Hypercalcemia changes xray
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent images retrieved. Now I have everything needed for a comprehensive answer. Here is the full breakdown:
Hypercalcemia: X-Ray Changes
Hypercalcemia most commonly results from primary hyperparathyroidism or malignancy, and the radiological findings largely reflect the underlying cause and chronicity. The classic changes are best understood under the mnemonic "Stones, Bones, Abdominal Groans, Psychic Moans."
1. Skeletal Changes (Bones)
These are due to excessive PTH-driven bone resorption (osteoclast activation). Classic findings are now rare in developed countries due to early biochemical detection, seen in <5% of patients. They become apparent in severe/long-standing disease.
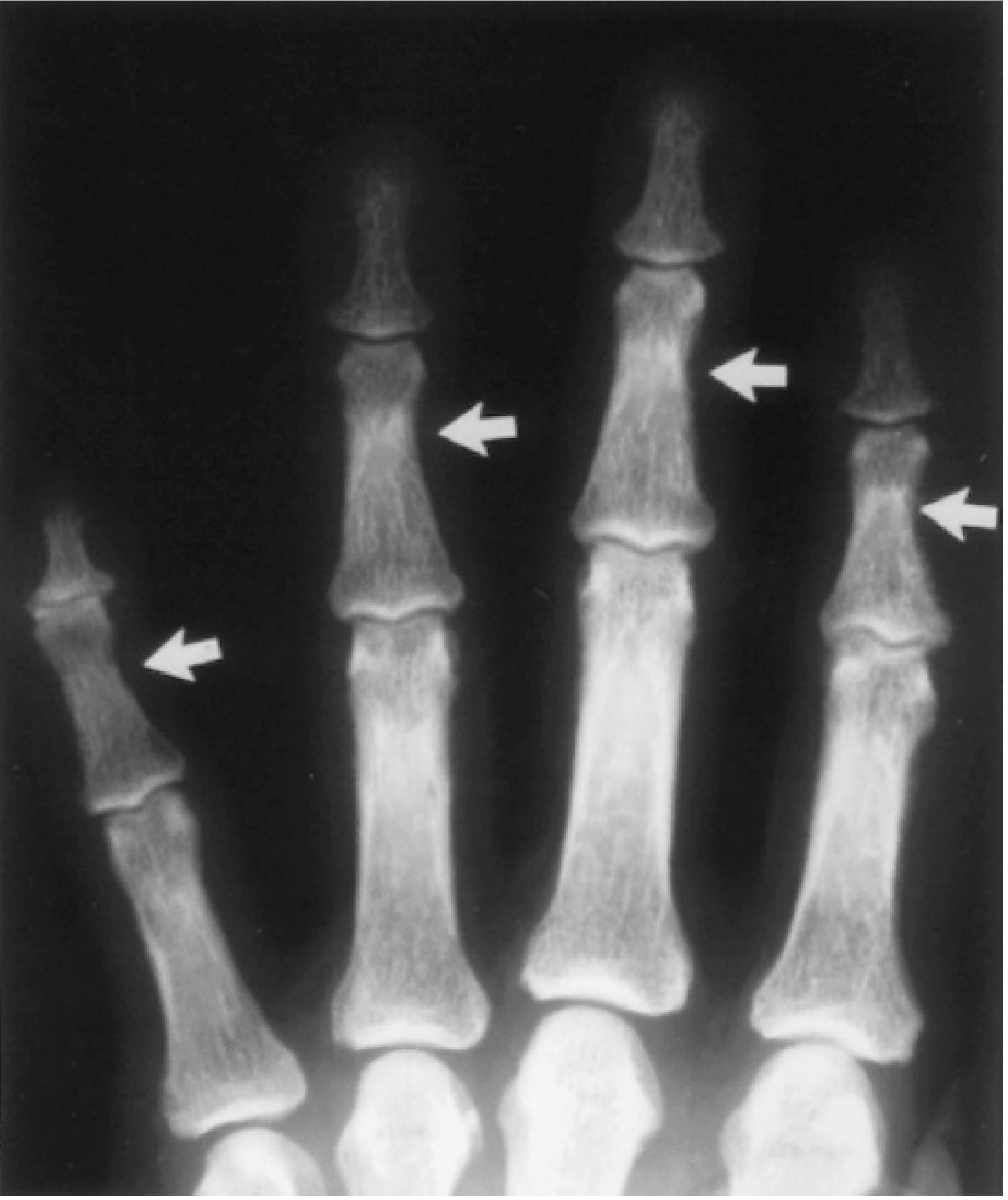
a. Subperiosteal Bone Resorption (most pathognomonic)
- Best seen on the radial aspect of the middle phalanx of the 2nd and 3rd fingers
- Appears as irregular, lacy erosion of the cortex on the radial border
- Also involves: lamina dura (loss around tooth roots on dental X-ray), distal clavicle tapering/resorption, and distal phalanges (acro-osteolysis/tufting)
b. "Salt-and-Pepper" Skull
- Diffuse granular demineralization of the skull vault
- Results from a mix of bone resorption and new bone formation
- Gives a mottled, stippled appearance on skull X-ray
c. Osteitis Fibrosa Cystica
- Most severe skeletal manifestation (rare today, seen in parathyroid carcinoma or very advanced disease)
- X-ray shows: bone cysts, brown tumors (well-defined lucent lesions in long bones/jaw from osteoclast proliferation and hemorrhage), and generalized demineralization
- Brown tumors appear as lytic lesions and can be mistaken for metastases
d. Distal Clavicle Resorption
- Tapering and erosion of the outer end of the clavicle
- Best seen on AP chest or shoulder X-ray
e. Generalized Osteopenia
- Diffuse loss of cortical bone density - occurs in ~25% of patients
- More prominent in cortical bone (distal forearm) than cancellous bone (spine)
