Merge these two ppt & make one out of it on topic mesenteric ischemia which is with simple background & use little bit tables & flowchart format & images taken from standard textbook & not just paragraphic type …
cd /home/daytona/workspace && python -m markitdown "/home/daytona/workspace/attachments/0f2ab5db-433b-4a7d-8b03-41b86e7ff2e2/mesenteric ischemia.pptx" 2>/dev/null | head -300
cd /home/daytona/workspace && python -m markitdown "/home/daytona/workspace/attachments/0f2ab5db-433b-4a7d-8b03-41b86e7ff2e2/mesenteric ischemia.pptx" 2>&1 | cat
cd /home/daytona/workspace && python3 -c " from pptx import Presentation import sys path1 = '/home/daytona/workspace/attachments/0f2ab5db-433b-4a7d-8b03-41b86e7ff2e2/mesenteric ischemia.pptx' prs = Presentation(path1) print(f'=== FILE 1: mesenteric ischemia.pptx - {len(prs.slides)} slides ===') for i, slide in enumerate(prs.slides): print(f'--- Slide {i+1} ---') for shape in slide.shapes: if shape.has_text_frame: for para in shape.text_frame.paragraphs: text = para.text.strip() if text: print(text) " 2>&1
which node && node --version && ls /home/daytona/skills/pptx/scripts/ 2>/dev/null || ls /home/daytona/skills/pptx/ 2>/dev/null
ls /home/daytona/skills/pptx/ && ls /home/daytona/skills/pptx/office/ 2>/dev/null
ls /home/daytona/skills/pptx/scripts/ && python3 /home/daytona/skills/pptx/scripts/thumbnail.py --help 2>&1 | head -20
ls /home/daytona/skills/pptx/scripts/office/ 2>/dev/null && ls /home/daytona/skills/shared/scripts/ 2>/dev/null
mkdir -p /home/daytona/workspace/mesenteric-ischemia && python3 /home/daytona/skills/pptx/scripts/office/unpack.py "/home/daytona/workspace/attachments/0f2ab5db-433b-4a7d-8b03-41b86e7ff2e2/mesenteric ischemia.pptx" /home/daytona/workspace/mesenteric-ischemia/unpacked1/ 2>&1 && echo "DONE"
cd /home/daytona/workspace/mesenteric-ischemia && unzip -o "/home/daytona/workspace/attachments/0f2ab5db-433b-4a7d-8b03-41b86e7ff2e2/mesenteric ischemia.pptx" -d unpacked1/ 2>&1 | tail -5 && echo "Done"
ls -la "/home/daytona/workspace/attachments/0f2ab5db-433b-4a7d-8b03-41b86e7ff2e2/" 2>&1
cp "/home/daytona/workspace/attachments/0f2ab5db-433b-4a7d-8b03-41b86e7ff2e2/mesenteric ischemia.pptx" /home/daytona/workspace/mesenteric-ischemia/ppt1.pptx && cp "/home/daytona/workspace/attachments/0f2ab5db-433b-4a7d-8b03-41b86e7ff2e2/Mesenteric_Ischemia_Surgery_v2.pptx" /home/daytona/workspace/mesenteric-ischemia/ppt2.pptx && echo "Copied"
cd /home/daytona/workspace/mesenteric-ischemia && unzip -o ppt1.pptx -d unpacked1/ 2>&1 | tail -3 && echo "DONE1"
timeout 10 python3 -c " import zipfile path = '/home/daytona/workspace/mesenteric-ischemia/ppt1.pptx' with zipfile.ZipFile(path, 'r') as z: names = z.namelist() print('Files:', len(names)) slides = [n for n in names if 'ppt/slides/slide' in n and '.xml' in n and 'rels' not in n] print('Slides:', sorted(slides)) " 2>&1
