Unmasked hypertension
Reading File
Searching PubMed
masked hypertension cardiovascular risk
Finding Sources
Finding Sources
Reading Article
PMID: 39722158
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have everything needed for a thorough answer. Here is the full breakdown:
Masked (Unmasked) Hypertension
Terminology note: The condition is most precisely called masked hypertension in published literature. "Unmasked hypertension" is a colloquial phrase sometimes used to describe the same phenomenon - blood pressure that is "unmasked" (revealed) only outside the clinic. The two terms refer to the same entity.
Definition
Masked hypertension is defined as:
- Normal office/clinic blood pressure: < 130/80 mmHg
- Elevated out-of-office BP: home BP ≥ 130/80 mmHg OR ambulatory BP ≥ 125/75 mmHg
...in a patient not on antihypertensive therapy. If the patient is on antihypertensive drugs, the same pattern is called masked uncontrolled hypertension (MUCH).
This is the mirror image of white coat hypertension, where office BP is high but out-of-office BP is normal. - Goldman-Cecil Medicine, p. 3781; Fuster's The Heart 15e, p. 2606
Mechanism
The most accepted explanation is that frequently encountered daily stressors evoke sympathetic nervous system hyperactivity, but those stressors are reduced or absent when the patient is in the calm clinical setting. The result: BP normalizes in the office but rises during the person's real-world environment (work, physical activity, sleep).
A potential confounder is nonstandard home measurement technique or inaccurate devices, which can inflate home readings and create false positive diagnoses. - Goldman-Cecil Medicine, p. 3781
Prevalence
- 10-19% of individuals in population studies have masked hypertension
- Among persons with office BP > 140/90 mmHg, prevalence is 15-30%
- The IDACO study estimated prevalence at 13-19%
- A 2024 meta-analysis (26 studies, 129,061 participants) found a pooled prevalence of 18% (95% CI 15-21%) - [Zhu et al., 2024, PMID 39722158]
Associated Conditions (Higher Risk Groups)
- Older adults
- Diabetes mellitus
- Chronic kidney disease (CKD)
- Obstructive sleep apnea (OSA)
- Patients on antihypertensive therapy (masked uncontrolled hypertension)
Goldman-Cecil Medicine, p. 3782
Cardiovascular Risk - The Key Point
Masked hypertension carries significantly greater cardiovascular risk than white coat hypertension, which is essentially near normotensive. Data from the IDACO study and multiple meta-analyses show:
- Masked hypertension is associated with similar cardiovascular risk as sustained hypertension
- White coat hypertension: HR 0.964, P = .85 (no difference from normotension)
- Masked hypertension: HR 2.09 (P < .0001) vs. normotension
Brenner & Rector's The Kidney, p. 2410-2415
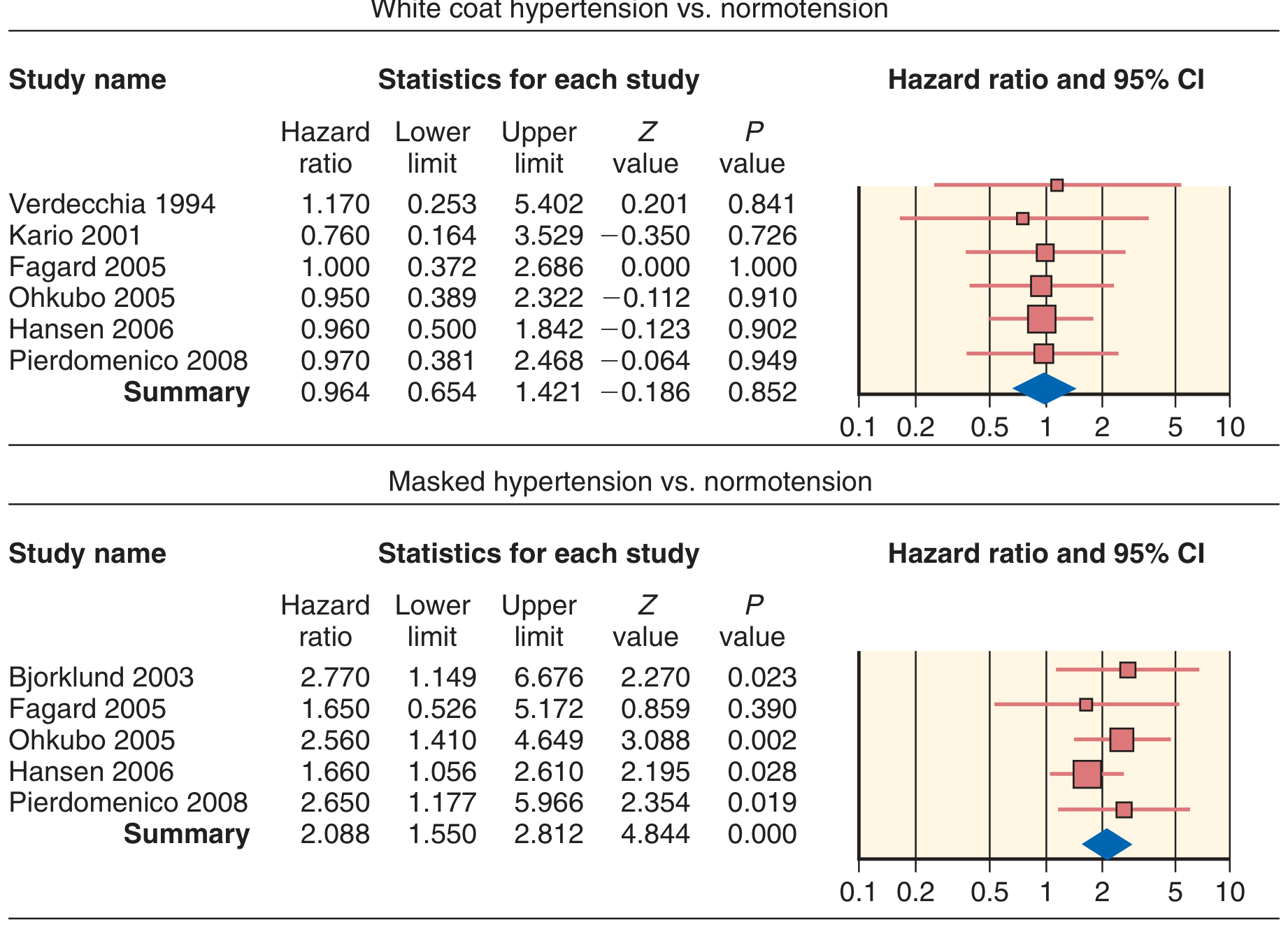
Fig: Meta-analysis of fatal/nonfatal cardiovascular events. Masked hypertension confers a >2-fold increase in risk. (From Pierdomenico & Cuccurullo, Am J Hypertens, 2011)
The 2024 meta-analysis by Zhu et al. (PMID 39722158) confirmed in 129,061 participants:
- All-cause mortality: RR 1.64 (95% CI 1.32-2.04)
- Incident CVD: RR 1.57 (95% CI 1.45-1.69)
- Cardiovascular mortality: RR 1.69 (95% CI 1.02-2.78)
- Composite renal outcomes: RR 3.57 (95% CI 2.32-5.50)
How It is Identified
Because office BP is normal, masked hypertension is only detectable with out-of-office measurement:
| Method | Threshold for diagnosis |
|---|---|
