Out patient hypotension management
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypotension outpatient management treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
orthostatic hypotension management treatment
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
I now have comprehensive content to compose a detailed, well-structured answer. Let me compile everything.
Outpatient Hypotension Management
In the outpatient setting, hypotension most commonly refers to orthostatic (postural) hypotension - defined as a sustained fall in systolic BP ≥20 mmHg or diastolic BP ≥10 mmHg within 3 minutes of standing. Management follows a stepwise approach: correct aggravating factors → non-pharmacologic measures → pharmacologic therapy.
The goal of treatment is to improve symptoms, not to achieve a target blood pressure.
- Goldman-Cecil Medicine, p. 4062
Management Flowchart
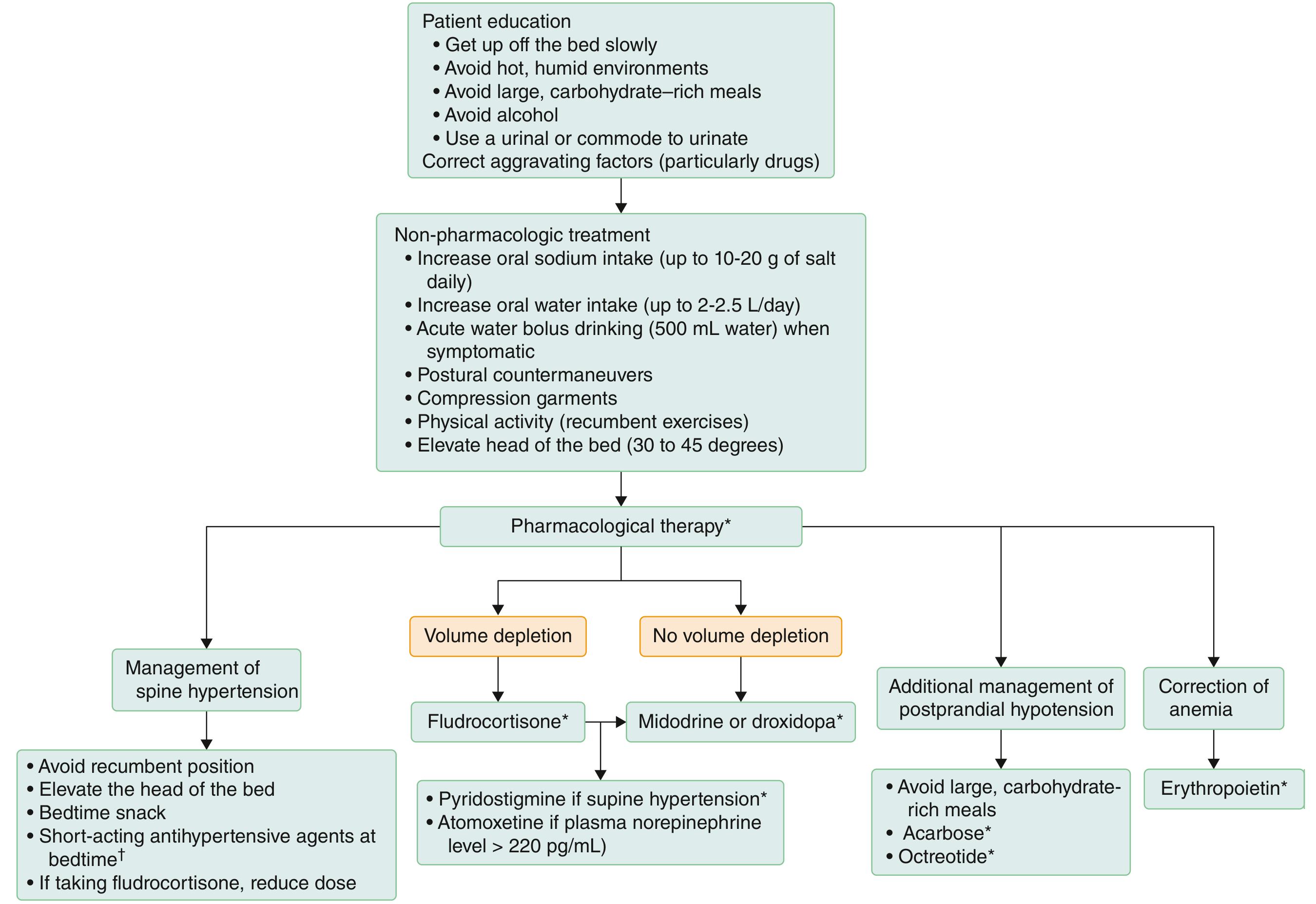
Step 1 - Correct Aggravating Factors
- Review and reduce medications that worsen hypotension: diuretics, alpha-blockers, antihypertensives, vasodilators, tricyclics, dopaminergic agents (levodopa/dopamine agonists in Parkinson's)
- Treat reversible causes: volume depletion, anemia, adrenal insufficiency
Step 2 - Patient Education (Always First)
- Rise from bed/chair slowly - briefly sit before standing
- Avoid hot, humid environments (cause vasodilatation)
- Avoid large carbohydrate-rich meals (postprandial splanchnic vasodilation)
- Avoid alcohol (potent vasodilator; if used, restrict to evenings before bedtime)
- Urinate in the sitting position (or use a urinal) to avoid Valsalva-triggered syncope
Step 3 - Non-Pharmacologic Measures
Fluid and Salt Loading
- Oral water intake: 2-2.5 L/day
- Salt intake: 10-20 g/day (add 1-2 teaspoons of salt to diet); salt tablets (0.5-1.0 g) are an alternative but may cause GI discomfort
- Acute rescue: Bolus water drinking (500 mL/16 oz) produces a rapid BP rise within 5-10 min, peaking at ~30 min - useful for acute symptomatic episodes
Physical Countermaneuvers
- Leg crossing, squatting, standing on tiptoes, buttock clenching, stooping - these all reduce venous pooling acutely
- Compression garments: High-waist stockings (at least 15-20 mmHg compression) or abdominal binder reduce venous pooling in the lower extremities and abdomen
- Elevate the head of the bed 30-45 degrees at night (reduces nocturnal hypertension and morning orthostasis)
Exercise
- Patients should NOT stop exercising (cardiovascular deconditioning worsens symptoms)
- Prefer recumbent or seated exercises, or swimming pool-based activity
Postprandial Hypotension
- Eat smaller, more frequent meals
- Low-carbohydrate diet
- Avoid large meals before activity
Step 4 - Pharmacologic Therapy
Volume Expansion
| Drug | Dose | Side Effects | Notes |
|---|---|---|---|
| Fludrocortisone | 0.1-0.2 mg orally daily | Supine hypertension, hypokalemia, ankle edema | First-line volume expander; takes ≥7 days to exert full effect; potential for LV hypertrophy and nephrotoxicity with prolonged use |
