Sleep physiology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"sleep physiology"[MeSH Terms] AND "review"[pt]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have very rich content from multiple authoritative textbooks. Let me compile the comprehensive answer.
Sleep Physiology
Definition
Sleep is an active, reversible state of unconsciousness in which the brain is relatively more responsive to internal than external stimuli. It is not passive rest - the brain remains highly active, with distinct patterns of neural firing, hormone secretion, and metabolic activity across its stages.
- Miller's Anesthesia, 10e
1. Measurement: Polysomnography (PSG)
The standard method for defining sleep is polysomnography, the continuous recording of:
- EEG (electroencephalogram) - brain electrical activity
- EOG (electrooculogram) - eye movements
- EMG (electromyogram) - muscle tone (chin and legs)
Supplemented clinically by nasal airflow sensors, pulse oximetry, respiratory effort bands, and body position sensors.
PSG defines two fundamental sleep states: REM and NREM sleep.
- Harrison's Principles of Internal Medicine, 22e
2. Sleep Stages
NREM Sleep
NREM is divided into three stages of progressively deepening sleep:
| Stage | Old Name | EEG Features | Characteristics |
|---|---|---|---|
| N1 | Stage 1 | Low-voltage, mixed frequency; loss of alpha waves | Light sleep; slow, roving eye movements; easy arousal |
| N2 | Stage 2 | Sleep spindles (12-14 Hz bursts, 0.5-2 s); K-complexes (vertex waves) | Majority of total sleep time |
| N3 | Stages 3/4 (slow-wave sleep) | Delta waves predominate (high-amplitude, low-frequency) | Deepest NREM; hardest to arouse; most restorative |
N3 ("slow-wave sleep" or SWS) is the most restorative stage and predominates in the first third of the night.
REM Sleep
-
EEG: low-amplitude, mixed-frequency (resembles N1 or even wakefulness)
-
Rapid, saccadic eye movements in bursts
-
Skeletal muscle atonia (brainstem-mediated paralysis of all muscles except respiratory muscles)
-
Associated with vivid dreaming and phasic muscle twitches
-
Predominates in the last third of the night
-
Harrison's Principles of Internal Medicine, 22e; Adams and Victor's Principles of Neurology, 12e
3. Sleep Architecture (Hypnogram)
Normal adult sleep shows a consistent nightly pattern:
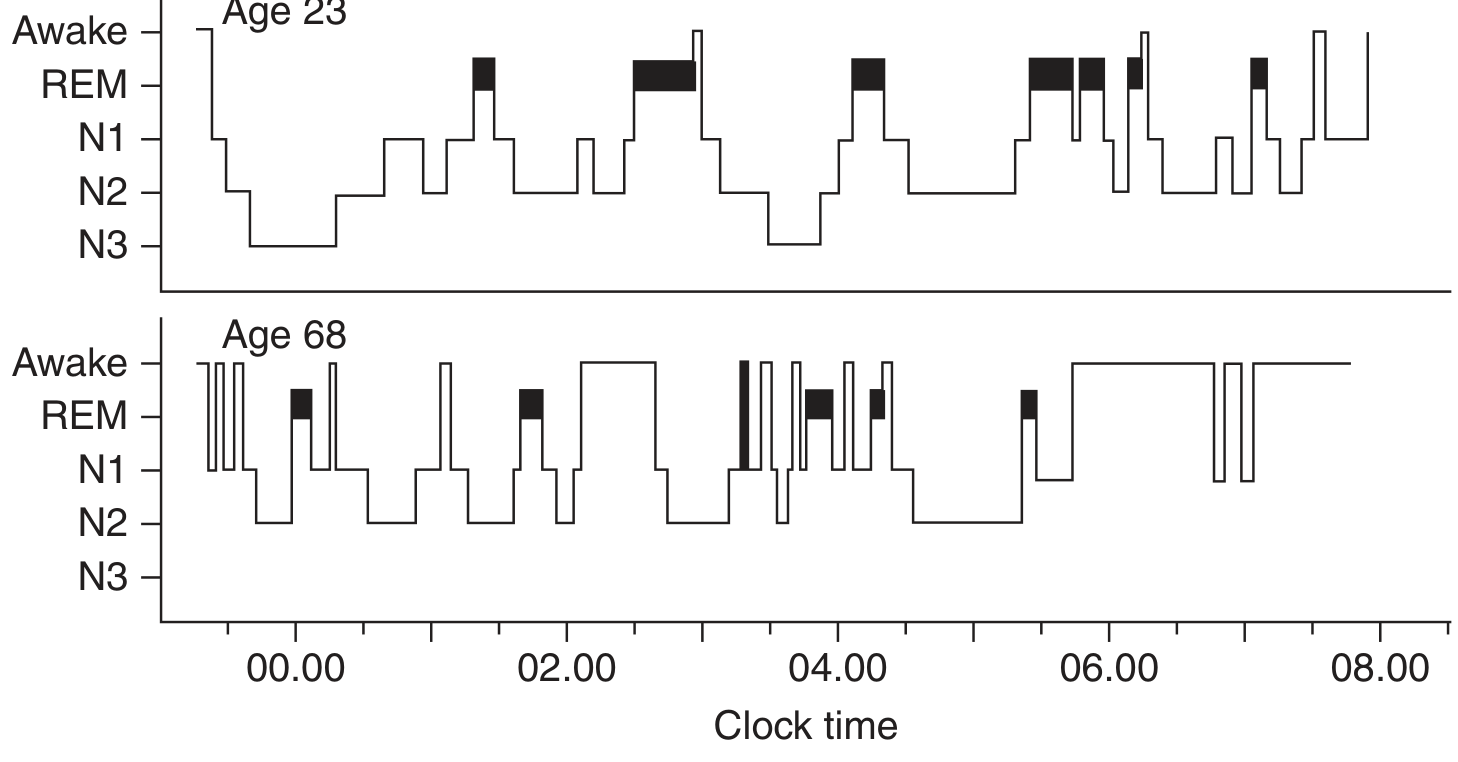
