No periarticular osteoporosis (unlike RA)
- No marginal erosions (unlike RA)
Kellgren-Lawrence Grading (hips/knees):
- Grade 0: Normal
- Grade 1: Doubtful narrowing, possible osteophytic lipping
- Grade 2: Definite osteophytes, possible joint space narrowing
- Grade 3: Moderate narrowing, multiple osteophytes, sclerosis
- Grade 4: Severe narrowing, large osteophytes, marked sclerosis, deformity
Important: X-ray findings correlate poorly with pain severity - structural changes may be extensive without significant symptoms, and vice versa.
MRI
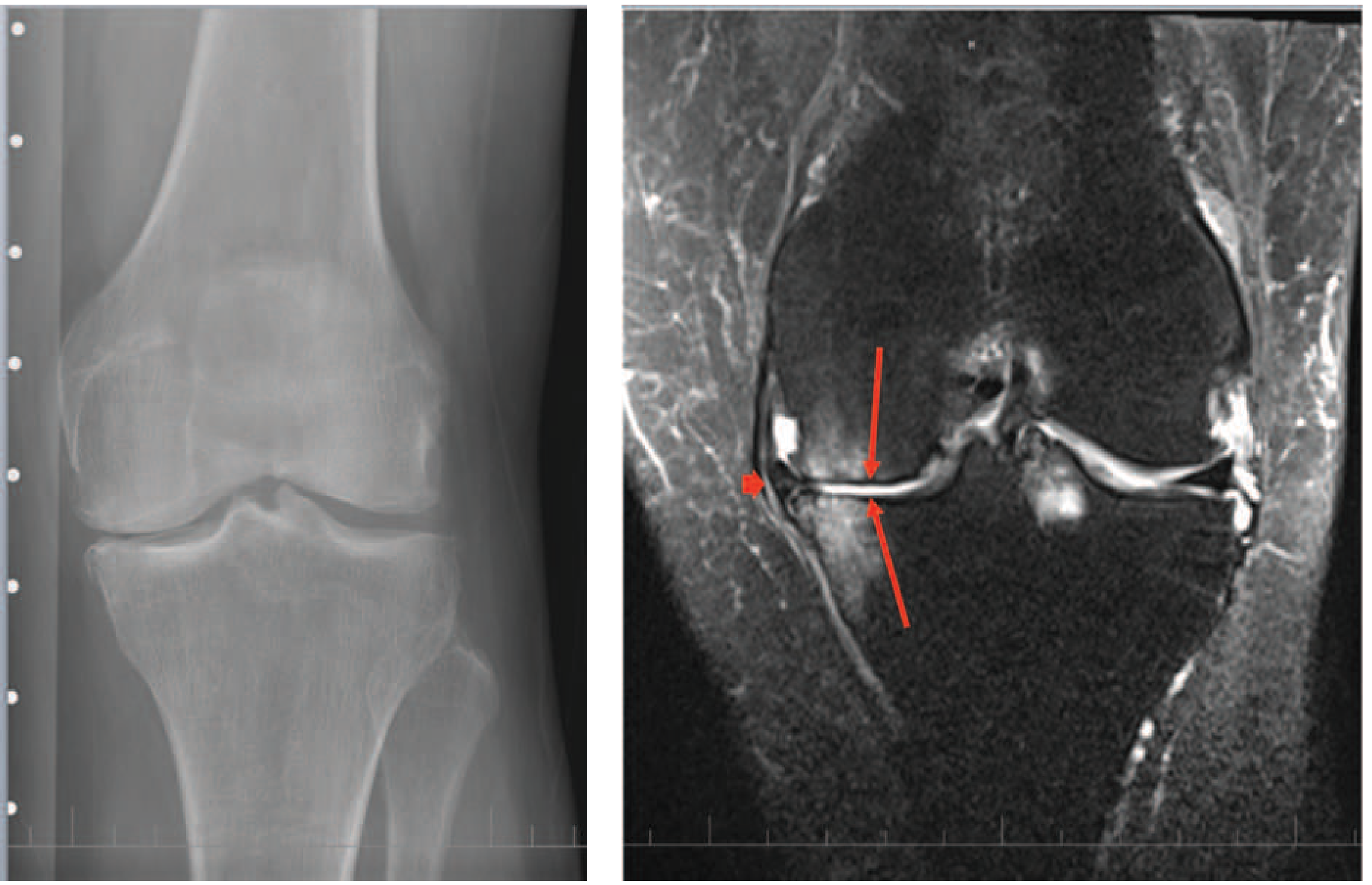
MRI is not routinely indicated for OA diagnosis. However, it detects:
- Cartilage loss (direct visualization)
- Bone marrow edema (evidence of bone injury/microcracks, correlates with pain)
- Meniscal tears and extrusion
- Synovial inflammation
- Subchondral cysts and bone lesions
- Osteophytes
MRI findings rarely warrant change in therapy - most findings (meniscal tears, cartilage lesions) are also common in painless older adults.
