Lung carcinoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Searching PubMed
lung cancer treatment targeted therapy immunotherapy
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources to write a detailed, well-organized response. Let me compile this into a thorough review of lung carcinoma.
Lung Carcinoma - A Comprehensive Overview
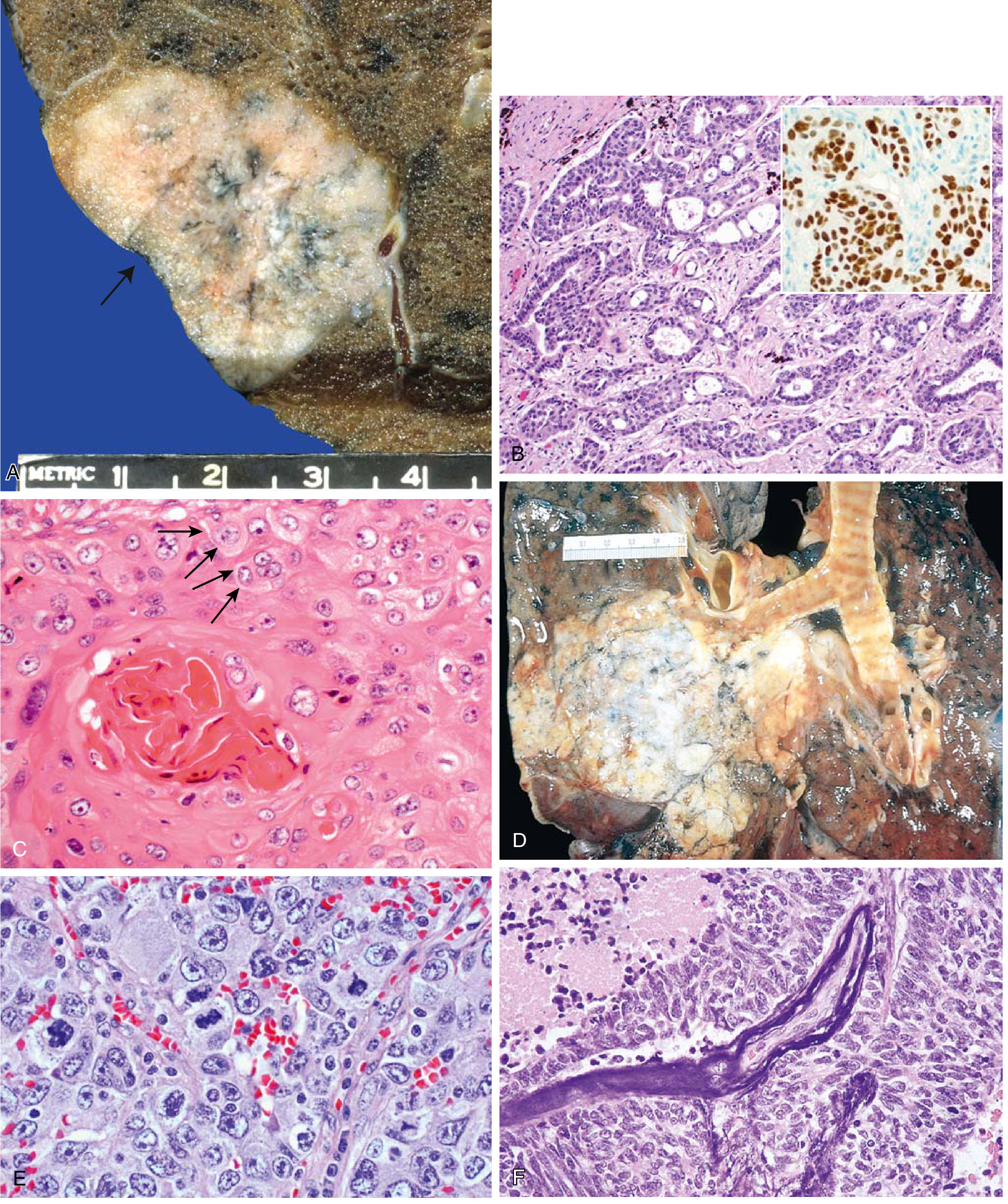
FIG. Lung carcinoma pathology: (A) Adenocarcinoma gross specimen with pleural puckering. (B) Gland-forming adenocarcinoma with TTF-1 immunostain (inset). (C) Well-differentiated squamous cell carcinoma with keratinization, pearls, and intercellular bridges. (D) Squamous cell carcinoma as a central hilar mass. (E) Large cell carcinoma. (F) Small cell carcinoma with Azzopardi effect (DNA encrustation of vessel walls from necrotic tumor cells).
