Hyperacidity
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full, detailed response.
Hyperacidity (Acid Peptic Disease)
Hyperacidity refers to excess gastric acid production beyond what the gastroduodenal mucosal defense can safely neutralize. Clinically it encompasses a spectrum from functional dyspepsia and gastritis to peptic ulcer disease (PUD) and gastroesophageal reflux disease (GERD).
Physiology of Gastric Acid Secretion
Gastric acid (HCl) is produced by parietal cells in the oxyntic (corpus) mucosa. Three major stimuli converge on these cells:
| Stimulus | Receptor | Second Messenger |
|---|---|---|
| Histamine (from enterochromaffin-like cells) | H₂ receptor | ↑ cAMP via Gs protein |
| Gastrin (from G cells in antrum) | CCK-B receptor | ↑ Ca²⁺ |
| Acetylcholine (vagal stimulation) | M₃ muscarinic receptor | ↑ Ca²⁺ |
All three pathways ultimately activate the H⁺/K⁺-ATPase proton pump on the apical (luminal) surface of the parietal cell, secreting H⁺ in exchange for K⁺. Histamine is the dominant physiological mediator - blocking H₂ receptors inhibits acid responses to gastrin and vagal stimulation as well.
The mucosal defense against acid includes:
- Mucus-bicarbonate barrier
- Mucosal blood flow
- Tight epithelial junctions
- Prostaglandins (PGE₂, PGI₂) that stimulate mucus and bicarbonate
Hyperacidity arises when acid production exceeds mucosal defense capacity.
Causes and Risk Factors
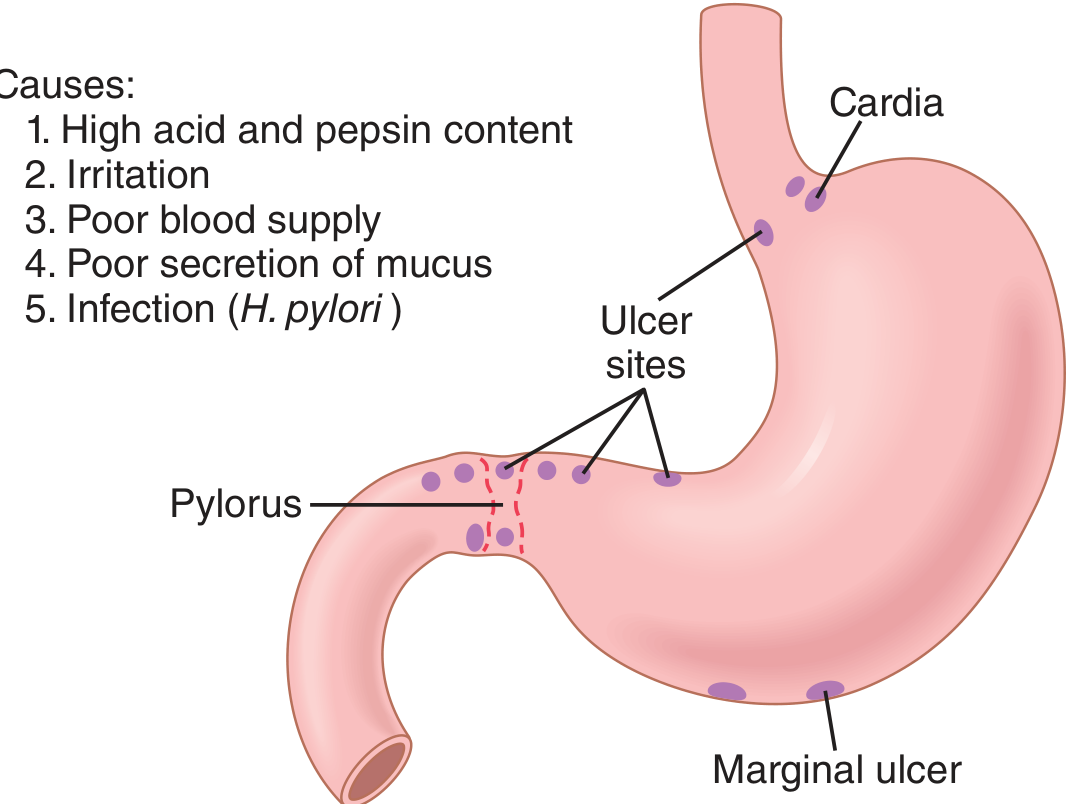
1. Helicobacter pylori Infection (most common cause)
- Gram-negative spiral bacterium colonizing the gastric mucosa
- Produces urease (splits urea → NH₃, buffering local acid and allowing survival)
- Causes antral-predominant gastritis → reduces somatostatin → removes inhibition of gastrin → gastric hyperacidity
- If infection destroys oxyntic glands, hypoacidity results instead (a paradox in advanced disease)
- Prevalence: ~50% of people >65 years in Western countries; near-universal in developing countries
2. NSAIDs and Aspirin
- Inhibit COX-1 → reduced prostaglandin synthesis → impaired mucus and bicarbonate secretion, reduced mucosal blood flow
- Break down the mucosal barrier even when acid levels are normal
- Account for a disproportionately large fraction of bleeding ulcers
3. Hypergastrinemic Syndromes
- Zollinger-Ellison Syndrome (ZES): gastrinoma (usually pancreatic/duodenal) secreting excess gastrin → massive acid hypersecretion → recurrent, multiple, atypical ulcers
- Other causes: retained gastric antrum after surgery, G-cell hyperplasia, short bowel syndrome
4. Hyperhistaminic Syndromes
- Systemic mastocytosis, basophilic leukemia - persistent histamine elevation chronically stimulates parietal cells
