Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough explanation of everything in your notes on Cushing's Syndrome, enhanced with content from Robbins & Kumar Basic Pathology and Campbell-Walsh Urology.
Cushing's Syndrome - Complete Notes Explained
Definition
Cushing's syndrome = glucocorticoid (cortisol) excess, regardless of cause. The hallmark is chronically elevated serum cortisol.
Etiopathogenesis (Causes)
Here is the full classification, matching your notes exactly:
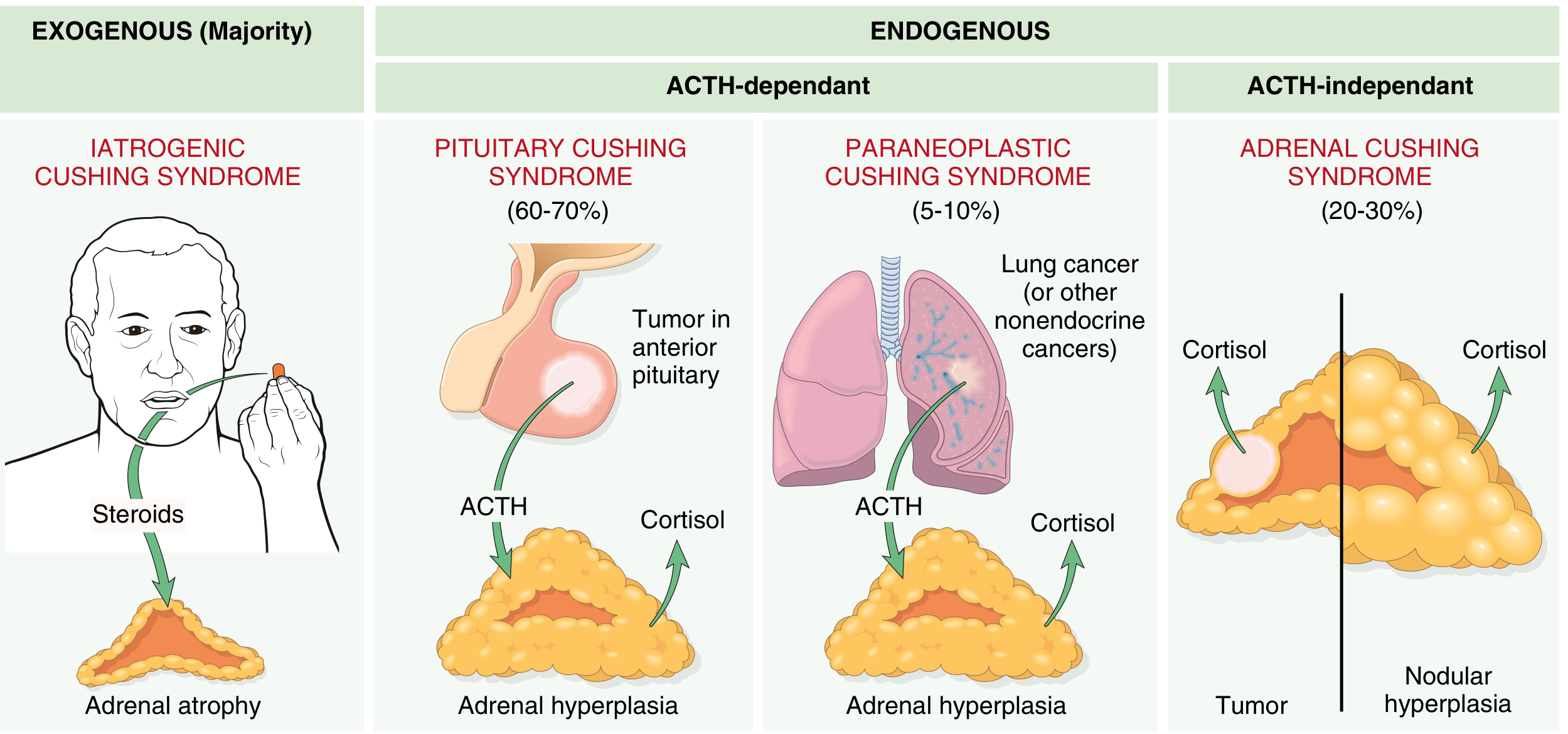
a) Exogenous Corticosteroids (Drugs) - MOST COMMON overall
- Patient is given steroids for treatment of another disease (e.g., asthma, autoimmune disease)
- The exogenous cortisol feeds back negatively on the pituitary, suppressing ACTH production
- Result: decreased ACTH + bilateral adrenal atrophy (both adrenal glands shrink because they receive no ACTH stimulation)
b) Adrenal Cushing's Syndrome (ACTH-independent, ~20-30% of endogenous cases)
- Caused by a primary adrenal adenoma (most common adrenal cause), adrenal hyperplasia, or carcinoma
- The adrenal tumor produces cortisol autonomously, without needing ACTH
- This autonomously produced cortisol suppresses the pituitary via negative feedback
- Result: decreased ACTH + atrophy of the uninvolved adrenal gland (the opposite gland shrinks)
- Key exam distinction: ACTH is LOW, cortisol is HIGH
c) Pituitary Cushing's Disease (~60-70% of endogenous cases)
- Caused by an ACTH-secreting pituitary adenoma (almost always a microadenoma, too small to cause mass effects)
- The excess ACTH drives both adrenal glands to overproduce cortisol
- Result: bilateral adrenal hyperplasia (both glands enlarge)
- ACTH is HIGH, cortisol is HIGH
- 4x more common in women, peak age 20-40 years
- This is specifically called "Cushing's disease" - the term "disease" is reserved for the pituitary adenoma subtype
d) Paraneoplastic (Ectopic) ACTH Secretion (~10-15% of endogenous cases)
- A non-pituitary tumor produces ACTH ectopically
- Most common cause: Carcinoid tumor > Small cell carcinoma of the lung
- (Your notes say carcinoid > SCLC; Robbins states SCLC is most common, but carcinoid is more frequently associated with the classic full syndrome because SCLC progresses too fast)
- Other tumors: medullary thyroid carcinoma, pancreatic neuroendocrine tumors
- Result: bilateral adrenal hyperplasia (same mechanism as pituitary - excess ACTH drives both glands)
- ACTH is HIGH (often very high), cortisol is HIGH
Summary Table: ACTH Levels and Adrenal Morphology
| Cause | ACTH | Adrenal Morphology |
|---|---|---|
| Exogenous steroids | Low | Bilateral atrophy |
| Adrenal adenoma/carcinoma | Low | Unilateral tumor + contralateral atrophy |
| Pituitary adenoma (Cushing's disease) | High | Bilateral hyperplasia |
| Ectopic ACTH (paraneoplastic) | Very high | Bilateral hyperplasia |
Clinical Features
The mechanism diagram in your notes explains why each feature occurs:
1. Fat Redistribution (Lipid Effects)
