teach me blood picturefrom basics to clinical
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
I now have comprehensive, textbook-sourced content with real images. Let me compose the full teaching guide.
The Blood Picture - From Basics to Clinical
A complete teaching guide drawn from Henry's Clinical Diagnosis, Tietz Textbook of Laboratory Medicine, Histology (Eroschenko), Robbins Pathology, Harrison's, and Goldman-Cecil Medicine.
PART 1 - What is the "Blood Picture"?
The term blood picture refers to the full interpretation of a peripheral blood smear (PBS) combined with the complete blood count (CBC). It is the most ordered investigation in medicine and serves as a window into the bone marrow, immune system, nutritional status, and dozens of systemic diseases.
PART 2 - The CBC: Numbers First
The CBC is generated by automated flow cytometry-based analyzers that count ~10,000 cells per category. The key parameters:
| Parameter | Normal Range | What it Reflects |
|---|---|---|
| RBC count | M: 4.5-5.5 × 10¹²/L; F: 4.0-5.0 × 10¹²/L | Total circulating red cells |
| Hemoglobin (Hb) | M: 13.5-17.5 g/dL; F: 12-15.5 g/dL | O₂-carrying capacity |
| Hematocrit (HCT/PCV) | M: 41-53%; F: 36-46% | Packed cell volume |
| MCV | 80-100 fL | Average RBC size |
| MCH | 27-33 pg | Hb per cell |
| MCHC | 31-36 g/dL | Hb concentration per cell |
| RDW | <14.5% | Variation in RBC size (anisocytosis) |
| WBC | 4.5-11.0 × 10⁹/L | Total leukocytes |
| Platelets | 150-400 × 10⁹/L | Thrombocytes |
The rule of thirds: Hb × 3 ≈ HCT, and HCT × 3 ≈ RBC count (roughly). A quick bedside check for CBC consistency.
Source: Histology - A Text and Atlas (Eroschenko), p. 728-729
PART 3 - Making and Reading the Blood Film
Preparation
Blood is anticoagulated in EDTA and a wedge film (or coverslip preparation) is made. It is stained with Romanowsky stain (Wright-Giemsa). The film must be:
- Well-made (no artefacts, uniform thickness)