FIGURE: Wake-sleep hypnogram comparing a 23-year-old (top) and 68-year-old (bottom). Note the prominent N3 slow-wave sleep early in the night in the young adult, and the REM periods (dark blocks) lengthening toward morning. The older adult shows absent N3, frequent awakenings, and fragmented architecture. - Harrison's Principles of Internal Medicine, 22e
Key features:
- Sleep onset: Rapid descent through N1 → N2 → N3 within 45-60 minutes
- N3 dominates the first third of the night
- First REM episode appears in the second hour of sleep
- NREM/REM cycle ("ultradian cycle") repeats every 60-160 minutes
- 4-6 cycles per night in a typical 7-8 hour sleep
- REM episodes lengthen toward morning; N3 progressively shortens
Proportions in healthy young adults:
- N1 + N2: ~50-60% of total sleep
- N3: ~15-25%
- REM: ~20-25%
4. Circadian Regulation and the Two-Process Model
Sleep timing is governed by two interacting systems:
Process C - Circadian Drive
The suprachiasmatic nucleus (SCN) of the hypothalamus is the master biological clock. It:
- Generates an intrinsic ~24-25 hour rhythm independent of environment
- Is entrained to the 24-hour day by light input from retinal photoreceptors
- Integrates light/dark signals to synchronize activity, temperature, hormone secretion, and gene expression
- About 15% of all human genes show daily circadian expression rhythms
Melatonin, secreted by the pineal gland at night and suppressed by retinal light stimulation, is a key output signal of the SCN. Chronotype (morning vs. evening preference) reflects individual variation in the circadian clock.
Process S - Homeostatic Sleep Pressure
During wakefulness, adenosine and other sleep-promoting substances progressively accumulate in the brain, building "sleep pressure." This pressure is discharged during sleep. The SCN circadian wake drive offsets Process S during daytime hours; as it diminishes in the evening, sleep pressure becomes irresistible.
- Miller's Anesthesia, 10e; Adams and Victor's Principles of Neurology, 12e
5. Neural Control of Sleep and Wakefulness
The Ascending Arousal System (Wakefulness)
Multiple brainstem nuclei release wake-promoting neurotransmitters:
- Locus coeruleus - norepinephrine
- Raphe nuclei - serotonin
- Tuberomammillary nucleus (TMN) - histamine (major source of brain histamine; H1 antihistamines cause sedation by blocking this)
- Pedunculopontine/laterodorsal tegmental nuclei - acetylcholine
- Basal forebrain - acetylcholine
These project to the thalamus, basal forebrain, and cortex to maintain arousal.
