A two-month-old child presented with persistent cough and fever for three days, and he is not feeding well. What is the diagnosis?
Reading File
Finding Sources
Finding Sources
Searching PubMed
bronchiolitis infant diagnosis clinical features
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of this clinical case:
Diagnosis: Bronchiolitis (most likely RSV-related)
A 2-month-old with persistent cough, fever (x3 days), and poor feeding fits the classic presentation of viral bronchiolitis, with RSV (Respiratory Syncytial Virus) being the most common causative agent.
Why Bronchiolitis?
| Feature | This Patient | Bronchiolitis |
|---|---|---|
| Age | 2 months | Most common in first 2 years of life |
| Cough | Present | Cardinal symptom |
| Fever | Present | Variable, commonly present |
| Poor feeding | Present | Classic - due to respiratory distress and fatigue |
| Duration | 3 days | Acute illness typically lasts 10-14 days |
"Bronchiolitis is a viral lower respiratory tract infection that is common during the first 2 years of life. RSV is the most common infectious agent..."
- Swanson's Family Medicine Review
Pathophysiology
RSV and other viruses (influenza, adenovirus, parainfluenza, human metapneumovirus) cause:
- Inflammation, edema, and necrosis of the epithelial lining of small airways
- Increased mucus production and bronchospasm
- Resulting in wheeze, cough, accessory muscle use, tachypnea, and rhinorrhea
The incubation period for RSV is 4-6 days, followed by rhinitis that progresses over 1-3 days to bronchiolitis and pneumonitis, with cough, wheezing, and respiratory distress.
Additional Signs to Look For
- Tachypnea (RR >60)
- Intercostal/subcostal retractions and nasal flaring