- Properly stained
- Evaluated systematically: low power scan first (10x), then high power (40-100x oil immersion)
The Systematic Approach
When you pick up a blood film, go through these 5 steps in order:
- Scan at low power - estimate WBC count, check for clumps, parasites, large abnormal cells
- Evaluate RBC morphology - size, shape, colour, inclusions
- Perform differential WBC count - 100 cells minimum; note morphology
- Estimate platelet count - ~1 platelet per 10-30 RBCs = normal
- Note any abnormal cells - nucleated RBCs, blasts, parasites - these are NEVER normal in peripheral blood
PART 4 - Normal RBC Morphology
The reference image - normal RBCs:
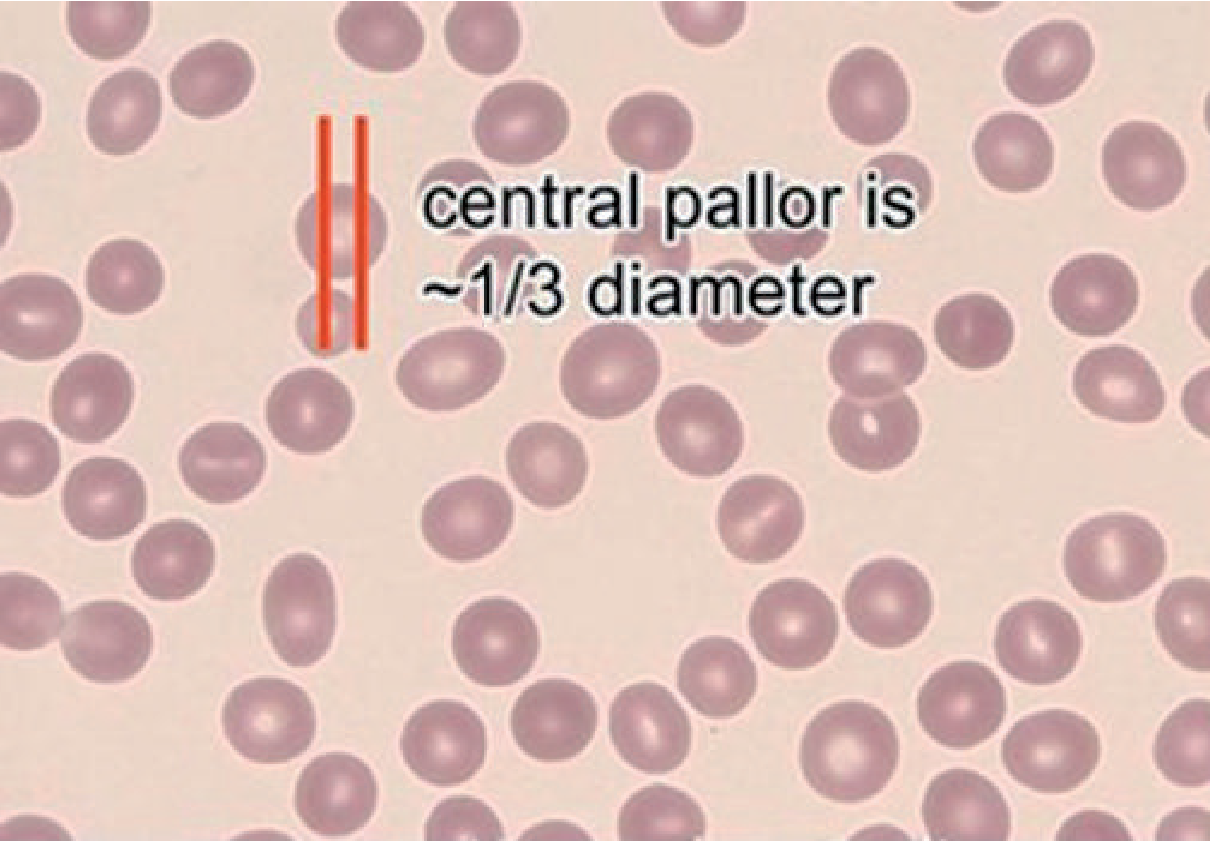
Normal RBCs are:
- Normocytic: MCV 80-100 fL, diameter ~6-8 µm (roughly the size of a small lymphocyte nucleus)
- Normochromic: MCHC 31-36 g/dL; central pallor = approximately 1/3 of the cell diameter
- Uniform in shape: biconcave discs - this gives them flexibility to squeeze through capillaries
- Uniform in size: minimal anisocytosis (RDW <14.5%)
Source: Tietz Textbook of Laboratory Medicine, 7th Ed., p. 2989
PART 5 - Abnormal RBC Morphology (The Core of the Blood Picture)
This is the most clinically useful part. Each abnormal shape has a differential diagnosis.
5.1 - Size Changes
| Abnormality | Feature | Key Causes |
|---|---|---|
| Microcytes | RBC <6 µm, MCV <80 fL, increased central pallor | Iron deficiency anemia, thalassemia, anemia of chronic disease, sideroblastic anemia |
| Macrocytes | RBC >8 µm, MCV >100 fL | B12/folate deficiency, liver disease, hypothyroidism, MDS, chemotherapy (methotrexate) |
| Anisocytosis | Variation in size | Elevated RDW; seen in iron deficiency (one of the earliest findings), mixed deficiencies |
Pearl: In iron deficiency, anisocytosis (high RDW) appears BEFORE the MCV falls. An elevated RDW with normal MCV should prompt iron studies.
