How to treat hypoxic brain injury
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypoxic-ischemic brain injury" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have a comprehensive picture. Let me compile the full, well-structured answer.
Treatment of Hypoxic-Ischemic Brain Injury (HIBI)
Hypoxic-ischemic brain injury results from failure of oxygen delivery to the brain - either from hypotension/circulatory arrest (hypoxia-ischemia) or from respiratory failure/asphyxia alone. Causes include cardiac arrest, shock, asphyxiation, carbon monoxide poisoning, and cyanide poisoning. Consciousness is lost within seconds of circulatory arrest; if circulation is not restored within 3-5 minutes, permanent neurological damage often results.
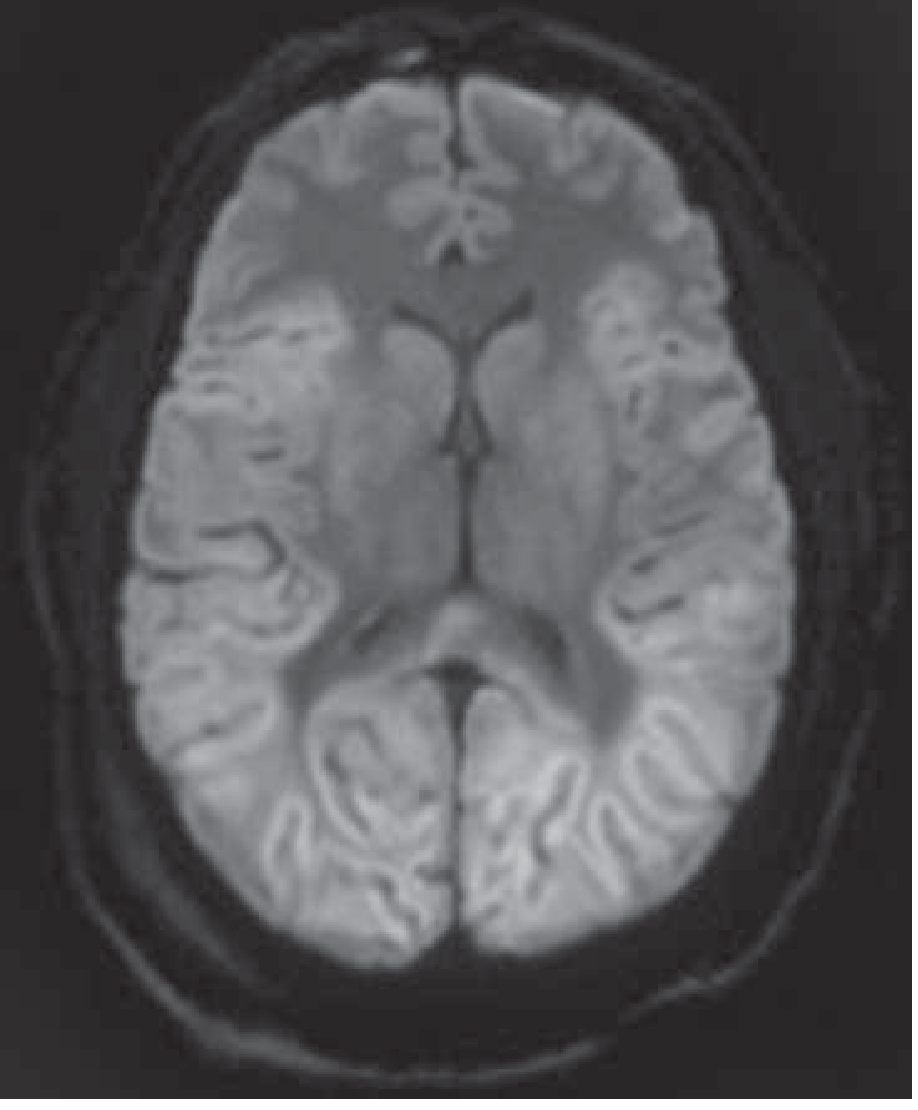
The DWI MRI below shows diffuse cortical injury following cardiac arrest - bright signal throughout the cortex, caudate, globus pallidus, and thalamus bilaterally, which is the hallmark imaging finding:
1. Immediate Resuscitation (Restore Cardiorespiratory Function)
The first priority is eliminating the ongoing cause of hypoxia:
-
Airway: Secure the airway immediately; intubate if necessary
-
Oxygenation/ventilation: Ensure adequate oxygenation. Target SpO2 94-98% - avoid hyperoxia, as elevated cumulative oxygen tension is associated with worse functional outcomes
-
Restore cerebral perfusion: CPR, IV fluids, vasopressors (norepinephrine is commonly used), or cardiac pacing as needed
-
Target MAP >60 mmHg (systolic >90 mmHg). Higher perfusion targets may benefit patients with elevated ICP or intracranial stenosis, but benefit is not firmly established by trials
-
12-lead ECG immediately after ROSC; emergent cardiac catheterization if ST-elevation MI is identified
-
Head CT (noncontrast) to exclude hemorrhagic stroke or subarachnoid hemorrhage presenting as cardiac arrest
-
Harrison's Principles of Internal Medicine 22E (2025), p. 2390
-
Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 612
2. Targeted Temperature Management (TTM) - Neuroprotection
This is the primary neuroprotective strategy after return of spontaneous circulation (ROSC) in comatose survivors.
Current guideline recommendation: Maintain a constant temperature between 32-37.5°C in patients who have no meaningful response to verbal commands after ROSC. Fever must be actively avoided in all cases.
Evidence summary:
- Early trials showed mild hypothermia (33°C for 12-24 h) improved functional outcome after out-of-hospital cardiac arrest with shockable rhythms