- Wheeze or fine crackles on auscultation
- Hypoxemia (O2 sat <90% in severe cases)
- Hyperinflated chest on X-ray (air trapping)
Chest X-Ray Findings
In severe cases, CXR shows bilateral interstitial infiltrates, lung hyperexpansion, and possible atelectasis:
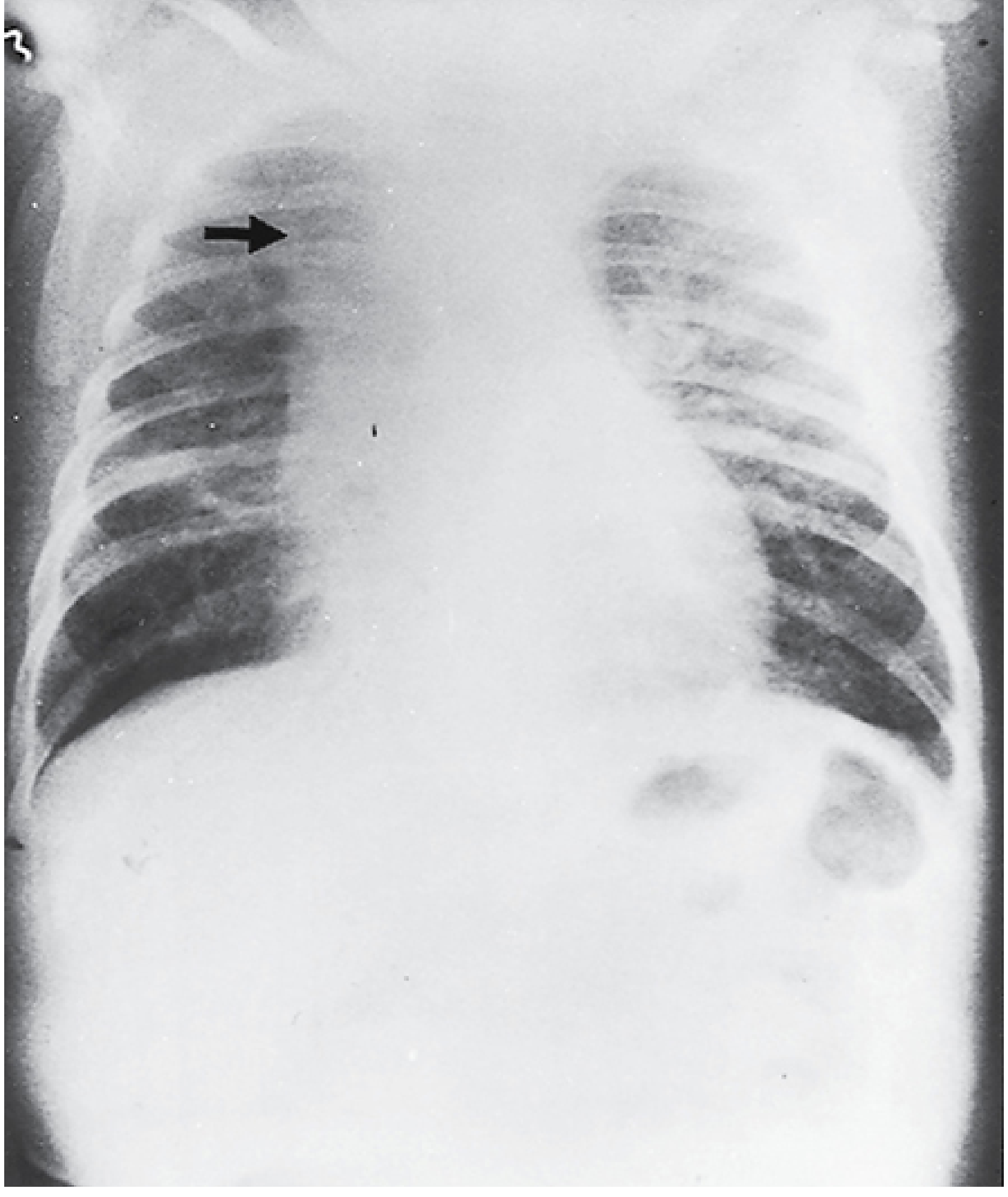
Chest radiograph of an infant with severe RSV pneumonia and bronchiolitis. Note bilateral interstitial infiltrates, hyperexpansion, and right upper lobe atelectasis (arrow). - Sherris & Ryan's Medical Microbiology
Differential Diagnoses to Consider
- Bacterial pneumonia - more likely if focal consolidation on CXR, toxic appearance, WBC markedly elevated
- Pertussis (whooping cough) - at 2 months, partially or unvaccinated; paroxysmal cough, post-tussive vomiting, whoop
- Viral pneumonitis - often co-exists with bronchiolitis
- Congenital heart disease - poor feeding + respiratory symptoms, but usually without fever
- Chlamydia trachomatis pneumonia - afebrile pneumonia in this age group (but fever here makes it less likely)
Management (Evidence-Based)
Treatment is primarily supportive - no treatment shortens the course:
- Hydration: IV fluids if not tolerating feeds (poor feeding + RR >60-70 = aspiration risk)
- Supplemental oxygen: if SpO2 persistently <90%
- Nasal suctioning: provides temporary relief
- NOT recommended: routine bronchodilators, corticosteroids, antibiotics, or chest physiotherapy
- Antibiotics only if: confirmed bacterial coinfection (positive culture, AOM with bulging TM, consolidation on CXR)
Hospital admission is warranted for this infant given the age (<3 months is a high-risk criterion), poor feeding, and 3-day course.