5.2 - Shape Changes (Poikilocytosis)
| Cell | Description | Mechanism | Causes |
|---|---|---|---|
| Spherocyte | Small, round, no central pallor | Loss of membrane | Hereditary spherocytosis, AIHA, ABO incompatibility |
| Elliptocyte / Ovalocyte | Oval/cigar-shaped | Spectrin mutation | Hereditary elliptocytosis; also iron deficiency (pencil cells = hypochromic elliptocytes) |
| Target cell (Codocyte) | Bullseye appearance | Excess membrane or decreased Hb | Thalassemia, HbC disease, liver disease, post-splenectomy, iron deficiency |
| Sickle cell (Drepanocyte) | Elongated crescent/scythe | HbS polymerisation under low O₂ | Sickle cell disease (pathognomonic) |
| Schistocyte | RBC fragments, helmet cells | Mechanical shearing in small vessels | TTP, HUS, DIC, prosthetic heart valves, HELLP syndrome |
| Acanthocyte (Spur cell) | Irregular spicules of varying length | Membrane lipid abnormality | Abetalipoproteinemia, severe liver disease, McLeod phenotype |
| Echinocyte (Burr cell) | Regular spicules, uniform | Crenation (often artefact) | Uremia, liver disease, often artefact (EDTA effect) |
| Stomatocyte | Slit-like central pallor (mouth shape) | Altered Na/K permeability | Hereditary stomatocytosis, alcohol, liver disease |