timeout 30 python3 -c " import zipfile, re def extract_text(path): with zipfile.ZipFile(path, 'r') as z: names = z.namelist() slides = sorted([n for n in names if 'ppt/slides/slide' in n and n.endswith('.xml') and 'rels' not in n], key=lambda x: int(re.search(r'slide(\d+)', x).group(1))) results = [] for sname in slides: content = z.read(sname).decode('utf-8', errors='ignore') # Extract all text runs texts = re.findall(r'<a:t[^>]*>(.*?)</a:t>', content, re.DOTALL) slide_text = ' | '.join([t.strip() for t in texts if t.strip()]) results.append((sname, slide_text[:300])) return results print('=== PPT1 ===') for s, t in extract_text('/home/daytona/workspace/mesenteric-ischemia/ppt1.pptx'): print(f'{s}: {t}') " 2>&1
timeout 30 python3 -c " import zipfile, re def extract_text(path): with zipfile.ZipFile(path, 'r') as z: names = z.namelist() slides = sorted([n for n in names if 'ppt/slides/slide' in n and n.endswith('.xml') and 'rels' not in n], key=lambda x: int(re.search(r'slide(\d+)', x).group(1))) results = [] for sname in slides: content = z.read(sname).decode('utf-8', errors='ignore') texts = re.findall(r'<a:t[^>]*>(.*?)</a:t>', content, re.DOTALL) slide_text = ' | '.join([t.strip() for t in texts if t.strip()]) results.append((sname, slide_text[:400])) return results print('=== PPT2 ===') for s, t in extract_text('/home/daytona/workspace/mesenteric-ischemia/ppt2.pptx'): print(f'{s}: {t}') " 2>&1
~/mesenteric-ischemia/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Mesenteric Ischemia – Comprehensive Surgical Review";
pres.author = "Surgical Education";
// ─────────────────────────────────────────────
// COLOUR PALETTE (clean, clinical, white background)
// ─────────────────────────────────────────────
const C = {
navy: "1A3557", // dark navy – title bars, headers
teal: "1A7A8A", // teal accent – section banners
red: "C0392B", // danger / warning callouts
orange: "E67E22", // amber highlights
green: "1E8449", // good outcomes
lightBg: "F0F4F8", // slide background (very light blue-grey)
white: "FFFFFF",
darkText: "1A2332",
midText: "2C3E50",
subText: "4A5568",
tableHdr: "1A3557",
tableRow: "EAF0F6",
tableAlt: "FFFFFF",
border: "B0BEC5",
};
// ─────────────────────────────────────────────
// HELPERS
// ─────────────────────────────────────────────
function addSlide(bg) {
const sl = pres.addSlide();
sl.background = { color: bg || C.lightBg };
return sl;
}
function sectionBanner(slide, label) {
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.45, fill: { color: C.teal }, line: { color: C.teal } });
slide.addText(label.toUpperCase(), {
x: 0.18, y: 0.04, w: 9.6, h: 0.38,
fontSize: 9, bold: true, color: C.white, charSpacing: 2
});
}
function slideTitle(slide, title, sub) {
// navy bar at top
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0.45, w: 10, h: 0.72, fill: { color: C.navy }, line: { color: C.navy } });
slide.addText(title, {
x: 0.25, y: 0.47, w: 9.5, h: 0.66,
fontSize: 22, bold: true, color: C.white, valign: "middle"
});
if (sub) {
slide.addText(sub, {
x: 0.25, y: 1.22, w: 9.5, h: 0.32,
fontSize: 11, color: C.teal, italic: true
});
}
}
function bullet(text, indent, bold) {
return {
text,
options: {
bullet: { indent: indent || 10 },
fontSize: 13,