Epidemiology & Risk Factors
Lung carcinoma is the leading cause of cancer-related mortality worldwide. Smoking is the single most important risk factor across all histologic types - nearly all small cell carcinomas are smoking-related, as is the majority of squamous cell carcinoma. Adenocarcinoma is the most common subtype both in smokers and in nonsmokers (particularly women), and is also the most common lung cancer overall.
Other risk factors include: radon gas exposure, asbestos (synergizes with smoking), occupational carcinogens (chromium, nickel, vinyl chloride), air pollution, and prior radiation therapy.
Classification
Lung carcinomas are divided into two major clinical groups:
Non-Small Cell Lung Carcinoma (NSCLC) - ~84% of cases
1. Adenocarcinoma (most common overall, ~40%)
- More common in women, the elderly, and nonsmokers
- Typically peripheral in location
- Arises from precursor lesions: atypical adenomatous hyperplasia → adenocarcinoma in situ (lepidic growth pattern, formerly bronchioloalveolar carcinoma) → invasive adenocarcinoma
- Lesions ≤3 cm with pure lepidic (non-invasive) growth = adenocarcinoma in situ
- Strong association with EGFR mutations (especially in nonsmokers, women, East Asian patients) and ALK fusions (~4-6%, often with signet ring morphology), KRAS mutations (~30% of adenocarcinomas)
- IHC: positive for TTF-1 and mucin
- Paraneoplastic: DIC, non-bacterial thrombotic endocarditis (hematologic syndromes)
2. Squamous Cell Carcinoma (~25-30%)
- Strongly associated with smoking
- Typically central (hilar/peribronchial), arising from the main bronchi
- Arises from squamous metaplasia → squamous dysplasia → squamous carcinoma in situ → invasive SCC
- Histology: keratinization, keratin pearls, intercellular bridges ("prickles")
- IHC: positive for p40, p63, CK5/6; negative TTF-1
- Paraneoplastic: hypercalcemia (secretes PTHrP) - most characteristic
- Cavitation is common
3. Large Cell Carcinoma (~10%)
- Diagnosis of exclusion - sheets of large pleomorphic cells with no glandular or squamous differentiation
- Peripherally located
- Poor prognosis; aggressive behavior
Small Cell Lung Carcinoma (SCLC) - ~13-15% of cases
- Arises from neuroendocrine cells (Kulchitsky cells) of the bronchial epithelium
- Almost always centrally located, hilar/perihilar
- Highly aggressive - virtually always metastatic at presentation
- Histology: small cells with scant cytoplasm, hyperchromatic "salt-and-pepper" nuclei, fine chromatin, indistinct nucleoli, diffuse sheets; Azzopardi effect (DNA encrustation of vessel walls)
- IHC: positive for chromogranin, synaptophysin, CD56 (neuroendocrine markers)
- Molecular: TP53 mutations (~90%), RB mutations (~90%), 3p deletions (~90%)
- Associated with the most paraneoplastic syndromes (see below)
Carcinoid Tumors (~1-2%)
- Low-grade neuroendocrine carcinoma; subclassified as typical and atypical
- Mean age ~40 years; 20-40% are nonsmokers
- Typical carcinoid: organoid/trabecular nests, regular round nuclei, salt-and-pepper chromatin, absent/rare mitoses, little pleomorphism; rare distant metastasis
- Atypical carcinoid: higher mitotic rate, small foci of necrosis, TP53 mutations in 20-40%, higher metastatic potential
- Often arise centrally, may cause obstructive symptoms; can produce carcinoid syndrome
Comparison: SCLC vs NSCLC
| Feature | SCLC | NSCLC |
|---|---|---|
| Microscopy | Scant cytoplasm; small hyperchromatic nuclei; diffuse sheets | Abundant cytoplasm; pleomorphic nuclei; glandular or squamous architecture |
| Neuroendocrine markers | Present (chromogranin, synaptophysin, CD56) | Absent |
| Mucin | Absent | Present in adenocarcinoma |
| TP53 mutations | ~90% | ~50% |
| RB mutations | ~90% | ~20% |
| KRAS mutations | Rare | ~30% (adenocarcinoma) |
| EGFR mutations | Absent | ~20% (adenocarcinoma, nonsmokers, women) |
| ALK fusions | Absent | 4-6% (adenocarcinoma) |
| Chemo/RT response | Often complete but invariably recurs | Incomplete response |
| Checkpoint inhibitor response | Less responsive | Responsive |
| Surgery | Rarely curative | Potentially curative (early stage) |
(Robbins & Kumar Basic Pathology, Table 11.6)
Paraneoplastic Syndromes
Approximately 3-10% of lung cancer patients develop paraneoplastic syndromes. They may precede the diagnosis of the primary tumor.