| Teardrop cell (Dacrocyte) | Teardrop-pear shape | Forced through stiff marrow stroma | Myelofibrosis, thalassemia, infiltrative marrow disease |
| Bite cell (Degmacyte) | Semicircular bite out of cell | Heinz body removed by spleen | G6PD deficiency, unstable hemoglobins, oxidative drug exposure |
Source: Tietz Textbook of Laboratory Medicine, Table 76.1, pp. 2989-2990; Harrison's Principles of Internal Medicine 22E
PART 6 - RBC Inclusions
| Inclusion | Stain | Composition | Causes |
|---|---|---|---|
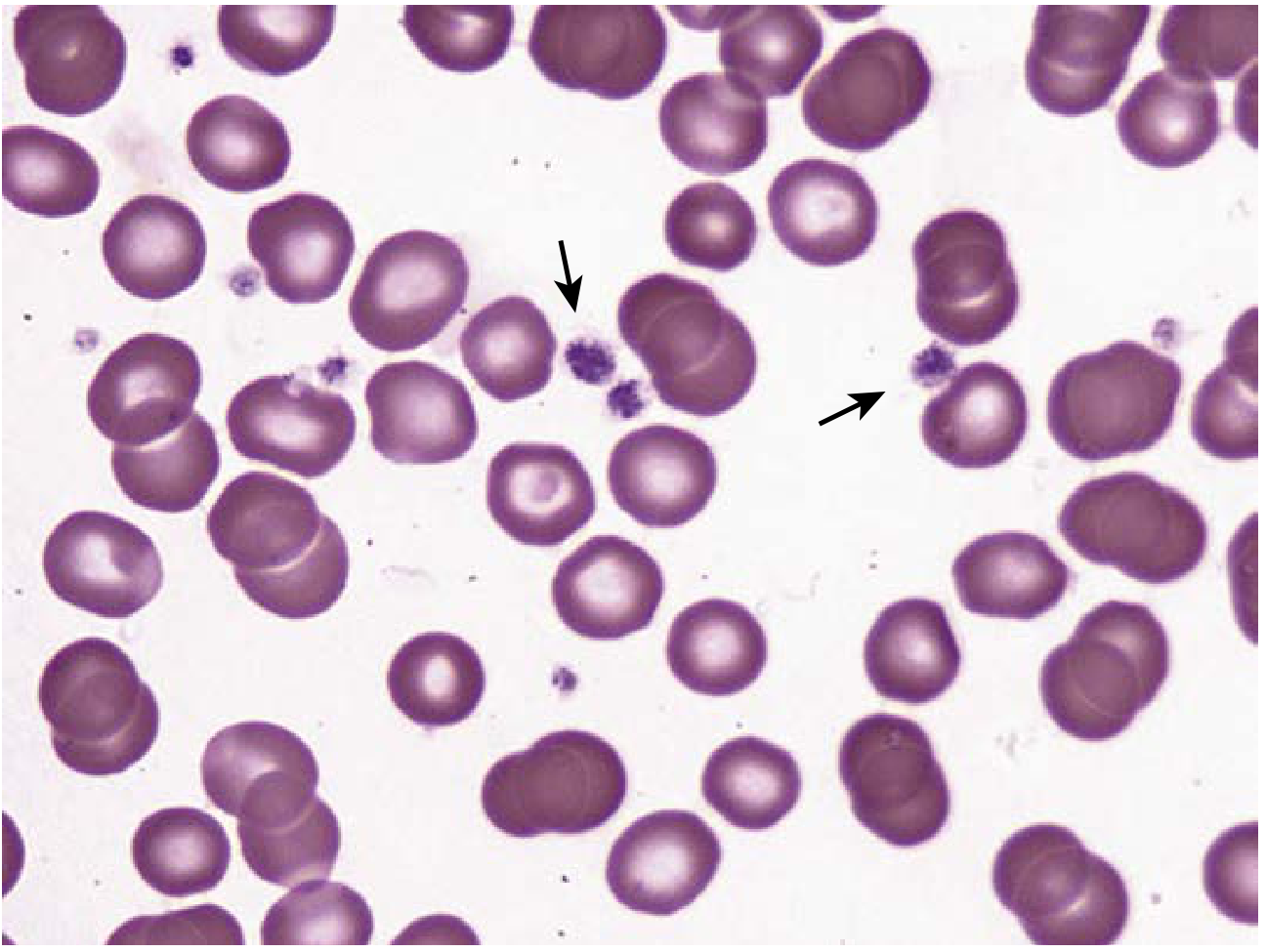
| Howell-Jolly bodies | Romanowsky (dark purple dot) | DNA remnant (chromosome fragment) | Post-splenectomy, functional asplenia (sickle cell), megaloblastic anemia |
| Basophilic stippling | Romanowsky (blue dots) | Aggregated ribosomes | Lead poisoning, thalassemia, megaloblastic anemia, pyrimidine 5'-nucleotidase deficiency |
| Heinz bodies | Supravital stain (brilliant cresyl blue) - NOT visible on Romanowsky | Denatured/oxidised Hb | G6PD deficiency, unstable hemoglobins, alpha-thalassemia |
| Pappenheimer bodies | Romanowsky and Prussian blue | Iron granules (siderosomes) | Sideroblastic anemia, post-splenectomy, hemolytic anemia |
| Cabot rings | Romanowsky (ring/figure-8) | Mitotic spindle remnant | Severe megaloblastic anemia, lead poisoning |
| Malaria parasites | Romanowsky | Plasmodium sp. | Malaria (ring forms in P. falciparum; enlarged cells in P. vivax/ovale) |