- Subsequent larger trials (TTM trial) showed 33°C vs. 36°C yielded similar outcomes - suggesting the benefit may derive primarily from fever prevention rather than the degree of cooling
- A more recent trial found early fever treatment (target <37.8°C) resulted in similar outcomes to hypothermia to 33°C
- Current practice: target either 33°C or 36°C per institutional protocol, with strict fever avoidance
Methods to achieve temperature control:
- Surface cooling: cold baths, ice packs, adhesive pads, helmets
- IV infusion of chilled fluids
- Endovascular temperature control devices (balloons with circulating cold fluid)
- Modern devices use real-time temperature feedback loops
Shivering management (critical to maintaining target temperature):
- Counter-warming of hands/feet
- Acetaminophen 650 mg q4h PO
- Buspirone 30 mg q8h PO
- Sedation: propofol infusions (preferred) or benzodiazepines
- Analgesia: fentanyl or other opiate infusions
- Dexmedetomidine: potent anti-shivering agent
- Magnesium sulfate (target serum Mg 3-4 mEq/L)
- Meperidine 25 mg IV q6h (use cautiously - lowers seizure threshold)
- Neuromuscular blockade (vecuronium) as a last resort
Contraindications: Absolute - refractory bleeding at a non-compressible site, severe recurrent symptomatic bradycardia. Relative - severe baseline neurologic impairment, multiorgan failure, sepsis/meningitis, trauma, pregnancy.
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, pp. 613-615
3. Seizure Management
-
Seizures occur in 10-30% of comatose post-arrest patients, most with status epilepticus (SE)
-
Most common during rewarming; may be convulsive or nonconvulsive
-
Continuous EEG monitoring is essential - nonconvulsive seizures will be missed clinically
-
Treatment: levetiracetam, valproic acid, and benzodiazepines (e.g., clonazepam) are preferred in cardiac arrest patients
-
Myoclonic status epilepticus within 24 h post-arrest is a poor prognostic sign, even when controlled
-
Do not give prophylactic anticonvulsants routinely
-
Complete suppression of all rhythmic/periodic EEG activity for 48 h (in a clinical trial) did not improve outcomes vs. standard care - this strategy is not recommended
-
Post-hypoxic myoclonus: clonazepam 1.5-10 mg/day PO or valproate 300-1200 mg/day in divided doses
-
Harrison's Principles of Internal Medicine 22E (2025), p. 2391
-
Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 614
4. Intracranial Pressure (ICP) Management
-
Cerebral edema/swelling occurs in up to one-third of patients after cardiac arrest
-
Managed using standard ICP protocols (head of bed elevation, osmotic therapy, etc.)