Ultrasound
- Useful for detecting joint effusion and synovitis
- Guides aspiration and injection
7. Diagnosis
OA is primarily a clinical diagnosis supported by imaging.
Diagnostic criteria (ACR Clinical Criteria for Knee OA):
- Age >50
- Morning stiffness <30 minutes
- Crepitus on active motion
- Bony tenderness
- Bony enlargement
- No palpable warmth
Key diagnostic approach:
- History + physical examination is sufficient in most patients with typical presentation
- Synovial fluid analysis if effusion present and inflammatory arthritis is considered
- X-rays for atypical presentations, treatment planning, or surgical assessment
8. Pathology (Gross and Histological)
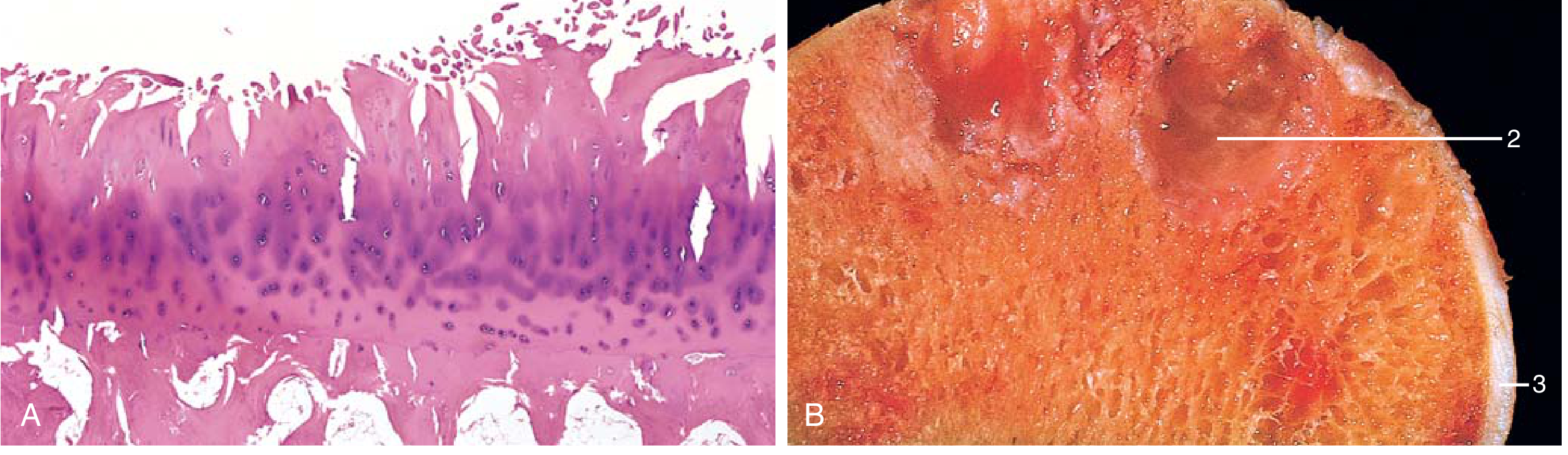
Histological features:
- Early: surface fibrillation and clefting of cartilage, chondrocyte proliferation (cloning), increased matrix water
- Late: full-thickness cartilage loss, chondrocyte dropout, bone eburnation (polished ivory appearance)
- Subchondral cysts (fibrous-walled geodes)
- Osteophytes at joint margins (fibrocartilage capped, gradually ossifying)
- Synovium: mildly congested, fibrotic, scattered chronic inflammatory cells only
9. Treatment Overview
Physical modalities (mainstay):
- Patient education and self-management
- Weight loss (each pound lost multiplies unloading across knees and hips)
- Exercise and muscle strengthening (quadriceps for knee OA)
- Avoiding pain-provocating activities
- Assistive devices: cane (opposite hand to affected joint), crutches, walkers
- Splinting (especially for 1st CMC joint)
Pharmacotherapy:
- Topical NSAIDs (first-line, especially in elderly)
- Oral NSAIDs (with GI protection)