color: bold ? C.navy : C.darkText,
bold: !!bold,
breakLine: true,
paraSpaceAfter: 3,
}
};
}
function divider(slide, y) {
slide.addShape(pres.ShapeType.line, {
x: 0.3, y, w: 9.4, h: 0,
line: { color: C.border, width: 0.8 }
});
}
// ─────────────────────────────────────────────
// 1. TITLE SLIDE
// ─────────────────────────────────────────────
{
const sl = addSlide(C.navy);
// decorative top stripe
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.18, fill: { color: C.teal }, line: { color: C.teal } });
// large white title
sl.addText("MESENTERIC ISCHEMIA", {
x: 0.6, y: 0.9, w: 8.8, h: 1.1,
fontSize: 42, bold: true, color: C.white, align: "center", charSpacing: 3
});
sl.addShape(pres.ShapeType.rect, { x: 2.5, y: 2.1, w: 5, h: 0.07, fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("A COMPREHENSIVE SURGICAL REVIEW", {
x: 0.5, y: 2.25, w: 9, h: 0.55,
fontSize: 17, color: C.teal, align: "center", charSpacing: 1.5
});
sl.addText([
{ text: "Presenter: Dr. Jeet Vaghasiya (R3SU1) | ", options: { fontSize: 12, color: "A8C0D6" } },
{ text: "Chairperson: Dr. Ketan Mehta (MS), Dr. Girish Parmar (MS)", options: { fontSize: 12, color: "A8C0D6" } }
], { x: 0.5, y: 3.1, w: 9, h: 0.4, align: "center" });
sl.addText("Based on: Schwartz's Principles of Surgery 11e · Sabiston Textbook of Surgery · Current Surgical Therapy 14e", {
x: 0.5, y: 3.65, w: 9, h: 0.4,
fontSize: 9.5, color: "7A9BBF", align: "center", italic: true
});
sl.addShape(pres.ShapeType.rect, { x: 0, y: 5.2, w: 10, h: 0.42, fill: { color: "122540" }, line: { color: "122540" } });
sl.addText("General Surgery · 2026", {
x: 0.5, y: 5.22, w: 9, h: 0.36,
fontSize: 10, color: "7A9BBF", align: "center"
});
}
// ─────────────────────────────────────────────
// 2. LECTURE OUTLINE
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Overview");
slideTitle(sl, "Lecture Outline", null);
const topics = [
"1. Introduction & Historical Perspective",
"2. Epidemiology & Mortality Data",
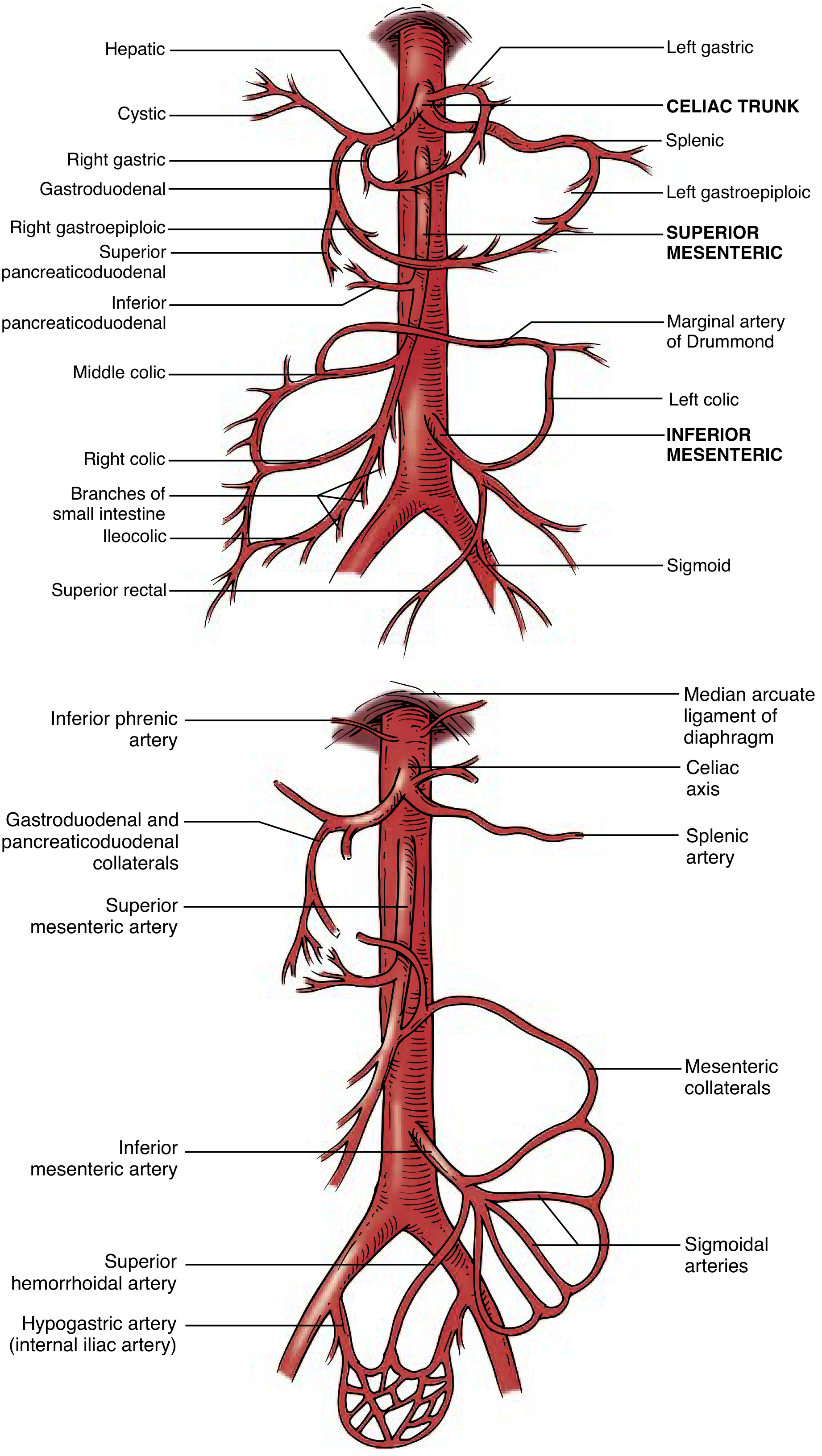
"3. Vascular Anatomy — SMA & Collaterals",
"4. Classification of Mesenteric Ischemia",
"5. Pathophysiology — Ischemia Timeline",
"6. Embolic vs. Thrombotic vs. NOMI vs. MVT",
"7. Clinical Presentation & Differential Diagnosis",
"8. Diagnostic Investigations (Labs + CTA)",
"9. Surgical & Endovascular Management of AMI",
"10. Chronic Mesenteric Ischemia — Workup & Revascularization",
"11. Special Scenarios, Complications & Outcomes",
];
const col1 = topics.slice(0, 6);
const col2 = topics.slice(6);
const mkItems = (arr) => arr.map(t => ({ text: t, options: { fontSize: 13, color: C.darkText, bullet: { indent: 8 }, breakLine: true, paraSpaceAfter: 5 } }));
sl.addText(mkItems(col1), { x: 0.3, y: 1.58, w: 4.6, h: 3.8 });
sl.addShape(pres.ShapeType.line, { x: 5.0, y: 1.6, w: 0, h: 3.7, line: { color: C.border, width: 0.8 } });
sl.addText(mkItems(col2), { x: 5.15, y: 1.58, w: 4.6, h: 3.8 });
}
// ─────────────────────────────────────────────
// 3. HISTORICAL MILESTONES TABLE
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 1 — Introduction & Epidemiology");