2. Renal Changes (Stones)
a. Nephrocalcinosis
- Calcification within the renal parenchyma (medullary > cortical)
- Appears as bilateral dense calcification in renal shadows on plain abdominal X-ray


b. Nephrolithiasis
- Calcium oxalate or calcium phosphate stones (radio-opaque) visible on KUB/plain abdominal film
- Occurs in ~20% of patients with primary hyperparathyroidism
3. Soft Tissue Calcification
- Metastatic calcification in severe/chronic hypercalcemia: deposits in soft tissues, blood vessels, lungs, stomach wall, and myocardium
- Best visualized on chest X-ray (pulmonary calcification) or plain films of extremities
- Chondrocalcinosis (calcium pyrophosphate deposition in cartilage): seen in joints, particularly the knee
4. Other Notable X-Ray Features
| Finding | Location | Notes |
|---|---|---|
| Salt-and-pepper skull | Skull X-ray | Mottled granular appearance |
| Subperiosteal resorption | Radial aspect of middle phalanx | Most pathognomonic sign |
| Lamina dura loss | Dental X-ray | Loss of dense white line around tooth roots |
| Distal clavicle tapering | Shoulder/chest X-ray | Erosion of acromial end |
| Brown tumors | Long bones, jaw | Lytic lesions - rare |
| Nephrocalcinosis | KUB / abdominal X-ray | Bilateral renal calcification |
| Nephrolithiasis | KUB | Radio-opaque stones |
| Generalized osteopenia | Any skeletal film | Cortical > cancellous bone |
Clinical Context
These classic X-ray changes (especially osteitis fibrosa cystica) are now rarely seen in resource-rich settings because hypercalcemia is detected incidentally on routine biochemistry before bony disease develops. According to Goldman-Cecil Medicine, they are found in fewer than 5% of patients today. In low-resource settings or with parathyroid carcinoma, the full picture remains clinically relevant.
Sources: Goldman-Cecil Medicine; Mulholland & Greenfield's Surgery; Swanson's Family Medicine Review; Robbins & Kumar Pathologic Basis of Disease; Comprehensive Clinical Nephrology 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.