- Intra-articular corticosteroids (short-term benefit)
- Duloxetine (centrally acting, for chronic pain)
- Paracetamol (limited evidence in OA vs. NSAIDs)
Surgical:
- Total joint replacement (TJR) - most effective for end-stage disease
- Arthroscopic debridement (limited indications)
- Osteotomy (selected cases to redistribute load)
10. Osteoarthritis vs. Rheumatoid Arthritis - Detailed Differential
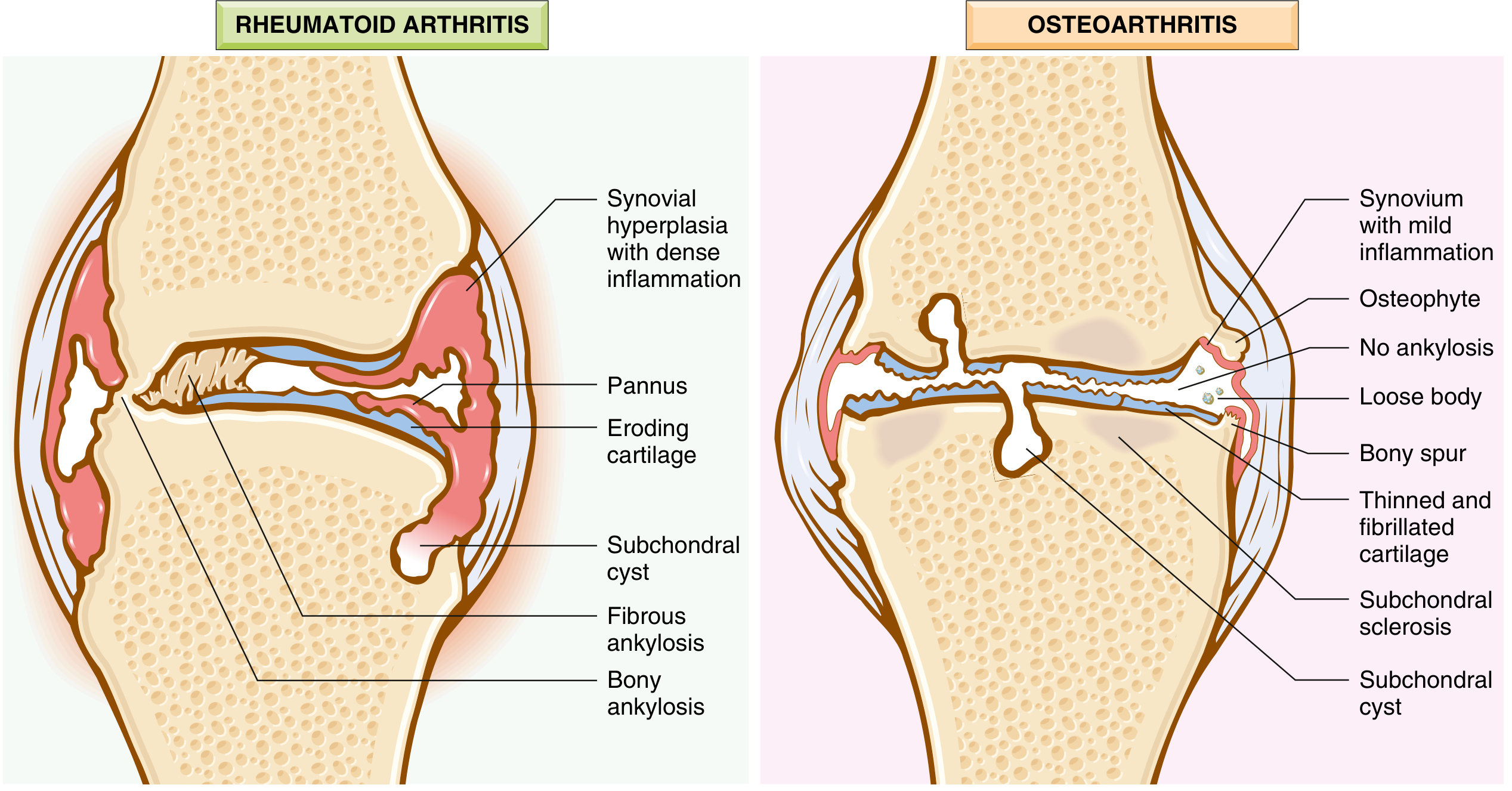
| Feature | Osteoarthritis | Rheumatoid Arthritis |
|---|---|---|
| Primary mechanism | Mechanical injury to articular cartilage | Autoimmunity (CD4+ T cell mediated) |
| Role of inflammation | Secondary; minimal | Primary and destructive |
| Age of onset | Typically >50 years | Any age; peak 3rd-5th decade |
| Sex predilection | Females > Males (especially hand/knee) | Females 3x more than males |
| Joints involved | Weight-bearing joints (knees, hips); DIP, 1st CMC, 1st MTP | Small joints first (MCP, PIP, wrists); symmetric; DIP rarely involved |
| Pattern | Asymmetric (may be bilateral but unequal) | Symmetric |
| Morning stiffness | <30 minutes | >1 hour (hallmark) |
| Systemic features | Absent | Present: fatigue, fever, weight loss, anemia |
| Joint swelling | Bony, firm (osteophytes) | Soft, boggy (synovial hypertrophy) |
| Warmth/redness | Absent or minimal | Present |
| Crepitus | Prominent | Less prominent |
| Heberden/Bouchard nodes | Present (DIP/PIP) | Absent at DIP |
| Swan neck / Boutonnière | Absent | Present (from pannus destroying tendons) |
| Ulnar drift | Absent | Present at MCPs |
| Rheumatoid nodules | Absent | Present (subcutaneous; forearms, elbows) |
