Blood supply of spinal cord
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of the blood supply of the spinal cord.
Blood Supply of the Spinal Cord
Overview
The spinal cord has a dual vascular system: an extrinsic (extramedullary) network that delivers blood to the cord, and an intrinsic (intramedullary) network that distributes it within.
Extrinsic (Extramedullary) System
Three Longitudinal Arteries
The cord is supplied by three longitudinal arteries running along its entire length:
| Artery | Number | Origin | Territory |
|---|---|---|---|
| Anterior spinal artery (ASA) | Single (1) | Anastomosis of two branches from the intracranial vertebral arteries | Anterior 2/3 of the cord |
| Posterior spinal arteries (PSA) | Paired (2) | Intracranial vertebral arteries or posterior inferior cerebellar arteries (PICA) | Posterior 1/3 of the cord |
- The ASA runs along the anterior median fissure from the level of the olivary nucleus to the tip of the conus medullaris.
- The PSAs run along the dorsal surface and also extend throughout the cord's length.
- At the conus medullaris, the ASA and PSAs are joined by an anastomosing ansa of the conus medullaris.
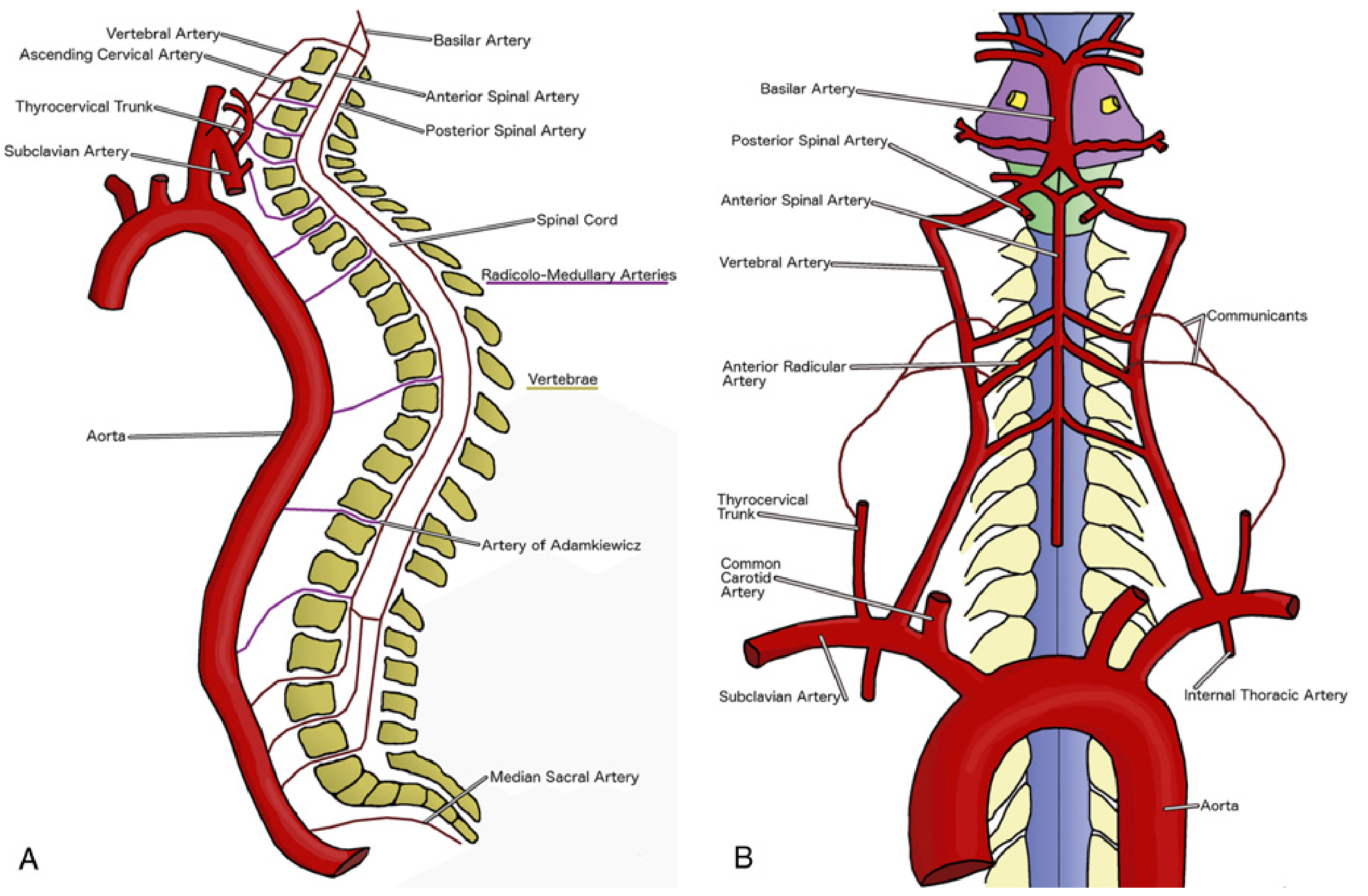
Radiculomedullary Arteries (Segmental Feeders)
The three longitudinal arteries are supplemented by radiculomedullary arteries, which arise from:
- Segmental branches of the aorta (intercostal and lumbar arteries)
- Subclavian arteries (via vertebral, ascending, and deep cervical branches)
- Hypogastric arteries