slideTitle(sl, "Historical Perspective & Epidemiology");
// Table
const rows = [
[{ text: "Year", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Milestone", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } }],
["1869", "First description of mesenteric ischemia — Chienne"],
["1895", "First intestinal resection & reanastomosis — Elliot"],
["1951", "First SMA embolectomy — Klass"],
["1957", "First successful embolectomy without bowel resection — Shaw & Maynard"],
["1980s", "Endovascular treatment of mesenteric disease introduced"],
["2000s+", "Endovascular-first strategies; improved CT imaging — paradigm shift"],
];
sl.addTable(rows, {
x: 0.3, y: 1.6, w: 9.4, h: 3.4,
colW: [1.2, 8.2],
border: { type: "solid", color: C.border, pt: 0.5 },
fill: { color: C.tableAlt },
rowH: 0.44,
fontFace: "Calibri",
fontSize: 12,
color: C.darkText,
align: "left",
valign: "middle",
});
// Epi callout box bottom
sl.addShape(pres.ShapeType.rect, { x: 0.3, y: 5.05, w: 9.4, h: 0.45,
fill: { color: "EBF5FB" }, line: { color: C.teal, width: 1 } });
sl.addText("Epidemiology: < 1/100,000 admissions · Median age 74 yrs · Incidence doubles per 5-yr interval >70 · 3× higher in females · Overall AMI mortality ~17–21%", {
x: 0.4, y: 5.07, w: 9.2, h: 0.4,
fontSize: 10.5, color: C.teal, italic: false
});
}
// ─────────────────────────────────────────────
// 4. CLASSIFICATION TABLE
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 3 — Classification");
slideTitle(sl, "Classification of Mesenteric Ischemia");
const rows = [
[
{ text: "Type", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "% of AMI", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Mechanism", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Key Feature", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
],
[
{ text: "Arterial Embolism", options: { bold: true } },
"40–50%",
"Cardiac source → SMA lodging",
"Abrupt onset; proximal jejunum/R colon spared"
],
[
{ text: "Arterial Thrombosis", options: { bold: true } },
"20–35%",
"Atherosclerotic occlusion at SMA origin",
"History of CMI symptoms; diffuse ischemia"
],
[
{ text: "NOMI", options: { bold: true } },
"~20%",
"Mesenteric vasoconstriction; low-flow state",
"ICU patients; vasopressors; no occlusion on CTA"
],
[
{ text: "Mesenteric Venous Thrombosis", options: { bold: true } },
"5–15%",
"Portal/SMV thrombosis → venous hypertension",
"Subacute; anticoagulation; best prognosis"
],
[
{ text: "Chronic MI (CMI)", options: { bold: true } },
"—",
"Progressive atherosclerosis ≥2 visceral vessels",
"Food fear; weight loss; postprandial pain"
],
];
sl.addTable(rows, {
x: 0.2, y: 1.58, w: 9.6, h: 3.8,
colW: [2.1, 1.0, 3.4, 3.1],
border: { type: "solid", color: C.border, pt: 0.5 },
fill: { color: C.tableAlt },
rowH: 0.6,
fontFace: "Calibri",
fontSize: 11.5,
color: C.darkText,
align: "left",
valign: "middle",
});
}
// ─────────────────────────────────────────────
// 5. VASCULAR ANATOMY
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 2 — Vascular Anatomy");