- Cortisol increases lipid mobilization and catabolism in the extremities
- But high insulin (from cortisol-driven hyperglycemia) promotes fat storage centrally
- Results in:
- Moon facies - round, puffy face
- Buffalo hump - fat pad on upper back/posterior neck
- Truncal obesity - central fat accumulation
- Thin arms and legs - peripheral fat loss + muscle wasting
2. Glucose / Metabolic Effects
- Cortisol increases hepatic gluconeogenesis and causes insulin resistance
- Results in:
- Secondary diabetes (hyperglycemia, glycosuria, polydipsia)
- Hypokalemic metabolic alkalosis - cortisol has mild mineralocorticoid activity, causing renal K+ loss
3. Protein Catabolism (Negative Nitrogen Balance)
- Cortisol breaks down muscle protein to provide amino acids for gluconeogenesis
- Results in:
- Proximal muscle weakness (type II myofiber atrophy) - the patient cannot climb stairs or rise from a chair
- Thin extremities
- Impaired collagen synthesis causes:
- Violaceous (purple) abdominal striae - skin tears because collagen is deficient
- Thin, fragile skin - bruises easily
- Poor wound healing
4. Water and Electrolyte Disturbance
- Dependent edema - fluid retention from mineralocorticoid-like effects
- Hypertension - sodium and water retention raises blood pressure
5. Plethora (from your second image)
- Excess cortisol causes degradation and atrophy of the epidermis and underlying connective tissue
- This leads to thinning of the skin and facial plethora (a reddish-flushed appearance on the face, because the thin skin reveals the underlying blood vessels)
6. Hirsutism (from your first image)
- In ACTH-excess states (pituitary or ectopic), the excess ACTH stimulates all three zones of the adrenal cortex:
- Zona glomerulosa -> aldosterone
- Zona fasciculata -> cortisol
- Zona reticularis -> androgens
- Excess adrenal androgens cause hirsutism (male-pattern hair growth in females)
- Also causes menstrual irregularities and acne
7. Other Features
- Osteoporosis - cortisol reduces calcium absorption from the gut, increases renal calcium loss, and directly suppresses osteoblasts -> bone resorption and fractures
- Immune suppression - cortisol suppresses lymphocytes and inflammatory mediators -> increased infection risk
- Psychiatric features - mood swings, depression, psychosis
- Skin hyperpigmentation - only in ACTH-excess causes (pituitary and ectopic), because ACTH is derived from the same POMC precursor as melanocyte-stimulating hormone (MSH)
Key Exam Mnemonics
CUSHINGS to remember features:
- C - Central obesity, Collagen loss (striae)
- U - Urinary free cortisol elevated
- S - Striae, Skin thinning
- H - Hypertension, Hirsutism, Hyperglycemia
- I - Immune suppression, Infections
- N - Nitrogen balance negative (muscle wasting)
- G - Gluconeogenesis increased
- S - Secondary diabetes, Suppressed ACTH (in adrenal/exogenous types)
Sources: Robbins & Kumar Basic Pathology, pp. 754-755 | Campbell-Walsh-Wein Urology, pp. 3134-3135
This is a shared conversation. Sign in to Orris to start your own chat.