Prevention
- Palivizumab (15 mg/kg IM monthly x5): for high-risk infants (premature, congenital heart disease, chronic lung disease, immunodeficiency)
- Strict hand hygiene and contact precautions in hospital settings
Sources:
- Swanson's Family Medicine Review, p. 583
- Red Book 2021 - Report of the Committee on Infectious Diseases (AAP), pp. 977-980
- Sherris & Ryan's Medical Microbiology, 8th ed., p. 352
In ear lens procedure till wat tome to have the eye drops
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
post cataract surgery IOL eye drops duration how long to use
Here is a clear guide on post-operative eye drops after intraocular lens (IOL) / cataract surgery:
Eye Drops After IOL (Cataract) Surgery - Duration Guide
There are typically 3 types of eye drops prescribed, each used for a different duration:
1. Antibiotic Eye Drops
Purpose: Prevent infection (endophthalmitis)
Duration: 1-2 weeks after surgery
- Usually started 1-2 days before surgery
- Used several times daily in the first week
- Discontinued once infection risk has passed (usually by day 7-14)
- Note: Many modern surgeons now inject antibiotics directly into the eye at time of surgery, so post-op antibiotic drops may not always be required
2. Anti-inflammatory Eye Drops (Steroid + NSAID)
Purpose: Reduce inflammation and prevent cystoid macular oedema (CMO) - a common post-op complication
| Type | Duration |
|---|---|
| Corticosteroid (e.g., prednisolone, dexamethasone) | 4-6 weeks, tapered gradually |
| NSAID (e.g., ketorolac, nepafenac, diclofenac) | 4-6 weeks |
- These are the most important drops to complete fully
- Often started 2 days before surgery
- The dose is tapered: e.g., 4x/day for week 1-2, then 2x/day, then 1x/day before stopping
- Do NOT stop abruptly without your surgeon's instruction - stopping early risks rebound inflammation
3. Lubricating / Artificial Tear Drops
Purpose: Relieve dryness and grittiness (surgery temporarily affects corneal nerves)
Duration: Several months as needed - can be continued long-term if comfortable
- These are not medicated and are safe to use freely
- Most patients need them for 1-3 months
General Timeline Summary
| Period | What to use |
|---|---|
| 2 days before surgery | Start antibiotic + NSAID drops |
| Day of surgery | Continue as instructed |
| Week 1-2 | All three types, highest frequency |
| Weeks 2-4 | Taper steroids/NSAIDs, continue lubricants |
| Weeks 4-6 | Finish steroid/NSAID course |
| Beyond 6 weeks | Lubricants only as needed |
Important Tips
- Wait 5-10 minutes between different eye drops - do not put multiple drops in at once
- Always wash hands before applying
- Do not touch the dropper tip to your eye or eyelid
- If you run out early, contact your doctor - do not stop halfway through a course
- Report any sudden pain, vision loss, redness, or discharge immediately
The exact schedule always depends on your surgeon's instructions. Some surgeons have different protocols, especially if a combined antibiotic-steroid drop is used. Always follow what you have been specifically prescribed.
Wat to do in sncu ward as an fmg intern
Reading File
Finding Sources
Finding Sources
Searching the Web
SNCU special newborn care unit intern duties FMG India responsibilities
Finding Sources
Finding Sources
Searching the Web
SNCU intern responsibilities duties neonatal ward India clinical procedures monitoring
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading Web Page
https://nhm.hp.gov.in/storage/app/media/uploaded-files/SNCU%…
Here is a practical and detailed guide on what you do as an FMG intern in the SNCU (Special Newborn Care Unit):
Your Role as an FMG Intern in the SNCU
The SNCU is a secondary-level neonatal unit (12+ beds) at district hospitals and medical colleges that manages sick and small newborns - all care except mechanical ventilation and major surgery. As an intern, you work under the supervising pediatrician/neonatologist.