PART 7 - WBC Morphology on the Blood Film
The Differential - Normal Ranges
| Cell | % | Absolute count × 10⁹/L | Key morphology |
|---|---|---|---|
| Neutrophil | 50-70% | 1.8-7.0 | 2-5 lobes, coarse chromatin, pale granules |
| Lymphocyte | 20-40% | 1.0-4.8 | Round nucleus, scant cytoplasm |
| Monocyte | 2-8% | 0.2-0.8 | Kidney-shaped nucleus, grey cytoplasm |
| Eosinophil | 1-4% | 0.04-0.4 | 2-lobed, large orange-red granules |
| Basophil | 0-1% | 0-0.1 | Large dark blue/purple granules obscure nucleus |
Neutrophil Morphology in Detail
Segmented vs. Band Neutrophil:
- Segmented (mature): 2+ lobes connected by thin filaments (thread-like, no width)
- Band (immature): horseshoe/U-shaped nucleus, thicker connection between lobes - filament has width
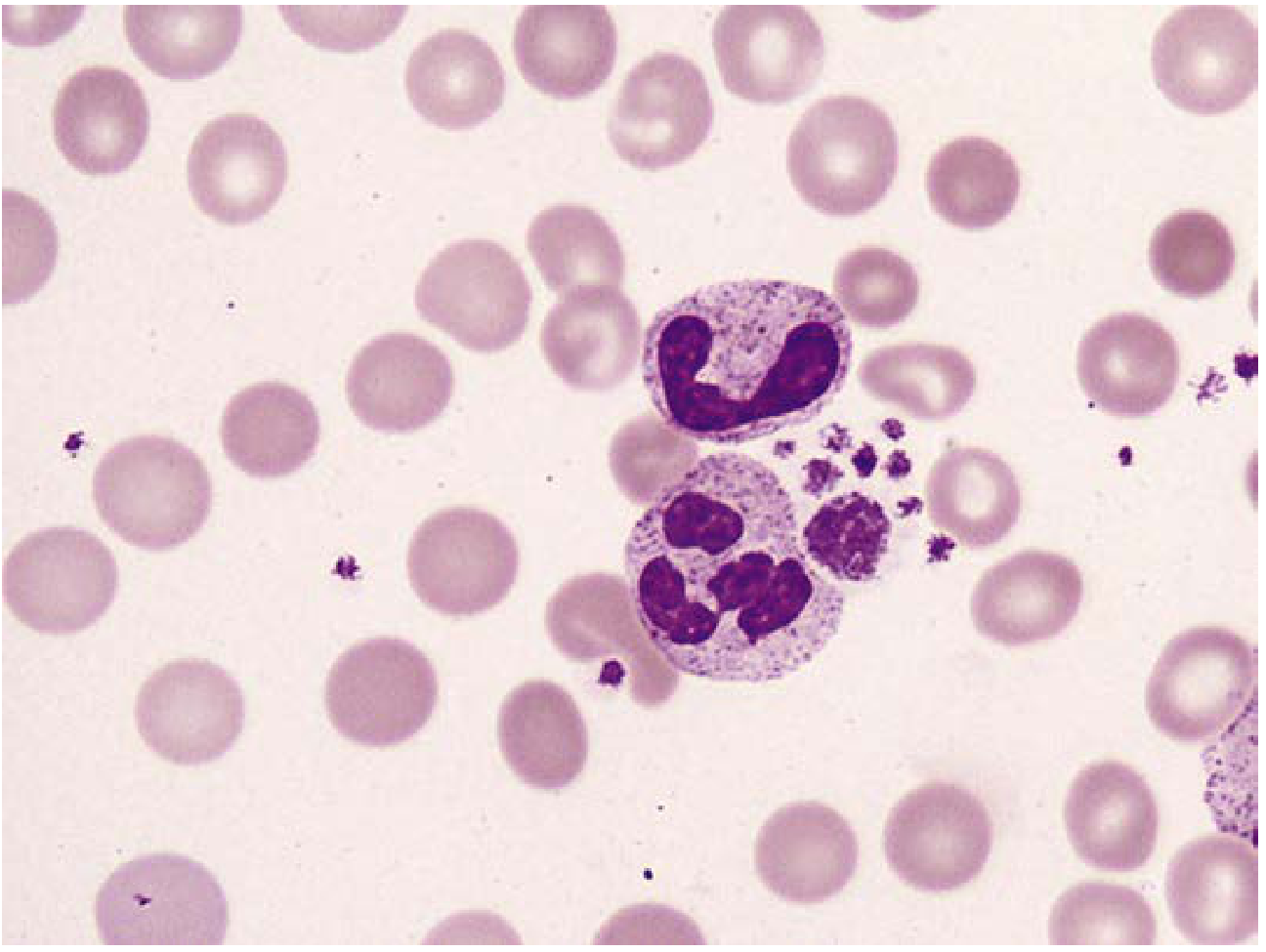
(Here you can see two neutrophils with lobulated nuclei and pale granular cytoplasm, surrounded by normocytic normochromic RBCs and a platelet cluster.)
Clinically Important WBC Changes
Left shift: appearance of immature granulocytes in blood (bands, metamyelocytes, myelocytes) - seen in sepsis, severe infection, myeloproliferative disorders
Toxic granulation: coarse, dark-blue primary granules in neutrophils - indicates severe bacterial infection, sepsis, or toxic states