Orexin (Hypocretin) - The Stabilizer
Orexinergic neurons in the lateral hypothalamus are critical for maintaining stable wakefulness. They:
- Provide excitatory input to all arousal system nuclei
- Stabilize the sleep-wake switch against unintended transitions
- Loss of orexin neurons causes narcolepsy (sudden attacks of sleep/cataplexy)
- Suvorexant and other dual orexin receptor antagonists block OX2R to promote sleep
The Sleep Switch - VLPO
The ventrolateral preoptic nucleus (VLPO) and median preoptic nucleus (MnPO) of the anterior hypothalamus are the main sleep-promoting areas. They fire at high frequency during sleep and send GABAergic/galaninergic inhibitory projections to all arousal nuclei.
The Flip-Flop Switch Model
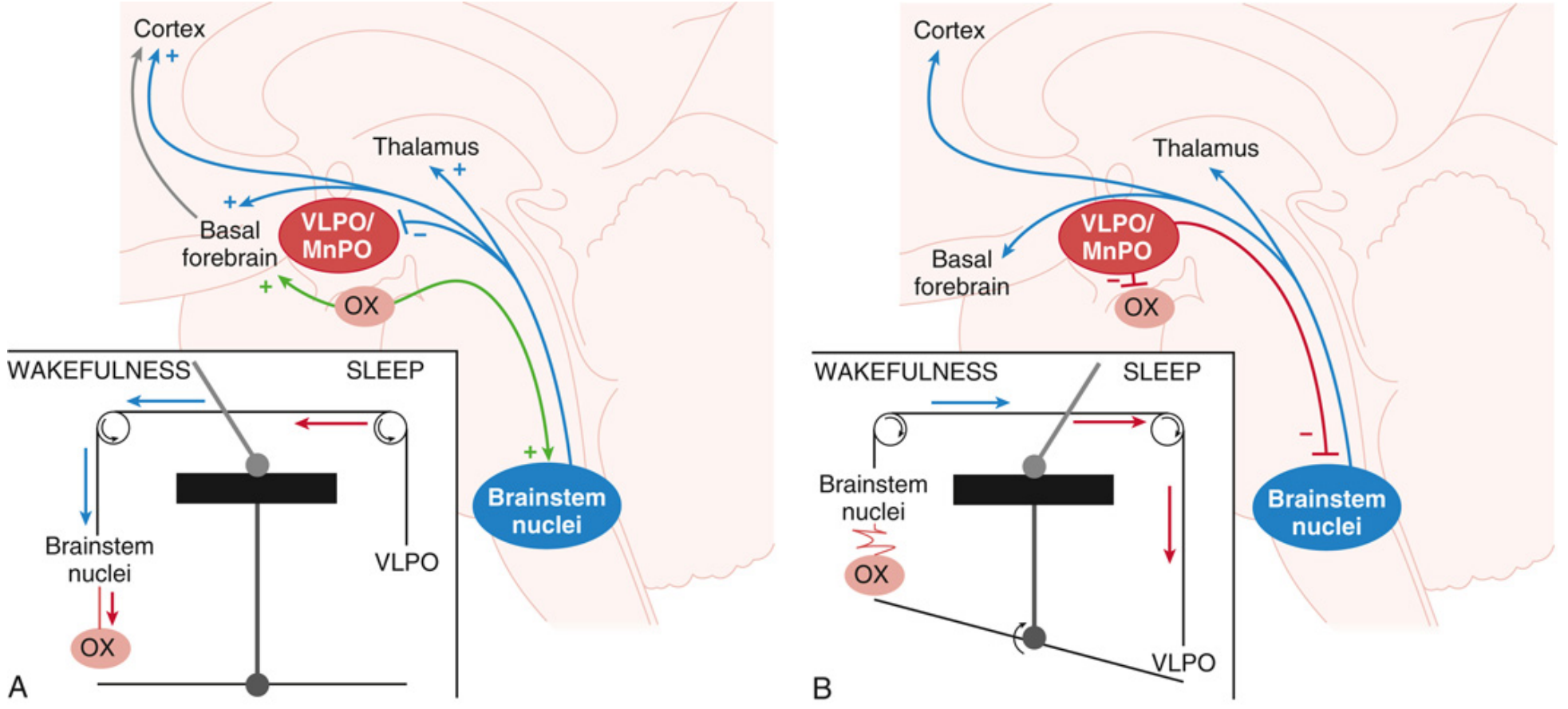
FIGURE: The flip-flop switch model (Saper et al.). During wakefulness (A), brainstem arousal nuclei excite the thalamus and cortex while inhibiting VLPO/MnPO. Orexin reinforces this state. During sleep (B), VLPO/MnPO neurons inhibit the brainstem arousal nuclei and orexin neurons; the switch "flops" to sleep. The mutual inhibition ensures rapid, stable transitions - not gradual drifts. - Miller's Anesthesia, 10e
NREM-REM Switch
A second flip-flop switch in the pons governs NREM-REM transitions:
- REM-on neurons: Sublaterodorsal nucleus (glutamatergic + GABAergic) - promotes REM
- REM-off neurons: Ventrolateral periaqueductal gray / lateral pontine tegmentum - suppresses REM
- Mutual inhibition between these two groups generates the cycling REM/NREM switch
The muscle atonia of REM is mediated by glycinergic and GABAergic inhibition of spinal motor neurons, driven from the sublaterodorsal nucleus.