Vasoconstrictors (if no adequate response or if no volume depletion)
| Drug | Dose | Side Effects | Notes |
|---|---|---|---|
| Midodrine | 5-10 mg orally TID | Piloerection, scalp itching, urinary retention, supine hypertension | Selective α1-agonist prodrug; take before getting out of bed, before lunch, and NOT within 3-4 h of bedtime |
| Droxidopa | 100-600 mg orally TID | Supine hypertension | Synthetic amino acid converted to norepinephrine; same timing rules as midodrine; useful in neurogenic OH |
If Supine Hypertension Is a Problem (prefer these agents)
| Drug | Dose | Side Effects | Notes |
|---|---|---|---|
| Pyridostigmine | 30-60 mg orally TID | Bradycardia, abdominal cramps, diarrhea, sialorrhea, urinary incontinence | Acetylcholinesterase inhibitor; raises standing BP without worsening supine hypertension; can be combined with midodrine. 2025 systematic review confirms efficacy for neurogenic OH |
| Atomoxetine | 10-18 mg orally BID | Insomnia, irritability, decreased appetite | Norepinephrine reuptake inhibitor; more helpful in patients with preserved sympathetic terminals (plasma norepinephrine >220 pg/mL) |
Postprandial Hypotension (Adjuncts)
| Drug | Dose | Notes |
|---|---|---|
| Acarbose | 50-100 mg before meals | Alpha-glucosidase inhibitor; slows carbohydrate absorption |
| Octreotide | 0.2-0.4 mcg/kg SQ | Somatostatin analogue; reduces splanchnic vasodilation |
Anemia Correction
| Drug | Dose | Notes |
|---|---|---|
| Erythropoietin | 25-75 U/kg SQ 3x/week until Hct normalizes, then 25 U/kg 3x/week | For anemia of chronic disease worsening hypotension; iron supplementation often required concurrently |
Managing Supine Hypertension (common complication of treatment)
Many drugs used for orthostatic hypotension cause supine/nocturnal hypertension. Management includes:
- Avoid recumbent position during the day
- Elevate head of bed
- Bedtime snack (reduces nocturnal BP rise)
- Short-acting antihypertensive agents at bedtime (e.g., nitroglycerin patch removed on waking, losartan, or amlodipine)
- If on fludrocortisone, reduce dose
Special Clinical Scenarios
Neurogenic Orthostatic Hypotension (NOH)
Common in Parkinson's disease, multiple system atrophy, pure autonomic failure. Droxidopa has FDA approval for NOH. Midodrine and fludrocortisone are widely used. Pyridostigmine is preferred when supine hypertension is a concern.
Vasovagal / Reflex Syncope
Lifestyle measures (increased fluid and salt intake, counterpressure maneuvers) are first-line. Midodrine has evidence for recurrent vasovagal syncope prevention.
Postprandial Hypotension
Particularly problematic in elderly and diabetic patients. Small frequent low-carb meals, acarbose, and octreotide are helpful.
Drug-Induced Hypotension
The most common and reversible cause in outpatients. Always review the medication list carefully - offending agents include antihypertensives, diuretics, alpha-blockers, nitrates, PDE5 inhibitors, and psychotropics.