1. Admission & Triage
Know which babies get admitted to SNCU - this is your first responsibility:
From the delivery room / inborn:
- Birth weight <1800 g and/or <34 weeks (minimum 24 hours observation)
- APGAR score <6 at 1 minute / gasping / delayed cry
- Respiratory distress (tachypnea, grunt, retractions, central cyanosis)
- Asphyxia / suspected HIE (Hypoxic Ischemic Encephalopathy)
- Symptomatic hypoglycemia
- Suspected sepsis (unstable)
- Major congenital anomalies requiring monitoring
From community (babies <28 days):
- Delayed cry >5 minutes
- Respiratory distress, central cyanosis or spells
- Bile-stained vomiting
- Abdominal distension
- Suspected sepsis - unstable baby
- Unstable baby with congenital abnormality
2. Daily Ward Rounds (Morning and Evening)
For each baby, you assess and document:
| Parameter | What to check |
|---|---|
| Temperature | Axillary - normal 36.5-37.5°C; watch for hypothermia in preterm |
| Heart rate | Normal 120-160 bpm |
| Respiratory rate | Normal 40-60/min; >60 = tachypnea |
| SpO2 | Target 90-95% in preterm, >95% in term |
| Blood glucose | Heel prick glucometry; maintain >45 mg/dL |
| Weight | Daily weight; expect 10% loss in first week, then regain by day 10-14 |
| Feeds | Volume, tolerance, vomiting, gastric residuals |
| Urine output | >1 mL/kg/hr |
| Jaundice | Clinical assessment + TSB levels; monitor under phototherapy |
| IV access | Check cannula site for phlebitis, infiltration |
| Umbilicus | Redness, discharge (signs of omphalitis) |
3. Clinical Procedures (Learn and Practice)
| Procedure | Notes |
|---|---|
| Heel prick / glucometry | Every 4-6 hours in at-risk babies |
| IV cannulation | Peripheral; use dorsum of hand or foot |
| NG tube insertion | For feeding in sick/preterm neonates unable to suck |
| Bag and mask ventilation | Neonatal resuscitation - use 250 mL bag, proper seal |
| Phototherapy setup | Ensure correct distance (30-35 cm), eye patches, cover gonads |
| Blood collection | Venous or heel prick for CBC, CRP, blood culture, bilirubin |
| Umbilical venous catheter (UVC) | Observed/assisted - emergency vascular access |
| Kangaroo Mother Care (KMC) | Counsel and assist mother; skin-to-skin for stable preterm |
| OGT feeds | Orogastric tube for feeding in very small/sick neonates |
4. Key Conditions to Manage (Know These Well)
Neonatal Sepsis
- Early onset (<72 hrs): GBS, E.coli, Listeria
- Late onset (>72 hrs): Staph aureus, Klebsiella, Pseudomonas (nosocomial)
- Work-up: CBC, CRP, blood culture x2, urine culture, LP if stable
- Treatment: Ampicillin + Gentamicin (early onset); Cloxacillin + Amikacin (late onset/nosocomial)
Neonatal Jaundice
- Physiological vs pathological (onset <24 hrs = always pathological)
- Know phototherapy thresholds by age in hours and gestation
- Know exchange transfusion indications
- Investigations: TSB, direct/indirect bilirubin, blood group, Coombs test, G6PD
Respiratory Distress Syndrome (RDS) / Hyaline Membrane Disease
- Preterm babies, <34 weeks
- Grunting, retractions, cyanosis from birth
- CXR: ground glass opacification, air bronchograms
- Management: surfactant, CPAP/O2, temperature, nutrition
Hypoglycemia
- Blood glucose <45 mg/dL
- Asymptomatic: oral/NG feeds; Symptomatic: IV dextrose bolus (2 mL/kg of D10)
- At-risk: LBW, preterm, IDM (Infant of Diabetic Mother), asphyxiated
Hypothermia
- Very common in preterm/LBW
- Use radiant warmer, incubator, skin-to-skin (KMC)
- Warm the room, warm fluids, delayed baths
Birth Asphyxia / HIE
- APGAR scoring at 1 and 5 minutes
- Therapeutic hypothermia if eligible (>36 weeks, <6 hours of age)
- Supportive: glucose, ventilation if needed, seizure management
5. Documentation (Critical Duty)
- Admission note: birth history, weight, gestation, APGAR, vitals, examination findings, provisional diagnosis, plan