Dohle bodies: pale blue cytoplasmic inclusions in neutrophils (rough ER remnants) - sepsis, burns, pregnancy
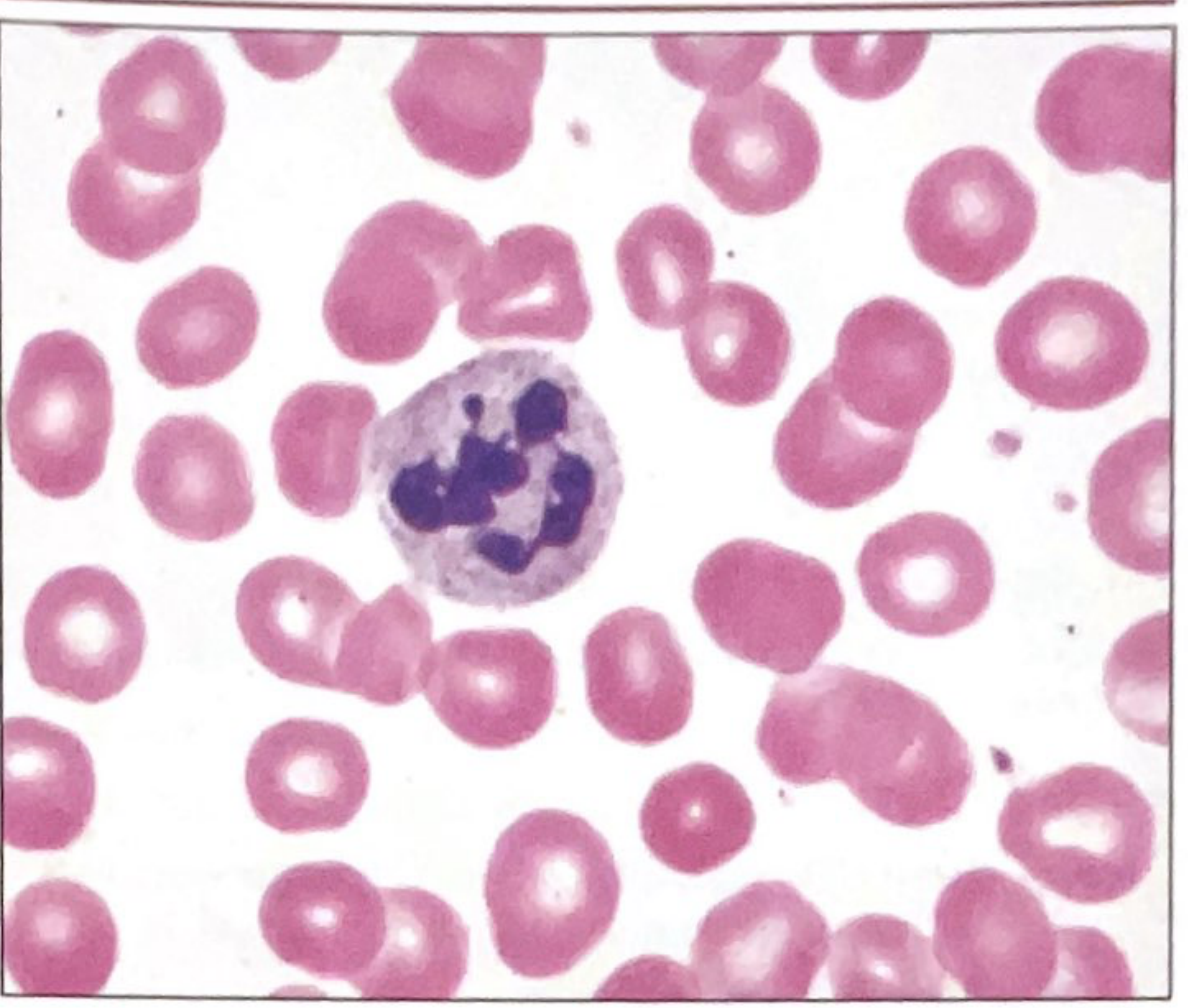
Hypersegmentation (>5 lobes): classic for megaloblastic anemia (B12/folate deficiency). Defined as: >5% of neutrophils with 5+ lobes, OR any neutrophil with 6+ lobes.
Reactive lymphocytosis: atypical lymphocytes (Downey cells) - large, irregular, with abundant blue cytoplasm that indents around adjacent RBCs - seen in EBV (infectious mononucleosis), CMV, viral hepatitis
PART 8 - Platelet Assessment on the Film
Estimation rule: ~7-20 platelets per oil immersion field = normal count (corresponds to 150-400 × 10⁹/L)
Normal platelets: 2-4 µm, round to oval, contain fine purple granules. Central "granulomere" and peripheral pale "hyalomere" may be seen.
Giant platelets (>3 µm): ITP (immune thrombocytopenic purpura), Bernard-Soulier syndrome, myeloproliferative neoplasms
Platelet clumping: artefact from EDTA causing pseudothrombocytopenia - check by repeating in citrate tube
Hypogranular platelets: myeloproliferative neoplasms (especially CML, ET)
Source: Henry's Clinical Diagnosis, p. 645
PART 9 - Clinical Integration: Reading the Film Diagnostically
This is where it all comes together. Use the MCV as your first branch point.