Of the 31 segmental branches that enter the spinal canal, only 6–10 reach the ASA and 10–23 reach the PSAs as true radiculomedullary vessels.
Three Vascular Zones
The cord is functionally divided into three regions with unequal blood supply:
1. Cervicothoracic Region (C1–T2) — richly vascularized
- C1–C4: supplied by the ASA with limited radiculomedullary input
- C5–T2: supplied by 2–4 large radicular arteries from the vertebral, ascending cervical, and deep cervical arteries
- The artery of the cervical enlargement (typically C4–C8, often entering with C7 or C8 root) is the most important feeder here
2. Midthoracic Region (T3–T8) — poorly vascularized (watershed zone)
- Most vulnerable to ischemia
- Receives only 1 radiculomedullary artery, usually entering with the T6, T7, or T8 root
- Fed by branches of the intercostal arteries
3. Thoracolumbosacral Region (T9–S) — richly vascularized
- The dominant feeder is the Artery of Adamkiewicz (AKA) — great anterior radicular artery / artery of the lumbar enlargement
- Usually arises from the left side (in ~75% of cases) with the T9–T12 root (75% of cases); occasionally from T6–T8 or upper lumbar roots
- It is the only major artery supplying the caudal 2/3 of the ASA — making it a critical watershed zone
- Has a characteristic "hairpin" configuration on imaging
- The sacral cord also receives supply from the median sacral artery anteriorly
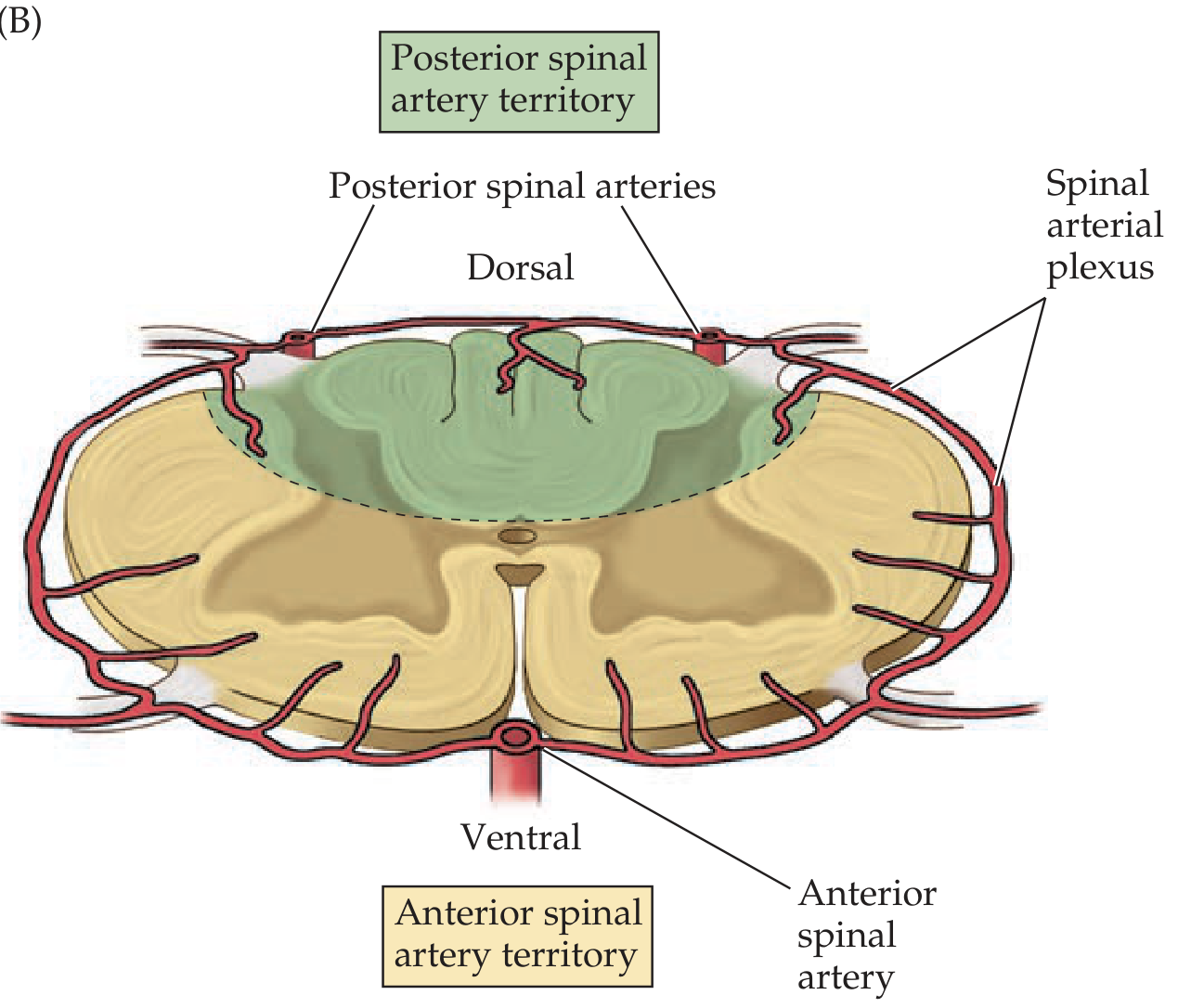
Intrinsic (Intramedullary) System
Once blood enters the three longitudinal arteries, it is distributed via:
- Sulcocommissural (central) arteries: largest branches of the ASA; enter the ventral median fissure and supply the anterior horns, lateral horns, central gray matter, and basal posterior horn