slideTitle(sl, "Mesenteric Vascular Anatomy & Collaterals");
// Left panel – anatomy text
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 1.58, w: 4.55, h: 0.32,
fill: { color: C.navy }, line: { color: C.navy } });
sl.addText("Three Major Mesenteric Arteries", {
x: 0.3, y: 1.59, w: 4.45, h: 0.3,
fontSize: 11, bold: true, color: C.white
});
sl.addText([
bullet("Celiac Artery — foregut (stomach → proximal duodenum, liver, spleen)", 10),
bullet("Superior Mesenteric Artery (SMA) — midgut (distal duodenum → 2/3 transverse colon)", 10),
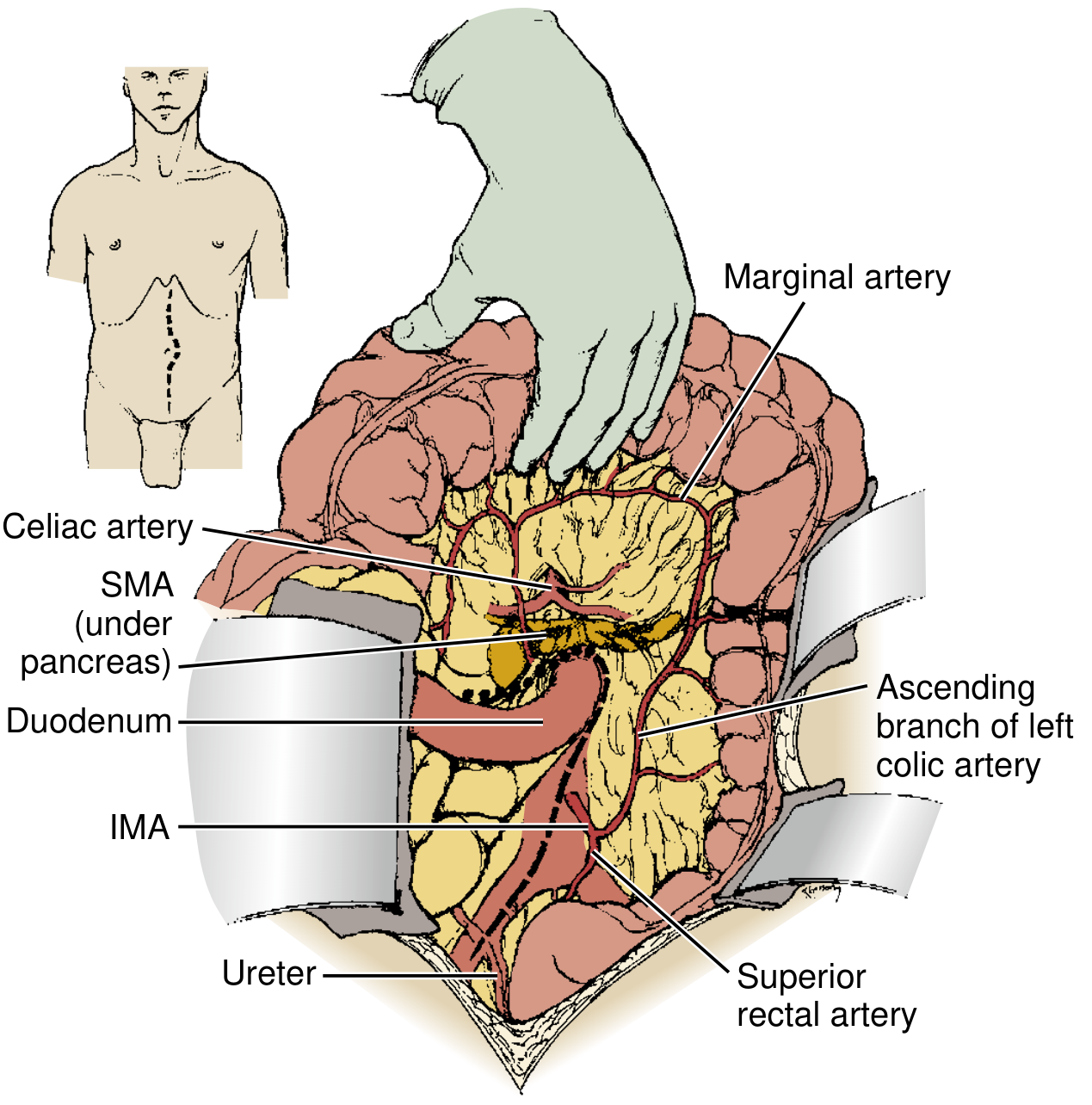
bullet("Inferior Mesenteric Artery (IMA) — hindgut (splenic flexure → rectum)", 10),
bullet("SMA: 2nd branch of aorta; oblique angle → thromboemboli preferentially lodge here", 10),
bullet("50% of emboli settle distal to middle colic a. origin", 10),
], { x: 0.3, y: 1.92, w: 4.45, h: 2.0 });
divider(sl, 3.95);
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 4.0, w: 4.55, h: 0.32,
fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("Key Collateral Pathways", {
x: 0.3, y: 4.01, w: 4.45, h: 0.3,
fontSize: 11, bold: true, color: C.white
});
sl.addText([
bullet("Celiac ↔ SMA: Pancreaticoduodenal arcade", 10),
bullet("SMA ↔ IMA: Marginal artery of Drummond", 10),
bullet("SMA ↔ IMA: Arc of Riolan (meandering mesenteric a.)", 10),
bullet("IMA ↔ Internal iliac: Hemorrhoidal arteries", 10),
], { x: 0.3, y: 4.34, w: 4.45, h: 1.2 });
// Right panel – anatomy diagram (shapes)
sl.addShape(pres.ShapeType.rect, { x: 5.05, y: 1.58, w: 4.7, h: 4.0,
fill: { color: "EBF5FB" }, line: { color: C.border } });
sl.addText("MESENTERIC ARTERIAL TREE", {
x: 5.1, y: 1.65, w: 4.6, h: 0.3,
fontSize: 10, bold: true, color: C.navy, align: "center"
});
// Aorta (vertical bar)
sl.addShape(pres.ShapeType.rect, { x: 7.3, y: 2.1, w: 0.18, h: 3.1,
fill: { color: C.navy }, line: { color: C.navy } });
sl.addText("AORTA", { x: 7.52, y: 3.4, w: 0.8, h: 0.25, fontSize: 8, bold: true, color: C.navy });
// Celiac
sl.addShape(pres.ShapeType.line, { x: 6.25, y: 2.25, w: 1.05, h: 0, line: { color: C.teal, width: 2 } });
sl.addShape(pres.ShapeType.ellipse, { x: 5.55, y: 2.12, w: 0.72, h: 0.28, fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("Celiac", { x: 5.55, y: 2.14, w: 0.72, h: 0.24, fontSize: 8, bold: true, color: C.white, align: "center" });
// SMA
sl.addShape(pres.ShapeType.line, { x: 6.25, y: 3.0, w: 1.05, h: 0, line: { color: C.orange, width: 2.5 } });
sl.addShape(pres.ShapeType.ellipse, { x: 5.45, y: 2.87, w: 0.85, h: 0.28, fill: { color: C.orange }, line: { color: C.orange } });
sl.addText("SMA", { x: 5.45, y: 2.89, w: 0.85, h: 0.24, fontSize: 9, bold: true, color: C.white, align: "center" });
// IMA
sl.addShape(pres.ShapeType.line, { x: 6.25, y: 3.75, w: 1.05, h: 0, line: { color: C.green, width: 2 } });
sl.addShape(pres.ShapeType.ellipse, { x: 5.55, y: 3.62, w: 0.72, h: 0.28, fill: { color: C.green }, line: { color: C.green } });
sl.addText("IMA", { x: 5.55, y: 3.64, w: 0.72, h: 0.24, fontSize: 8, bold: true, color: C.white, align: "center" });
