Riglers triad
Reading File
Finding Sources
Searching the Web
Rigler's triad gallstone ileus radiology findings
Reading File
Reading File
Loading Image
Rigler's Triad
Rigler's triad is the classic set of three radiographic signs diagnostic of gallstone ileus - a rare form of mechanical small bowel obstruction caused by a large gallstone migrating through a cholecystoenteric (bilioenteric) fistula into the gut.
The Three Components
| # | Sign | What it means |
|---|---|---|
| 1 | Pneumobilia | Air in the biliary tree, from the cholecystoenteric fistula through which the stone passed |
| 2 | Small bowel obstruction | Dilated bowel loops with air-fluid levels; transition point where the stone is lodged |
| 3 | Ectopic (aberrant) gallstone | A calcified stone visible outside the gallbladder, classically in the right iliac fossa / right lower quadrant |
First described by Leo Rigler in 1941; the eponym was formally attached in 1989.
CT Scan Showing All Three Elements
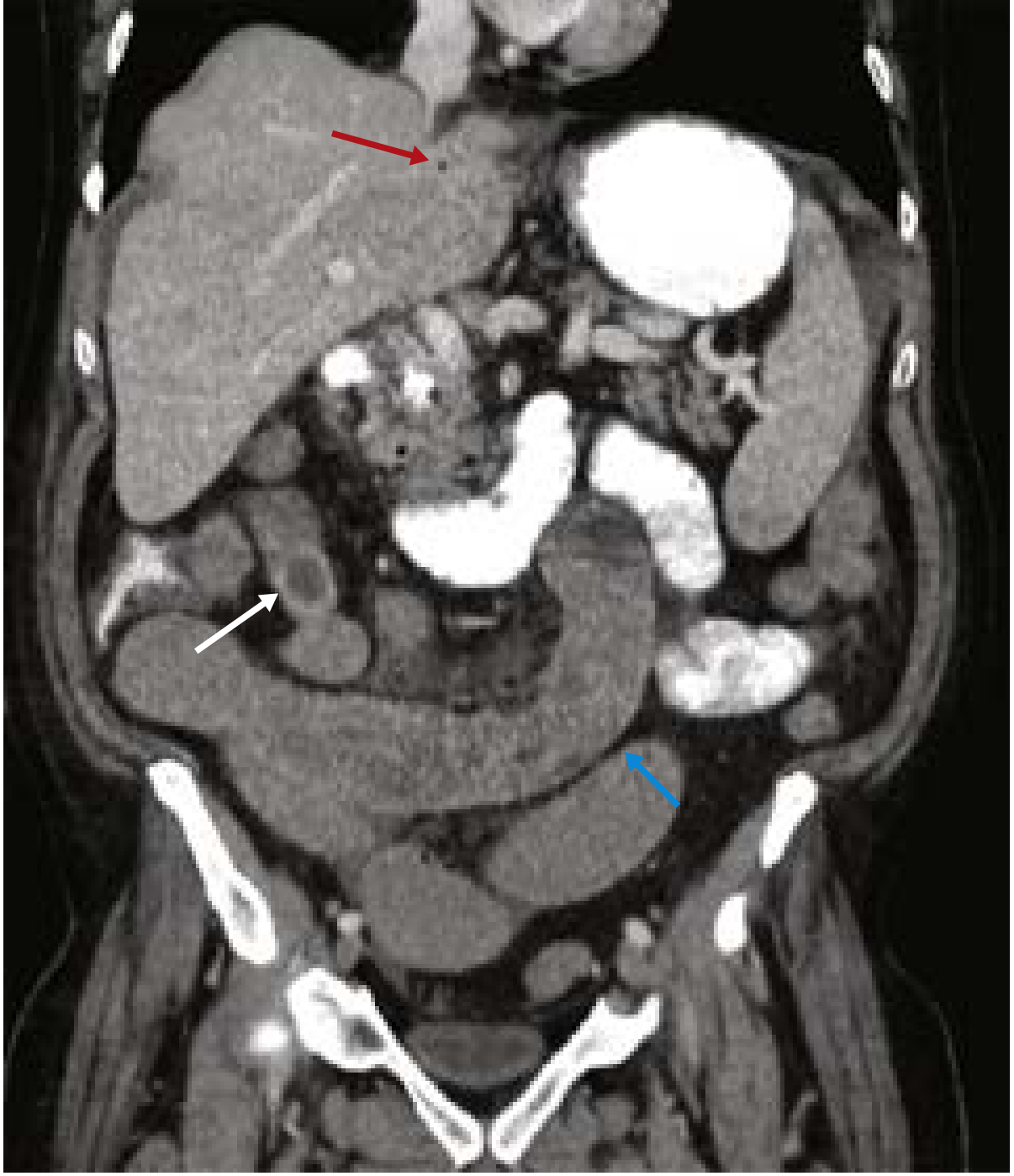
CT coronal image showing all three components: pneumobilia from bilioenteric fistula (red arrow), dilated small bowel (blue arrow), and obstructing ectopic gallstone (white arrow). - Current Surgical Therapy 14e
Diagnostic Value & Sensitivity
- All three signs together are pathognomonic, but this complete triad is seen in only ~15% of cases on plain X-ray and up to ~80% on CT
- Two of three signs is considered sufficient for diagnosis in clinical practice, present in ~40-50% of cases (Bailey & Love)
- Pneumobilia alone may be absent if the cholecystoenteric fistula has spontaneously closed, which occurs in ~80% of gallstone ileus cases
- Most gallstones (~90%) are radiolucent, making the ectopic stone component the hardest to spot on plain film
Why Findings Are Often Missed
- Stones are mostly radiolucent on X-ray
- Clinical presentation is non-specific (elderly female with intermittent bowel obstruction symptoms - "tumbling obstruction")
- Pneumobilia can also be seen after ERCP with sphincterotomy, reducing its specificity in isolation
Imaging of Choice
CT abdomen is the modality of choice - it detects all three components far more reliably than plain films, shows the transition point, reveals intraluminal stones, and characterizes fistula anatomy. MRCP can further define fistula anatomy but is reserved for stable patients.
Clinical Context
- Gallstone ileus accounts for ~1-4% of all small bowel obstructions, but ~25% in patients >65 years
- Classic impaction site: ~60 cm proximal to the ileocaecal valve (narrowest part of the small bowel)
- Treatment: enterolithotomy (milking the stone proximally and extracting it); cholecystectomy and fistula repair can be deferred to a second stage
Sources: Current Surgical Therapy 14e, p. 564 | Bailey & Love's Surgery 28th ed. | Sabiston Textbook of Surgery | Fischer's Mastery of Surgery 8th ed. | LITFL Eponym Library
Give just answer for the following
It looks like your message got cut off - you didn't include the question. Please go ahead and share it!
Caudate lobe which segment
Segment I (Couinaud classification).
This is a shared conversation. Sign in to Orris to start your own chat.