5. Stress Ulcers
- Severe illness (trauma, burns, sepsis, head injury, mechanical ventilation) → mucosal ischemia + hypersecretion
- Cushing ulcers (head injury) - strongly acid-mediated
- Curling ulcers (burns) - primarily ischemic
6. Lifestyle and Other Factors
- Smoking, alcohol
- High-dose corticosteroids (with NSAIDs synergistically)
- Ischemia of the upper GI tract (celiac/SMA stenosis)
- Cameron ulcers (large hiatal hernias)
- Rebound hyperacidity after PPI cessation
Clinical Features
| Symptom/Sign | Details |
|---|---|
| Epigastric pain/burning | Classically postprandial (gastric ulcer) or relieved by food/antacids (duodenal ulcer) |
| Heartburn/GERD symptoms | Retrosternal burning, acid regurgitation, waterbrash |
| Nausea and vomiting | Especially with outlet obstruction |
| Bloating, belching | Common in functional dyspepsia |
| Anorexia, early satiety | Gastric ulcer |
| Hematemesis/melena | Complication - bleeding ulcer (most common complication, ~1 in 6 patients over disease course) |
| Weight loss | Gastric cancer must be excluded |
Alarm features requiring urgent endoscopy: hematemesis, melena, unexplained weight loss, dysphagia, vomiting, age >55 with new onset dyspepsia, palpable mass.
Diagnosis
Endoscopy (gold standard)
- A peptic ulcer is a mucosal defect ≥0.5 cm penetrating the muscularis mucosae; smaller defects are erosions
- Gastric ulcers: mainly lesser curvature, transitional zone
- Duodenal ulcers: anterior/posterior wall of duodenal bulb; "kissing ulcers" when both walls involved
- Biopsy mandatory for all gastric ulcers to exclude malignancy; not routinely needed for duodenal ulcers
Testing for H. pylori
| Method | Notes |
|---|---|
| Rapid urease test (biopsy) | High positive predictive value; false-negatives with PPIs/antibiotics |
| Histology (H&E) | Sensitive and specific; standard at endoscopy |
| Culture | For antimicrobial susceptibility in refractory cases |
| Serology | Simple, inexpensive; cannot confirm eradication (antibodies persist >6-12 months) |
| Stool antigen test | Accurate; useful for eradication confirmation |
| ¹³C/¹⁴C urea breath test | Noninvasive; wait ≥6-8 weeks post-therapy to avoid false-negatives |
Gastric Acid Tests
- Basal acid output (BAO) and peak acid output (PAO) - used primarily when ZES is suspected
- Serum gastrin levels - markedly elevated in ZES (>1000 pg/mL strongly suggestive)
Treatment
1. Proton Pump Inhibitors (PPIs) - First Line
Mechanism: Irreversibly bind H⁺/K⁺-ATPase on the parietal cell canalicular membrane, blocking the final common pathway of acid secretion.