// Collateral arrows
sl.addShape(pres.ShapeType.line, { x: 5.9, y: 2.72, w: 0, h: 0.2, line: { color: C.red, width: 1.5 } });
sl.addText("↕ Collateral", { x: 5.75, y: 2.9, w: 1.1, h: 0.2, fontSize: 7.5, color: C.red, italic: true });
sl.addShape(pres.ShapeType.line, { x: 5.9, y: 3.46, w: 0, h: 0.2, line: { color: C.red, width: 1.5 } });
sl.addText("↕ Collateral", { x: 5.75, y: 3.65, w: 1.1, h: 0.2, fontSize: 7.5, color: C.red, italic: true });
sl.addText("Clinical pearl: Ischemia typically requires ≥2 of 3 vessels to be compromised due to abundant collaterals", {
x: 5.1, y: 4.8, w: 4.55, h: 0.55,
fontSize: 9.5, color: C.red, italic: true, wrap: true
});
}
// ─────────────────────────────────────────────
// 6. PATHOPHYSIOLOGY TIMELINE
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 4 — Pathophysiology");
slideTitle(sl, "Pathophysiology — Ischemia Timeline", '"Time is Bowel — Minutes Matter"');
// Timeline flowchart using shapes
const boxes = [
{ label: "0 – 3 hrs", desc: "Mucosal sloughing\nBacterial translocation\nVillous tip necrosis", color: C.orange },
{ label: "3 – 6 hrs", desc: "Full-thickness\nischemia begins\nWall oedema, haemorrhage", color: "E74C3C" },
{ label: "> 6 hrs", desc: "FULL-THICKNESS\nINFARCTION\nIrreversible necrosis", color: C.red },
{ label: "Late / Untreated", desc: "Peritonitis\nSeptic shock\nMulti-organ failure\nDEATH", color: "7B241C" },
];
boxes.forEach((b, i) => {
const x = 0.35 + i * 2.38;
// Box
sl.addShape(pres.ShapeType.rect, { x, y: 1.72, w: 2.1, h: 1.6,
fill: { color: b.color }, line: { color: b.color } });
sl.addText(b.label, { x, y: 1.74, w: 2.1, h: 0.36, fontSize: 12, bold: true, color: C.white, align: "center" });
sl.addText(b.desc, { x, y: 2.12, w: 2.1, h: 1.16, fontSize: 10.5, color: C.white, align: "center", valign: "middle", wrap: true });
// Arrow
if (i < 3) {
sl.addShape(pres.ShapeType.line, { x: x + 2.1, y: 2.52, w: 0.28, h: 0, line: { color: C.midText, width: 2 } });
sl.addText("▶", { x: x + 2.14, y: 2.43, w: 0.2, h: 0.2, fontSize: 10, color: C.midText });
}
});
// Cascade box
sl.addShape(pres.ShapeType.rect, { x: 0.3, y: 3.5, w: 9.4, h: 0.32,
fill: { color: C.navy }, line: { color: C.navy } });
sl.addText("PATHOPHYSIOLOGICAL CASCADE", {
x: 0.35, y: 3.51, w: 9.3, h: 0.3,
fontSize: 11, bold: true, color: C.white, charSpacing: 1.5
});
sl.addText([
{ text: "Reduced intestinal blood flow → ", options: { fontSize: 12, color: C.darkText } },
{ text: "Mucosal hypoxia → ", options: { fontSize: 12, color: C.orange } },
{ text: "Villous tip necrosis → ", options: { fontSize: 12, color: "E74C3C" } },
{ text: "Barrier disruption → ", options: { fontSize: 12, color: C.red } },
{ text: "Bacterial translocation → ", options: { fontSize: 12, color: "7B241C" } },
{ text: "Cytokine release → MODS", options: { fontSize: 12, bold: true, color: "7B241C" } },
], { x: 0.3, y: 3.85, w: 9.4, h: 0.45, wrap: true });
// Reperfusion injury box
sl.addShape(pres.ShapeType.rect, { x: 0.3, y: 4.38, w: 9.4, h: 0.95,
fill: { color: "FDFEFE" }, line: { color: C.orange, width: 1.5 } });