-
Important caveat: brain swelling after cardiac arrest is a poor prognostic sign - it indicates extensive cortical neuronal loss, so decompressive craniectomy is generally not indicated
-
Monitor carefully during rewarming for possible herniation
-
Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 615
5. Systemic/Medical Management
| Parameter | Target / Action |
|---|---|
| Glucose | Normoglycemia: 140-180 mg/dL (insulin infusion) |
| Electrolytes | Monitor and replace K, Mg, phosphate (cold diuresis shifts these) |
| IV fluids | Avoid hypotonic fluids |
| Ventilation | Low tidal volume (6 mL/kg IBW) for ARDS (lung-protective) |
| Infection | Screen aggressively for pneumonia, UTI; prophylactic antibiotics NOT recommended |
| DVT prophylaxis | Pneumatic compression + subcutaneous heparin or enoxaparin |
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 615
6. Special Cases
Carbon monoxide / cyanide poisoning:
- Carbon monoxide intoxication: hyperbaric oxygen is the treatment of choice for severe cases
- Both CO and cyanide can cause delayed encephalopathy - a parkinsonian syndrome (akinesia + rigidity without tremor) can develop weeks later, with progressive basal ganglia damage on CT/MRI
Neonatal hypoxic-ischemic encephalopathy (HIE):
- Therapeutic hypothermia (whole-body or selective head cooling) is the established standard of care
- Multiple large RCTs support its use; xenon and argon as adjuncts are being investigated in preclinical and early clinical studies (PMID 39453983)
7. Prognostication
Prognostication guides goals-of-care decisions and should use a multimodal approach:
| Finding | Implication |
|---|---|
| Intact pupillary, corneal, oculocephalic reflexes | Better prognosis |
| Absent pupillary reflex + absent/extensor motor response at 5-7 days | Poor prognosis (excluding sedation/hypothermia confounders) |
| Bilateral absence of SSEP N20 (after several days) | Poor prognosis |
| Burst-suppression or nonreactive EEG | Poor prognosis |
| NSE >60 µg/L in first 1-3 days | Worse outcome |
| CT/MRI: diffuse cortical DWI restriction | Extensive injury |
Critical caveat: Hypothermia and sedation delay the reliable timing of clinical prognosticators. The false-positive rate for incorrect poor-prognosis prediction can be as high as 21% in hypothermia-treated patients at 3 days. Allow sufficient observation time (some patients awaken after a week or longer).
- Harrison's Principles of Internal Medicine 22E (2025), pp. 2389-2391
Summary Algorithm
HIBI suspected/confirmed
|
v
Restore airway + oxygenation (SpO2 94-98%) + circulation
|
v
ROSC achieved?
|
Yes
v
12-lead ECG → STEMI → emergent cath
Head CT → exclude hemorrhage/SAH
|
v
Comatose (no response to verbal commands)?
|
Yes → TTM: target 32-37.5°C (commonly 33°C or 36°C)
→ Treat/prevent fever STRICTLY
→ Continuous EEG monitoring
→ Seizure management (levetiracetam, VPA, clonazepam)
→ Normoglycemia, electrolyte management
→ Lung-protective ventilation
|
v
Multi-modal prognostication (earliest reliable: 5-7 days post-arrest,
longer if hypothermia used)
Sources: Harrison's Principles of Internal Medicine 22E (2025), pp. 2389-2391 | Plum and Posner's Diagnosis and Treatment of Stupor and Coma, pp. 612-616
This is a shared conversation. Sign in to Orris to start your own chat.