- Daily progress notes: SOAP format (Subjective, Objective, Assessment, Plan)
- Drug charts: Verify doses using weight-based dosing (always per kg)
- Fluid charts: Input/output, daily fluid requirements
- SNCU online register: In India, every SNCU logs data on the NHM SNCU online portal
- Discharge summary: Final diagnosis, treatment given, follow-up plan, immunization status
6. Common Drugs in SNCU (Know Your Doses)
| Drug | Dose | Indication |
|---|---|---|
| Ampicillin | 50 mg/kg/dose Q12h (early onset) | Neonatal sepsis |
| Gentamicin | 4-5 mg/kg/dose Q36-48h | Neonatal sepsis |
| Phenobarbitone | 20 mg/kg IV (loading) | Neonatal seizures |
| Vitamin K | 1 mg IM (term), 0.5 mg (preterm) | Hemorrhagic disease of newborn |
| Dextrose 10% | 2 mL/kg IV bolus | Symptomatic hypoglycemia |
| Caffeine citrate | 20 mg/kg loading, 5 mg/kg/day | Apnea of prematurity |
7. Infection Control in SNCU
- Hand hygiene is non-negotiable - wash before and after touching every baby
- The SNCU is a high-risk zone for nosocomial infections
- Wear gloves for all invasive procedures
- Clean incubators and warmers regularly
- Do NOT cross-contaminate between babies (use individual equipment)
8. Counselling Parents
- Explain diagnosis and treatment in simple language
- Demonstrate KMC to mothers
- Teach mothers to recognize danger signs before discharge
- Discuss breastfeeding support and expressed breast milk (EBM)
- Arrange follow-up after discharge (weight check, immunization, ROP screening if needed)
9. Discharge Criteria (Know When Babies are Ready)
- All acute problems resolved
- Baby accepting breast feeds or spoon feeds well
- Adequate weight gain for 3 consecutive days
- Baby weight >1.5 kg
- Mother confident to manage at home
- If jaundice with exchange transfusion: arrange BERA (hearing test)
- If weight <1800 g or <32 weeks: arrange ROP screening (Retinopathy of Prematurity)
Quick Summary: Intern's Daily SNCU Routine
- Morning: Check vitals sheet overnight, update fluid and feed charts
- Rounds: Assess each baby systematically, present to senior
- Procedures: Heel pricks, IV cannula, blood draws, NG feeds
- Documentation: Progress notes, drug chart updates
- Phototherapy: Check bilirubin results, adjust therapy
- New admissions: Admission note, initial stabilization
- Evening: Handover note, pending investigations, critical baby watch
Remember: In the SNCU, every gram of weight and every degree of temperature matters. When in doubt, escalate to your senior immediately - sick neonates can deteriorate very rapidly.
In pediatric ward new admission how to take vitals and write complaints and diagnosis before the round
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have everything needed for a comprehensive, practical answer. Here it is:
Pediatric Ward New Admission: Complete Intern's Guide
This is the full systematic approach for taking vitals, writing complaints, and preparing a diagnosis before the round.
STEP 1 - Take Vitals First (Before Anything Else)
How to Measure Each Vital Sign
Temperature
- Use digital thermometer; axillary route in children <5 years
- Normal: 36.5 - 37.5°C
-
37.5°C = fever; >38°C rectal = significant fever
- <36°C = hypothermia (common in neonates, malnourished, shocked)
Heart Rate (Pulse)
- In infants: feel brachial/femoral pulse; in older children: radial
- Count for full 60 seconds - do not estimate
- Note: rate, rhythm, volume (thready = shock)
| Age | Normal Heart Rate |
|---|---|
| <1 year | 100 - 160 bpm |
| 1-2 years | 90 - 150 bpm |
| 2-5 years | 80 - 140 bpm |
| 6-12 years | 70 - 120 bpm |
| >12 years | 60 - 100 bpm |
Tachycardia is the earliest sign of cardiovascular compromise. A thready pulse with tachycardia = shock until proven otherwise. Bradycardia in a sick child = impending cardiorespiratory failure.