sl.addText([
{ text: "⚠ Reperfusion Injury: ", options: { bold: true, fontSize: 12, color: C.orange } },
{ text: "Restoration of blood flow → xanthine oxidase activation → superoxide radicals → lipid peroxidation → endothelial damage. ", options: { fontSize: 11.5, color: C.darkText } },
{ text: "Injury can EXCEED the original ischaemic insult.", options: { bold: true, fontSize: 11.5, color: C.red } },
], { x: 0.45, y: 4.43, w: 9.1, h: 0.8, wrap: true });
}
// ─────────────────────────────────────────────
// 7. EMBOLIC vs THROMBOTIC TABLE
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 4 — Pathophysiology");
slideTitle(sl, "Embolic vs. Thrombotic AMI — Key Differences");
const rows = [
[
{ text: "Feature", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Arterial EMBOLISM", options: { bold: true, color: C.white, fill: { color: "1A6080" } } },
{ text: "Arterial THROMBOSIS", options: { bold: true, color: C.white, fill: { color: "7B3A10" } } },
],
["% of AMI", "40–50%", "20–35%"],
["Source", "Cardiac (AF, LV thrombus, valvular)", "Atherosclerotic plaque at SMA origin"],
["Onset", "ABRUPT — no collateral protection", "Acute on chronic (gradual collaterals present)"],
["Location of lodging", "50% distal to middle colic a.; 15% at SMA origin", "SMA origin / proximal CA; pre-existing stenosis"],
["Bowel at risk", "Mid-jejunum → ascending colon; proximal jejunum SPARED", "Near-total small bowel (including proximal jejunum)"],
["Prior symptoms", "Usually none — sudden event", "Often history of post-prandial pain, weight loss"],
["Associated cardiac Dx", "95% have cardiac disease; 68% simultaneous emboli elsewhere", "Generalised PVD, renal artery disease, prior vascular Sx"],
["Operative approach", "SMA embolectomy (transverse arteriotomy)", "Bypass (antegrade / retrograde) or endarterectomy"],
];
sl.addTable(rows, {
x: 0.2, y: 1.6, w: 9.6, h: 3.9,
colW: [2.2, 3.7, 3.7],
border: { type: "solid", color: C.border, pt: 0.5 },
fill: { color: C.tableAlt },
rowH: 0.43,
fontFace: "Calibri",
fontSize: 10.8,
color: C.darkText,
align: "left",
valign: "middle",
});
}
// ─────────────────────────────────────────────
// 8. NOMI + MVT TABLE
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 4 — Pathophysiology");
slideTitle(sl, "NOMI & Mesenteric Venous Thrombosis");
// NOMI left
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 1.6, w: 4.6, h: 0.35,
fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("NOMI — Non-Occlusive Mesenteric Ischemia (~20%)", {
x: 0.3, y: 1.61, w: 4.5, h: 0.32,
fontSize: 10.5, bold: true, color: C.white
});
sl.addText([
bullet("Mechanism: Mesenteric vasoconstriction + intestinal hypoxaemia + reperfusion injury", 8),
bullet("Low-flow state: body prioritises cardiac/cerebral perfusion at expense of gut", 8),
bullet("Triggers: Cardiogenic shock, hypovolaemia, vasopressors, digitalis toxicity, dialysis, post-cardiac surgery, severe sepsis", 8),
bullet("CTA: No occlusion — 'pruning' of mesenteric vessels, vasospasm pattern", 8),
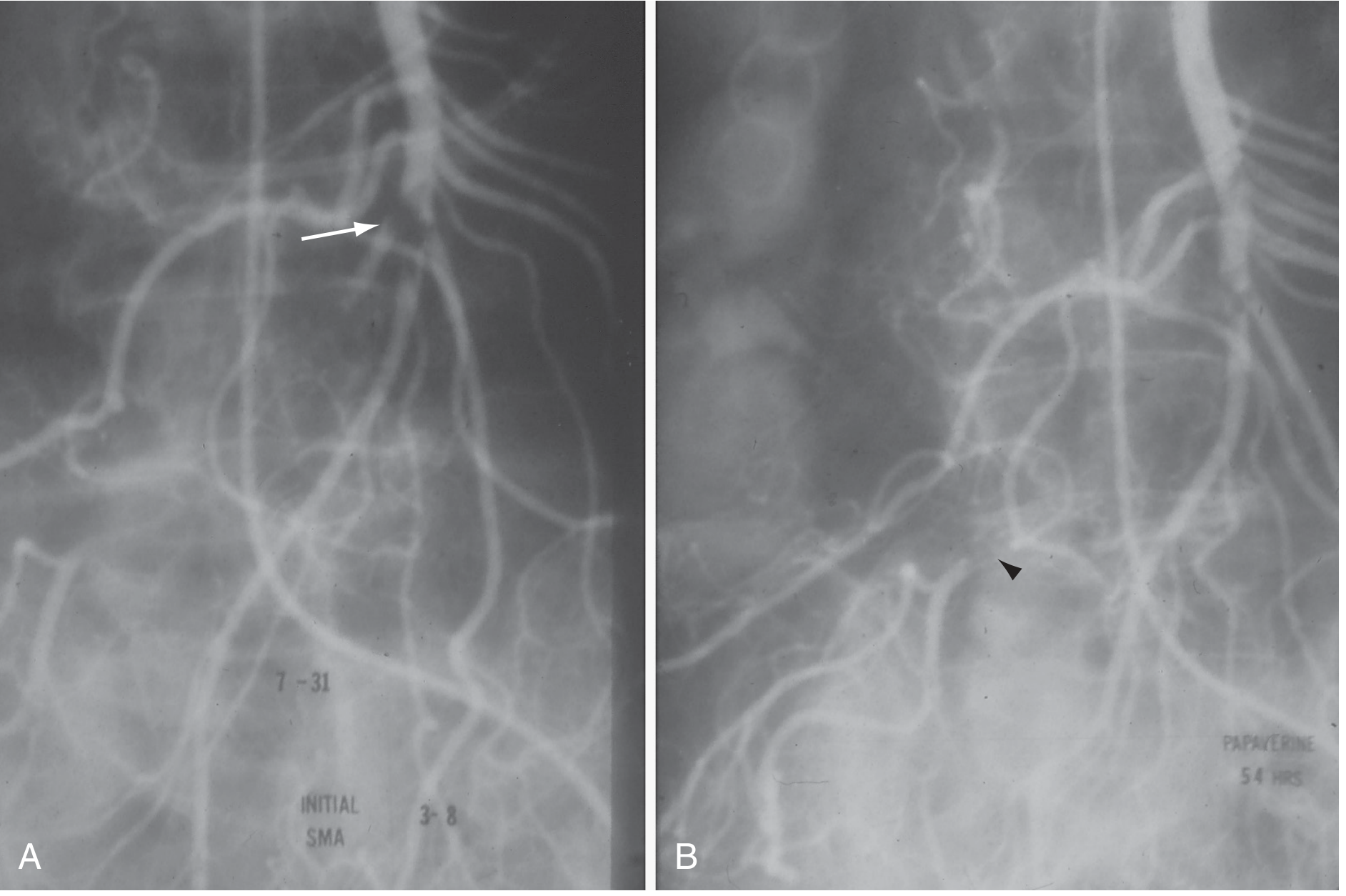