| Drug | Typical Dose |
|---|---|
| Omeprazole | 20-40 mg once daily |
| Pantoprazole | 40 mg once/twice daily |
| Esomeprazole | 20-40 mg once/twice daily |
| Lansoprazole | 30 mg once daily |
| Rabeprazole | 20 mg once daily |
- Must be taken 30-60 minutes before meals (require activation by acid in the secretory canaliculus)
- For Zollinger-Ellison syndrome: high-dose PPIs (esomeprazole 40 mg twice daily or more)
- Long-term concerns: GI and respiratory infections, vitamin B12 deficiency, hypomagnesemia, rebound hyperacidity on cessation
2. H₂-Receptor Antagonists
Mechanism: Competitive blockade of H₂ receptors on parietal cells → ↓ cAMP → reduced acid secretion.
- Famotidine, ranitidine (withdrawn in many markets), cimetidine, nizatidine
- Prevention of NSAID ulcers: famotidine 40 mg twice daily needed for gastric ulcer prevention
- Less potent than PPIs but useful for mild-moderate disease and stress ulcer prophylaxis in ICU
3. Antacids
- Neutralize secreted acid directly (Al(OH)₃, Mg(OH)₂, CaCO₃)
- Rapid symptom relief, short duration
- Adjunct therapy; not for ulcer healing
4. H. pylori Eradication (Triple Therapy - standard first-line)
PPI + amoxicillin 1g bd + clarithromycin 500 mg bd × 14 days
Alternative regimens:
- Bismuth quadruple therapy: PPI + bismuth + metronidazole + tetracycline (used in clarithromycin-resistant areas or second-line)
- Concomitant/Sequential/Hybrid regimens in high-resistance settings
Eradication confirmation: urea breath test or stool antigen at ≥6-8 weeks post-therapy.
5. Cytoprotective Agents
- Sucralfate: polymerizes in acid to form protective coat over ulcer base; no systemic absorption
- Misoprostol (PGE₁ analogue): stimulates mucus and bicarbonate, reduces acid; used for NSAID-ulcer prevention; side effects (diarrhea) limit adherence
6. Lifestyle Modifications
- Avoid NSAIDs/aspirin if possible (switch to paracetamol)
- Avoid smoking (impairs ulcer healing)
- Limit alcohol
- Small, frequent meals; avoid spicy/acidic food triggers
- Elevate head of bed for GERD
Prevention
| Scenario | Strategy |
|---|---|
| NSAID use + high ulcer risk | PPI (omeprazole 20 mg/day) or misoprostol 400-800 mg/day |
| Low-dose aspirin + high risk | PPI or H2-blocker |
| ICU stress ulcer prophylaxis | PPI or H2-blocker (roughly equally effective) |
| H. pylori-positive after ulcer | Mandatory eradication |
| Continuing NSAIDs after ulcer | Switch to COX-2 inhibitor + PPI |
Complications
| Complication | Key Points |
|---|---|
| Hemorrhage | Most common; 40-60% of upper GI bleeds; endoscopic hemostasis + high-dose IV PPI |
| Perforation | Surgical emergency; free air under diaphragm on CXR |
| Pyloric stenosis/obstruction | Repeated vomiting, succussion splash; balloon dilation or surgery |
| Malignant transformation | Gastric ulcers (not duodenal); mandatory biopsy and follow-up endoscopy |
Special Syndromes
Zollinger-Ellison Syndrome: Gastrinoma → massive hyperacidity → atypical/multiple ulcers in duodenum, jejunum; associated with MEN-1. Diagnosed by fasting serum gastrin >1000 pg/mL and secretin stimulation test. Treated with high-dose PPIs; surgery for resectable tumors.
Sources: Goldman-Cecil Medicine (Chapter 125) | Guyton & Hall Medical Physiology (Chapter 67) | Goodman & Gilman's Pharmacological Basis of Therapeutics (Chapter 43/53)
This is a shared conversation. Sign in to Orris to start your own chat.