The MCV-Based Approach to Anemia
ANEMIA (low Hb)
|
+--- MCV <80 fL (MICROCYTIC)
| Iron deficiency: ↑RDW, hypochromia, pencil cells, ↓ferritin, ↑TIBC
| Thalassemia: normal or ↓RDW, target cells, basophilic stippling, normal ferritin
| Anemia of chronic disease: usually normocytic, but can be microcytic; ↑ferritin
| Sideroblastic: ring sideroblasts on bone marrow; dimorphic picture on PBS
|
+--- MCV 80-100 fL (NORMOCYTIC)
| Acute blood loss, hemolytic anemia, anemia of chronic disease
| Aplastic anemia, renal disease (EPO deficiency)
| Mixed deficiency (Fe + B12 -- can cancel each other out to give normal MCV!)
|
+--- MCV >100 fL (MACROCYTIC)
Megaloblastic: oval macrocytes + hypersegmented neutrophils
(B12 deficiency: subacute combined degeneration; folate: neural tube defects)
Non-megaloblastic: round macrocytes (liver disease, alcohol, hypothyroidism, MDS)
Source: Robbins Pathologic Basis of Disease, Table 14.1; Harrison's, p. 731
Disease-Specific Patterns
| Disease | Blood Film Clues |
|---|---|
| Iron deficiency anemia | Hypochromic microcytes, pencil cells (hypochromic elliptocytes), ↑RDW, thrombocytosis (reactive) |
| B12/Folate deficiency | Oval macrocytes, hypersegmented neutrophils (≥5 lobes), pancytopenia in severe cases |
| Sickle cell disease | Sickle cells (pathognomonic), target cells, Howell-Jolly bodies (functional asplenia), polychromasia |
| Thalassemia | Microcytes, target cells, basophilic stippling, nucleated RBCs, tear drop cells (beta-thal major) |
| TTP/HUS/DIC | Schistocytes (microangiopathic hemolysis) + thrombocytopenia - this is a medical emergency |
| Hereditary spherocytosis | Spherocytes (no central pallor), polychromasia (reticulocytosis), increased MCHC |
| G6PD deficiency (after oxidant stress) | Bite cells, Heinz bodies (on supravital stain), polychromasia |
| Malaria | Ring forms inside RBCs, multiple infections per cell (P. falciparum), enlarged pale RBCs (P. vivax) |
| CML | Leukocytosis with full granulocyte spectrum (myelocytes, metamyelocytes, bands), eosinophilia, basophilia |
| Infectious mononucleosis | Atypical lymphocytes (>10% Downey cells), lymphocytosis |
| ITP | Isolated thrombocytopenia, giant platelets, otherwise normal smear |
| Aplastic anemia | Pancytopenia, no blasts, no abnormal cells - "empty" smear |
| AML | Blasts (large cells with open chromatin, prominent nucleoli, Auer rods in M2/M3), +/- Auer rod clumps |
| CLL | Lymphocytosis of small mature lymphocytes + smudge/smear cells (fragile CLL cells rupturing during slide prep) |
PART 10 - Key Terminology Summary
| Term | Meaning |
|---|---|
| Anisocytosis | Variation in RBC size |
| Poikilocytosis | Variation in RBC shape |
| Polychromasia | RBCs with bluish tint = reticulocytes (young RBCs with residual RNA) |
| Hypochromia | Increased central pallor (>1/3 diameter) = reduced MCHC |
| Rouleaux | RBCs stacked like coins - seen in high fibrinogen, paraproteinaemia (myeloma) |
| Leukoerythroblastic reaction | Immature WBCs + nucleated RBCs in peripheral blood = bone marrow infiltration (cancer mets, myelofibrosis) |
| Left shift | Immature neutrophil precursors in blood = active marrow response (usually infection) |
| Dimorphic picture | Two populations of RBCs (normochromic + hypochromic) - sideroblastic anemia, post-transfusion, treated iron deficiency |
PART 11 - A Practical Approach Summary
When you receive a blood picture report or look at a film yourself:
- Check the numbers (CBC): Is there anemia? Leukocytosis/leukopenia? Thrombocytopenia? Is it one cell line or pancytopenia?
- Classify anemia by MCV: Micro/Normo/Macrocytic
- Check RDW: High RDW = iron deficiency or mixed; normal/low RDW = thalassemia or chronic disease
- Look at the film description: What shapes? Inclusions? Color changes?
- Look at the white cells: Hypersegmented? Left shift? Blasts? Atypical lymphocytes?
- Look at platelets: Count estimate, size, morphology
- Correlate with the clinical context: The film never stands alone - always integrate with history, examination, and other tests
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods; Tietz Textbook of Laboratory Medicine 7th Ed.; Histology - A Text and Atlas (Eroschenko); Robbins Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Quick Compendium of Clinical Pathology 5th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.