| Syndrome | Mediator | Tumor Type |
|---|---|---|
| Hypercalcemia | PTHrP | Squamous cell carcinoma (most common) |
| SIADH (hyponatremia) | ADH/vasopressin | Small cell carcinoma (most common) |
| Cushing syndrome | Ectopic ACTH | Small cell carcinoma |
| Lambert-Eaton myasthenic syndrome | Anti-VGCC antibodies | Small cell carcinoma |
| Limbic encephalitis | Anti-Hu antibodies | Small cell carcinoma |
| Subacute cerebellar degeneration | Anti-Yo/anti-Hu | Small cell carcinoma |
| Hypertrophic osteoarthropathy / clubbing | - | Any type (especially adenocarcinoma) |
| Non-bacterial thrombotic endocarditis | Mucin/hypercoagulability | Adenocarcinoma |
| DIC | Mucin/hypercoagulability | Adenocarcinoma |
Neurologic syndromes predominate with small cell carcinoma; hypercalcemia predominates with squamous cell; hematologic syndromes with adenocarcinoma.
Clinical Presentation
Local tumor effects:
- Cough, hemoptysis, dyspnea, wheezing
- Post-obstructive pneumonia / atelectasis
- Chest pain (pleural or chest wall invasion)
- Hoarseness (left recurrent laryngeal nerve compression)
- Dysphagia (esophageal compression)
Regional/mediastinal spread:
- Superior vena cava (SVC) syndrome - facial plethora, arm swelling
- Pancoast (superior sulcus) tumor - apical tumor compressing the brachial plexus (C8-T1), causing shoulder/arm pain, Horner syndrome (ptosis, miosis, anhidrosis from sympathetic chain involvement)
- Phrenic nerve palsy (diaphragm elevation)
- Pleural effusion (malignant or reactive)
Distant metastases: Brain (headache, neurologic deficits), bone (pain, pathologic fracture), liver, adrenal glands, contralateral lung
Molecular Targets & Biomarkers
NSCLC contains many actionable mutations - molecular profiling is now standard for all advanced-stage adenocarcinomas:
| Mutation/Alteration | Frequency | Targeted Agent |
|---|---|---|
| EGFR activating mutations | ~20% (adenocarcinoma, esp. nonsmokers) | Gefitinib, erlotinib, osimertinib (TKIs) |
| ALK fusion (EML4-ALK) | 4-6% | Crizotinib, alectinib, brigatinib |
| KRAS G12C | ~13% of adenocarcinoma | Sotorasib, adagrasib |
| RET fusion | ~1-2% | Selpercatinib, pralsetinib |
| NTRK fusion | ~0.2% | Larotrectinib, entrectinib |
| BRAF V600E | ~2-3% | Dabrafenib + trametinib |
| MET exon 14 skipping | ~3-4% | Tepotinib, capmatinib |
| PD-L1 expression | Variable | Pembrolizumab, atezolizumab, durvalumab |
EGFR and ALK testing is not recommended in tumors lacking any adenocarcinoma component (e.g., pure squamous cell carcinoma) - Henry's Clinical Diagnosis, p. 824-827
Recent Lancet Oncology meta-analysis (PMID: 41038207) demonstrated improved long-term overall survival with dual CTLA-4 and PD-L1/PD-1 blockade in advanced NSCLC.