| Home BP monitoring (HBPM) | ≥ 130/80 mmHg |
| Ambulatory BP monitoring (ABPM) - 24h | ≥ 125/75 mmHg |
| ABPM - daytime only | ≥ 130/80 mmHg |
| ABPM - nighttime | ≥ 110/65 mmHg |
Who to screen: The 2017 ACC/AHA guidelines recommend considering out-of-office BP screening (Class IIa) for adults with office BP consistently 120-129/80-84 mmHg and/or those with target organ damage (e.g., left ventricular hypertrophy) or other cardiovascular risk factors. - Fuster's The Heart 15e, p. 2614
The ACC guidelines also extended Medicare/insurance coverage for ABPM to include masked hypertension indications. - NKF Primer on Kidney Diseases 8e, p. 2519
Treatment
This remains an area of uncertainty:
- No randomized controlled trial data have yet demonstrated benefit from drug therapy specifically in patients with masked hypertension
- The 2017 ACC/AHA guidelines recommend (Class IIa): continuation of lifestyle modification and initiation of antihypertensive drug therapy based on the overall CV risk profile
- Given the cardiovascular risk is comparable to sustained hypertension, most experts treat similar to sustained hypertension pending trial data
- Close monitoring with HBPM or ABPM is warranted to assess progression and treatment response
Goldman-Cecil Medicine, p. 3782; Fuster's The Heart 15e, p. 2614
White Coat vs. Masked: Quick Comparison
| Feature | White Coat HTN | Masked HTN |
|---|---|---|
| Office BP | High (≥ 130/80) | Normal (< 130/80) |
| Out-of-office BP | Normal | Elevated |
| Mechanism | Adrenergic response to clinical setting | Sympathetic activation by daily stressors |
| Prevalence | 15-30% of office HTN | 13-19% of population |
| CV risk | Minimal/none | Similar to sustained HTN |
| Treatment | Lifestyle + monitoring | Lifestyle + drugs (Class IIa) |
| Progression | ~1-5%/year to sustained HTN | Higher risk of sustained HTN |
Summary
Masked hypertension is a clinically silent but dangerous condition affecting roughly 1 in 6 adults. Its normal office readings mean it goes undetected without out-of-office measurement. The cardiovascular and renal consequences are similar to sustained hypertension. Prompt identification via HBPM or ABPM - especially in high-risk patients (diabetics, CKD, OSA, elderly, those with borderline office readings) - is the key clinical action. Treatment with antihypertensive therapy is reasonable given the risk profile, even though definitive RCT evidence is still pending.
Sources: Goldman-Cecil Medicine (2 Vol. Set), p. 3776-3782 | Fuster & Hurst's The Heart 15e, p. 2604-2614 | Brenner & Rector's The Kidney (2 Vol. Set), p. 2405-2415 | Zhu et al. [PMID 39722158], J Evid Based Med, 2024
Search recent guidelines on screening and treating masked hypertension
Searching PubMed
masked hypertension screening guidelines
Searching PubMed
masked hypertension treatment antihypertensive outcome
Searching the Web
masked hypertension 2024 2025 guidelines screening treatment ESC AHA
Reading Web Page
https://www.ahajournals.org/doi/10.1161/CIR.0000000000001356
Reading Article
PMID: 40244524
Reading Article
PMID: 39725775
Searching PubMed
masked hypertension ambulatory blood pressure monitoring home blood pressure
Chest pain and it’s differential diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Create a differential diagnosis poster for chest pain
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Generate a chest pain differential diagnosis PDF reference card
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.