Respiratory Rate
- Count chest movements for full 60 seconds (do not use stethoscope - observation only)
- Best done when child is calm or sleeping
| Age | Normal RR (breaths/min) |
|---|---|
| <1 year | 30 - 60 |
| 1-2 years | 24 - 40 |
| 2-5 years | 22 - 34 |
| 6-12 years | 18 - 30 |
| >12 years | 12 - 16 |
WHO definition of tachypnea (danger sign): >50/min in 2-11 months; >40/min in 1-5 years
Blood Pressure
- Use correct cuff size: cuff bladder should cover 2/3 of upper arm
- Too small a cuff = falsely HIGH reading; too large = falsely LOW reading
- Formula to estimate normal systolic BP:
- Children ≥1 year: (Age in years × 2) + 90 mmHg
- Minimum acceptable systolic BP (hypotension threshold):
- 0-28 days: 60 mmHg
- 1-12 months: 70 mmHg
- 1-10 years: 70 + (2 × age in years) mmHg
-
10 years: 90 mmHg
Remember: Children maintain BP until very late in shock (>30% blood loss). Hypotension is a late and ominous sign. Don't wait for it.
SpO2 (Pulse Oximetry)
- Normal: >95% in room air
- 90-94% = moderate hypoxia - give oxygen
- <90% = severe hypoxia - urgent
Weight
- Weigh every new admission - all drug doses are weight-based in pediatrics
- Use beam balance or electronic scale; remove clothes and nappy
- If unable to weigh: estimate - Weight (kg) = (Age in years + 4) × 2 (for 1-10 years)
AVPU / GCS (Neurological status)
- Quick assessment: Alert / Voice response / Pain response / Unresponsive
- Full GCS for older children with neurological complaints
STEP 2 - Write the Complaint
Write exactly what the parent/patient says in their own words, but frame it medically.
Format:
"[Name], [age], [gender], brought by [mother/father/caregiver] with complaints of:
- [Chief complaint] - since [duration]
- [Associated complaint] - since [duration]
- [Associated complaint] - since [duration]"*
Rules for Writing Complaints:
- List in order of importance or chronological order
- Include duration for each complaint
- Keep it brief - this is not the history, just the complaints
- Use lay terms that reflect what was reported, then translate
Common Examples:
Example 1 - Bronchiolitis / Pneumonia:
- Cough - 5 days
- Fever - 3 days
- Fast breathing - 1 day
- Poor feeding - 2 days
Example 2 - Gastroenteritis:
- Loose stools (6 episodes/day) - 3 days
- Vomiting - 2 days
- Decreased urine output - 1 day
- Fever - 2 days
Example 3 - Seizures:
- Abnormal body movements (generalized tonic-clonic) - 2 episodes today
- Fever - 1 day
- Post-ictal drowsiness - 30 minutes
STEP 3 - Write the History (for the Admission Note)
Structure the history under these headings:
A. History of Present Illness (HPI)
Tell the story chronologically:
- When did it start? What happened first?
- Progression: getting better / worse / same?
- Any treatment given before coming here?
- For each complaint, ask: onset, duration, severity, progression, aggravating/relieving factors, associated symptoms
B. Birth History (especially <2 years)
- Term or preterm? (gestational age)
- Mode of delivery (NVD / LSCS)
- Birth weight
- Any cry at birth? Any NICU/SNCU admission?
- Antenatal complications
C. Feeding History
- Exclusively breastfed? Formula? Complementary foods started?
- Current feeding pattern and appetite
- Any feeding difficulty?
D. Developmental History (especially <5 years)
- Milestones: social smile, neck holding, sitting, standing, walking, words, sentences
- Any regression?
E. Immunization History
- Up to date as per national schedule (BCG, OPV, IPV, Penta, PCV, MR, etc.)?