- Perforating pial branches: from the perimedullary plexus; supply white matter
- Posterior spinal arteries + perforating branches: supply dorsal horns and dorsal funiculi
Gray matter is more richly vascularized than white matter.
Clinical Relevance
Anterior Spinal Artery Syndrome
Occlusion of the ASA causes infarction of the anterior 2/3 of the cord:
- Bilateral motor loss (corticospinal tract damage → paraplegia/quadriplegia)
- Loss of pain and temperature (spinothalamic tract damage)
- Preserved vibration and proprioception (dorsal columns supplied by PSAs are spared)
Why the ASA Is More Vulnerable Than PSAs
- The single ASA receives fewer collateral feeders than the paired PSAs
- The midthoracic zone (T3–T8) is a watershed and lacks robust collaterals
- AKA occlusion (e.g., aortic surgery, dissection, atherosclerosis) can devastate the lower thoracic/lumbar cord
Aortic Surgery Risk
During thoracoabdominal aortic repair, cross-clamping can interrupt radiculomedullary feeders, particularly the AKA, causing paraplegia. The collateral network concept underpins modern neuroprotective strategies — blood can redistribute from alternate sources (subclavian, hypogastric arteries) when one segment is compromised.
Sources:
- Miller's Anesthesia, 10e — Spinal Cord Blood Supply
- Localization in Clinical Neurology, 8e — Extraspinal & Intraspinal Systems
- Neuroanatomy through Clinical Cases, 3e — Spinal Cord Blood Supply
This is a shared conversation. Sign in to Orris to start your own chat.