Staging
NSCLC - AJCC/UICC 8th Edition TNM System
Based on data from 94,708 NSCLC cases collected by the IASLC:
T (Primary Tumor):
- T1a: ≤1 cm | T1b: >1-2 cm | T1c: >2-3 cm
- T2a: >3-4 cm | T2b: >4-5 cm
- T3: >5-7 cm OR invades chest wall/pericardium/phrenic nerve/mediastinal pleura
- T4: >7 cm OR invades mediastinum/heart/great vessels/spine/carina/trachea
N (Regional Lymph Nodes):
- N0: No lymph node involvement
- N1: Ipsilateral peribronchial / ipsilateral hilar nodes
- N2: Ipsilateral mediastinal / subcarinal nodes
- N3: Contralateral mediastinal/hilar, ipsilateral or contralateral scalene, or supraclavicular nodes
M (Metastasis):
- M0: No distant metastasis
- M1a: Separate tumor nodule in contralateral lobe; pleural/pericardial nodules or effusion
- M1b: Single extrathoracic metastasis
- M1c: Multiple extrathoracic metastases
SCLC - Limited vs Extensive Stage (VA Staging)
- Limited stage (LS): Confined to one hemithorax and regional nodes (hilar, ipsilateral and contralateral mediastinal, supraclavicular); ipsilateral pleural effusion included
- Extensive stage (ES): Beyond above; includes bilateral pulmonary involvement and pericardial involvement
- ~30-40% of patients have LS disease at diagnosis
Diagnostic Workup
Imaging:
- Chest X-ray: initial assessment
- CT chest and upper abdomen: standard for tumor extent and mediastinal nodes
- FDG-PET/CT: central role in NSCLC staging; sensitivity 84%, specificity 89% for mediastinal nodal involvement (superior to CT alone: 57% sensitivity, 82% specificity). Also guides biopsy to the most metabolically active region. A negative PET indicates low likelihood of malignancy
- Brain MRI: mandatory for suspected metastatic disease
Tissue Diagnosis:
- Bronchoscopy / BAL / endobronchial biopsy (central tumors)
- CT-guided percutaneous needle biopsy (peripheral tumors)
- EBUS-TBNA (mediastinal nodes)
- Video-assisted thoracoscopic surgery (VATS) for indeterminate nodules
- Mediastinoscopy
Laboratory:
- CBC, serum Na (SIADH), Ca (hypercalcemia), ALP, LDH
- Molecular profiling (EGFR, ALK, KRAS, RET, MET, BRAF, PD-L1) for all advanced adenocarcinomas
Treatment Summary
NSCLC
| Stage | Treatment |
|---|---|
| Stage I-II | Lobectomy (gold standard) ± adjuvant chemotherapy |
| Stage IIIA (N2) | Concurrent chemoradiation ± surgery; trimodality therapy |
| Stage IIIB-C | Definitive concurrent chemoradiation + durvalumab (maintenance) |
| Stage IV (EGFR+) | EGFR TKI (osimertinib preferred) |
| Stage IV (ALK+) | ALK inhibitor (alectinib/brigatinib) |
| Stage IV (KRAS G12C) | Sotorasib or adagrasib |
| Stage IV (PD-L1 ≥50%) | Pembrolizumab monotherapy |
| Stage IV (any PD-L1) | Chemo + pembrolizumab combination |
Bevacizumab (anti-VEGF): used in non-squamous NSCLC - contraindicated in squamous cell carcinoma due to risk of life-threatening hemorrhage.
SCLC
- Surgical resection is rarely indicated; reserved for T1-2 N0-1 tumors (< 10% of SCLC patients)
- Limited stage: Etoposide + cisplatin + concurrent thoracic radiation
- Response rate: 85-90%; complete response: 50-60%
- Median survival: 18-24 months; 2-year survival: 40-50%
- Extensive stage: Etoposide + cisplatin/carboplatin ± atezolizumab (first line)
- Response rate: 75-85%; complete response: 15-25%
- Median survival: 7-11 months; 2-year survival < 5%
- Prophylactic cranial irradiation (PCI): offered to responders (reduces brain metastasis risk)
- SCLC invariably recurs despite initial complete responses; targeted therapies and immunotherapy remain limited in benefit compared to NSCLC
Prognosis
- Overall 5-year survival for all stages combined: approximately 20-25%
- Stage I NSCLC (surgical resection): 5-year survival 70-90%
- SCLC limited stage: median survival ~18-24 months; 5-year survival ~15-25% (T1N0 resected: 30-50%)
- SCLC extensive stage: median survival 7-11 months; 5-year survival < 5%
- Small cell carcinoma overall: only 5% alive at 10 years with treatment
- High tumor mutation burden from tobacco carcinogens creates many neoantigens, explaining why NSCLC responds to immune checkpoint inhibitors
Sources:
- Robbins & Kumar Basic Pathology, Carcinoma of the Lung, p. 497
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Carcinomas of the Lung, p. 674
- Mulholland & Greenfield's Surgery 7e, Staging of Non-Small Cell Lung Carcinoma, p. 4271
- Fishman's Pulmonary Diseases and Disorders, Non-Small-Cell and Small-Cell Lung Carcinoma
- Harrison's Principles of Internal Medicine 22E, Endocrine Paraneoplastic Syndromes
- Bailey & Love's Short Practice of Surgery 28e, Bronchial (Lung) Carcinoma
This is a shared conversation. Sign in to Orris to start your own chat.