- Adams and Victor's Principles of Neurology, 12e; Miller's Anesthesia, 10e
6. Physiological Changes During Sleep
Cardiovascular
- NREM (especially N3): Reduced heart rate, reduced blood pressure, reduced sympathetic tone ("nocturnal dip")
- REM: Increased sympathetic tone; blood pressure and heart rate fluctuate. Loss of the nocturnal dip (e.g., from sleep apnea) is associated with daytime hypertension and increased cardiovascular risk
Respiratory
- Breathing slows and becomes more regular in NREM
- Respiratory rate is more irregular in REM
- Upper airway muscle tone is reduced during sleep, predisposing to obstructive sleep apnea
Renal
- Urine output decreases (increased ADH secretion); urine osmolality increases
Endocrine (Key Relationships)
| Hormone | Relationship to Sleep |
|---|---|
| Growth hormone | Major surge in first 2 hours, during N3 slow-wave sleep |
| Cortisol | Peaks in early morning; high on awakening |
| TSH (thyroid-stimulating hormone) | Peaks at sleep onset |
| Melatonin | Produced throughout night; suppressed by morning light |
| Prolactin | Rises during sleep; highest concentration shortly after sleep onset |
| LH | Sleep-associated increase in pubertal boys and girls |
| Testosterone | Circadian + sleep-stage dependent secretion |
Other
-
Penile erections occur periodically during REM sleep (basis of NPT testing)
-
Temperature regulation is impaired during REM (ectothermic state)
-
Adams and Victor's Principles of Neurology, 12e
7. Effects of Age on Sleep
| Age Group | Sleep Characteristics |
|---|---|
| Neonate | 16-20 h/day; ~50% REM sleep |
| Child | 10-12 h/day; fragmented over multiple episodes |
| Adolescent | 9-10 h; N3 decreases after puberty |
| Young adult | 7-8 h; 20-25% REM, 15-25% N3 |
| >65 years | ~6-6.5 h; N3 may be absent; frequent nocturnal awakenings; fragmented sleep |
Women tend to sleep slightly more than men from age ~35 onward. The ultradian sleep cycle matures into the adult REM-NREM pattern over the first year of life.
- Adams and Victor's Principles of Neurology, 12e; Harrison's Principles of Internal Medicine, 22e
8. Sleep Deprivation Effects
- Degrades cognitive performance, particularly sustained vigilance and reaction time
- Young adults are especially susceptible to slowed reaction times
- Sleep deprivation increases sleep pressure, leading to faster sleep onset and increased N3 intensity on recovery nights
- Chronic sleep deprivation is linked to metabolic, cardiovascular, psychiatric, and immune dysfunction
Summary Table: REM vs. NREM
| Feature | NREM (N1/N2/N3) | REM |
|---|---|---|
| EEG | Slowing; spindles, K-complexes, delta waves | Low-amplitude, mixed frequency |
| Eye movements | Slow, roving (N1); absent (N2/N3) | Rapid, saccadic |
| Muscle tone | Gradually reduced | Absent (atonia) |
| Dreams | Rare, thought-like | Vivid, narrative |
| Heart rate/BP | Reduced | Variable, fluctuating |
| Growth hormone | Secreted during N3 | Not prominent |
| % of night | ~75-80% | ~20-25% |
| Timing in night | First third | Last third |
Sources: Harrison's Principles of Internal Medicine 22e | Adams and Victor's Principles of Neurology 12e | Miller's Anesthesia 10e
Make the topic for USMLe type
This is a shared conversation. Sign in to Orris to start your own chat.