| Extra-articular disease | Absent | Lungs (ILD, nodules), heart, vasculitis, eye |
| ESR/CRP | Normal/mildly elevated | Markedly elevated |
| Rheumatoid factor (RF) | Negative | Positive in ~80% |
| ACPA (anti-CCP) | Negative | Positive in ~70%; highly specific |
| Synovial fluid WBC | <1000/µL (non-inflammatory) | 2000-50,000+/µL (inflammatory) |
| X-ray: Joint space narrowing | Asymmetric (loaded compartment) | Symmetric, diffuse |
| X-ray: Osteophytes | Present (marginal) | Absent |
| X-ray: Erosions | Absent | Present (marginal/periarticular) |
| X-ray: Subchondral sclerosis | Present | Absent (osteoporosis instead) |
| X-ray: Periarticular osteoporosis | Absent | Present |
| X-ray: Ankylosis | Uncommon | Common (fibrous then bony) |
| X-ray: Soft tissue swelling | Less pronounced | Prominent periarticular |
| Pathology | Cartilage degeneration, osteophytes, subchondral cysts; minimal inflammation | Inflammatory pannus invading and destroying cartilage; severe chronic inflammation |
| Treatment approach | Physical therapy, NSAIDs, joint replacement | DMARDs (methotrexate), biologics (anti-TNF), steroids |
| Joint fusion | Does not occur | Occurs (fibrous then bony ankylosis) |
Sources: Robbins Table 19.2, p. 790; Bailey & Love Table 38.1, p. 565; Harrison's 22E
11. Sources
- Robbins & Kumar Basic Pathology, pp. 790-793
- Harrison's Principles of Internal Medicine 22E, Chapter 383, pp. 2994-2997
- Goldman-Cecil Medicine International Edition, Chapter 241
- Bailey & Love's Short Practice of Surgery 28th Ed, pp. 559, 565
- Grainger & Allison's Diagnostic Radiology, p. 1113
This is a shared conversation. Sign in to Orris to start your own chat.