- Note the last vaccine given and date
F. Past Medical History
- Previous hospitalizations, operations, chronic illnesses
- Known allergies (especially drug allergies)
G. Family History
- Siblings' health; similar illness in family?
- Consanguinity (relevant for genetic/metabolic disorders)
H. Socio-economic / Environmental History
- Housing, water source, sanitation
- Exposure to TB contact, smoke, animals
STEP 4 - Physical Examination (Systematic)
General Examination (always first)
- Build & nutrition: well-nourished / moderately malnourished / severely malnourished (use MUAC, weight-for-height)
- Pallor: check conjunctiva, palms, nail beds
- Icterus: check sclera, skin
- Cyanosis: central (tongue, lips) vs peripheral (fingertips)
- Clubbing: grade I-IV
- Lymphadenopathy: location, size, tender/non-tender, matted
- Edema: pitting? location?
- Dehydration signs: sunken eyes, sunken fontanelle, dry mouth, skin turgor, capillary refill
Systemic Examination
After general, examine the system relevant to the complaint in detail, then briefly cover others:
- Respiratory: RR, chest shape, retractions (subcostal/intercostal/suprasternal), air entry, wheeze/crackles
- CVS: heart sounds, murmur, pulse character, CRT (normal <2 sec)
- Abdomen: distension, tenderness, organomegaly (liver 1-2 cm below RCM is normal in infants), bowel sounds
- CNS: GCS/AVPU, fontanelle (bulging = raised ICP; sunken = dehydration), tone, reflexes, meningeal signs
- ENT: throat (red/tonsils), ears (TM), nose
STEP 5 - Write the Provisional Diagnosis
Based on the history and examination, write:
Format:
Provisional Diagnosis: A [age] [gender] child with [key complaint] likely due to:
- [Primary diagnosis] - based on [key findings that support it]
- Rule out: [Differential 1]
- Rule out: [Differential 2]
Example 1:
Provisional Diagnosis: A 3-year-old male child presenting with fever and fast breathing likely has:
- Community-acquired pneumonia (right lower lobe) - based on fever, tachypnea (RR 58), subcostal retractions, decreased air entry and crepitations on right side
- Rule out: Bronchiolitis (age slightly older, no wheeze)
- Rule out: Pulmonary TB (no contact history, short duration)
Example 2:
Provisional Diagnosis: A 10-month-old female child with loose stools and vomiting likely has:
- Acute gastroenteritis with moderate dehydration - based on 6 loose watery stools/day, sunken eyes, reduced skin turgor, irritable, RR normal, HR 140
- Rule out: Intussusception (if blood in stool / colicky pain)
STEP 6 - Write the Initial Management Plan
Immediately write what needs to be done before the round:
- IV access: establish, send bloods (CBC, CRP, electrolytes, blood culture if sepsis suspected)
- Fluids: IV/oral rehydration plan (ORS for mild-moderate dehydration; Ringer's Lactate/Normal Saline IV for severe)
- Oxygen: if SpO2 <94%, start O2 via nasal prongs 1-2 L/min
- Temperature: paracetamol 15 mg/kg/dose if fever >38.5°C
- Empirical antibiotics: only if sepsis/pneumonia suspected - hold pending senior review
- Nothing by mouth (NPO): if surgical abdomen, altered consciousness, severe respiratory distress
- Monitoring: chart vitals every 4 hours (or more frequently if sick), record urine output
Quick Pre-Round Checklist
Before the consultant arrives, have ready for each new admission:
- Vitals recorded on chart (T, HR, RR, SpO2, BP, weight)
- Complaints written in order with duration
- History taken and documented
- General + systemic examination done
- Provisional diagnosis written
- IV access established (if needed)
- Baseline investigations sent (CBC, CRP, urine, blood culture, etc.)
- Drug chart started with accurate weight-based doses
- Fluid chart started (input/output)
- Previous records / referral letter reviewed
Sources: Rosen's Emergency Medicine, 10th ed.; The Harriet Lane Handbook, 23rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.