Recent Evidence
- A 2025 meta-analysis (PMID 40132893) confirms pyridostigmine is effective for managing orthostatic hypotension, with a favorable profile when supine hypertension is a concern.
- A 2025 systematic review on POTS treatments (PMID 40653179) highlights evidence for both pharmacologic and exercise-based interventions for postural tachycardia syndrome, a related autonomic disorder.
Sources: Goldman-Cecil Medicine (International Edition), pp. 4062-4063; Bradley and Daroff's Neurology in Clinical Practice; Harrison's Principles of Internal Medicine 22E; Fuster & Hurst's The Heart, 15th Edition
Outpatient management for hypotension
I already covered this topic in detail in my previous response above. Here's a structured summary for quick reference:
Outpatient Hypotension Management
Definition
Orthostatic hypotension (OH) = fall in systolic BP ≥20 mmHg or diastolic BP ≥10 mmHg within 3 minutes of standing.
Key principle: The goal is to relieve symptoms, not hit a BP target.
Step 1 - Correct Aggravating Factors
- Review and reduce/stop offending drugs: diuretics, alpha-blockers, nitrates, antihypertensives, PDE5 inhibitors, dopaminergic agents, tricyclics
- Treat reversible causes: volume depletion, anemia, adrenal insufficiency
Step 2 - Patient Education
- Rise slowly from lying or sitting
- Sit briefly before standing
- Avoid hot/humid environments
- Avoid large carbohydrate-rich meals
- Avoid alcohol (potent vasodilator)
- Urinate sitting down (avoids Valsalva-triggered syncope)
Step 3 - Non-Pharmacologic Measures
| Measure | Detail |
|---|---|
| Salt intake | 10-20 g/day (1-2 tsp added to diet; salt tablets 0.5-1.0 g are an option) |
| Water intake | 2-2.5 L/day |
| Acute rescue bolus | 500 mL water rapidly - raises BP within 5-10 min, peaks at ~30 min |
| Compression garments | High-waist stockings ≥15-20 mmHg, or abdominal binder |
| Physical countermaneuvers | Leg crossing, squatting, toe-standing, buttock clenching |
| Elevate head of bed | 30-45 degrees at night |
| Exercise | Recumbent or seated forms; swimming pool preferred |
| Meals | Small, frequent, low-carbohydrate meals for postprandial OH |
Step 4 - Pharmacologic Therapy
Volume Expansion
| Drug | Dose | Key Points |
|---|---|---|
| Fludrocortisone | 0.1-0.2 mg orally daily | First-line; synthetic mineralocorticoid; takes ≥7 days for full effect; monitor for supine hypertension, hypokalemia, edema, LV hypertrophy |
Vasoconstrictors
| Drug | Dose | Key Points |
|---|---|---|
| Midodrine | 5-10 mg orally TID | α1-agonist prodrug; take before rising, before lunch, NOT within 3-4 h of bedtime; causes supine hypertension |
| Droxidopa | 100-600 mg orally TID | Converted to norepinephrine; FDA-approved for neurogenic OH; same timing rules as midodrine |
Preferred When Supine Hypertension Is a Concern
| Drug | Dose | Key Points |
|---|---|---|
| Pyridostigmine | 30-60 mg orally TID | Raises standing BP without worsening supine hypertension; can combine with midodrine; SE: bradycardia, cramps, diarrhea |
| Atomoxetine | 10-18 mg orally BID | Best when plasma norepinephrine >220 pg/mL (preserved sympathetic terminals) |
Postprandial Hypotension Adjuncts
| Drug | Dose | Notes |
|---|---|---|
| Acarbose | 50-100 mg before meals | Slows carbohydrate absorption |
| Octreotide | 0.2-0.4 mcg/kg SQ | Reduces splanchnic vasodilation |
Anemia-Related Hypotension
| Drug | Dose | Notes |
|---|---|---|
| Erythropoietin | 25-75 U/kg SQ 3x/week | Correct anemia of chronic disease; co-administer iron |
Managing Supine Hypertension (a common treatment complication)
- Avoid lying flat during the day
- Elevate head of bed
- Bedtime snack
- Short-acting antihypertensive at bedtime (e.g., nitroglycerin patch removed on waking)
- Reduce fludrocortisone dose if it is the cause
Common Outpatient Subtypes
| Subtype | Priority |
|---|---|
| Drug-induced | Most common and most reversible - review the medication list first |
| Neurogenic OH (Parkinson's, MSA) | Droxidopa + midodrine; pyridostigmine if supine HTN |
| Vasovagal/reflex syncope | Hydration, salt, counterpressure maneuvers; midodrine for recurrent episodes |
| Postprandial OH | Small low-carb meals, acarbose, octreotide |
| Dehydration/volume depletion | Oral rehydration, salt loading, fludrocortisone |
Sources: Goldman-Cecil Medicine (International Edition), pp. 4062-4063; Bradley and Daroff's Neurology in Clinical Practice; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.