bullet("Treatment: Treat underlying cause + intra-arterial papaverine/vasodilators", 8),
bullet("Surgery only if peritonitis or bowel necrosis", 8),
], { x: 0.3, y: 1.98, w: 4.5, h: 3.45 });
// MVT right
sl.addShape(pres.ShapeType.rect, { x: 5.15, y: 1.6, w: 4.6, h: 0.35,
fill: { color: C.navy }, line: { color: C.navy } });
sl.addText("Mesenteric Venous Thrombosis (5–15%)", {
x: 5.2, y: 1.61, w: 4.5, h: 0.32,
fontSize: 10.5, bold: true, color: C.white
});
sl.addText([
bullet("Mechanism: Portal/SMV thrombosis → venous hypertension → bowel wall oedema & ischaemia", 8),
bullet("Risk factors: Hypercoagulable state (Factor V Leiden, protein C/S deficiency, JAK2), portal HTN, malignancy, OCP, abdominal sepsis", 8),
bullet("Presentation: Subacute (days–weeks) abdominal pain; often less dramatic than arterial AMI", 8),
bullet("CTA (venous phase): SMV/portal thrombus; bowel wall thickening; mesenteric fat stranding", 8),
bullet("Treatment: ANTICOAGULATION (heparin → warfarin/DOAC) — cornerstone", 8),
bullet("Surgery: Only for frank bowel necrosis; best overall prognosis of all AMI types", 8),
], { x: 5.2, y: 1.98, w: 4.5, h: 3.45 });
sl.addShape(pres.ShapeType.line, { x: 4.97, y: 1.6, w: 0, h: 3.8, line: { color: C.border, width: 0.8 } });
}
// ─────────────────────────────────────────────
// 9. CLINICAL PRESENTATION
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 5 — Clinical Presentation");
slideTitle(sl, "Clinical Presentation", "The diagnosis is clinical first, imaging second");
// AMI box
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 1.6, w: 4.6, h: 0.35,
fill: { color: C.red }, line: { color: C.red } });
sl.addText("ACUTE Mesenteric Ischemia — HALLMARKS", {
x: 0.3, y: 1.61, w: 4.5, h: 0.32,
fontSize: 10.5, bold: true, color: C.white
});
sl.addText([
{ text: "⚠ Pain OUT OF PROPORTION to physical exam — THE key diagnostic clue\n", options: { bold: true, fontSize: 13, color: C.red, breakLine: true } },
bullet("Sudden-onset severe periumbilical / mid-abdominal pain", 8),
bullet("Colicky character early; constant/severe when necrosis develops", 8),
bullet("Nausea, vomiting, diarrhoea (often bloody)", 8),
bullet("Early: physical exam surprisingly NORMAL", 8),
bullet("Late: peritonitis, rigidity, haemodynamic collapse", 8),
bullet("Risk factors: AF, recent MI, valvular disease, PVD", 8),
], { x: 0.3, y: 1.98, w: 4.5, h: 3.42 });
sl.addShape(pres.ShapeType.line, { x: 4.97, y: 1.6, w: 0, h: 3.85, line: { color: C.border, width: 0.8 } });
// CMI box
sl.addShape(pres.ShapeType.rect, { x: 5.15, y: 1.6, w: 4.6, h: 0.35,
fill: { color: C.navy }, line: { color: C.navy } });
sl.addText("CHRONIC Mesenteric Ischemia — Classic Triad", {
x: 5.2, y: 1.61, w: 4.5, h: 0.32,
fontSize: 10.5, bold: true, color: C.white
});
sl.addText([
bullet("Postprandial abdominal pain — 15–30 min after eating ('intestinal angina')", 8),
bullet("FOOD FEAR — patient voluntarily restricts eating to avoid pain", 8),
bullet("Progressive significant weight loss", 8),
bullet("Often misdiagnosed as malignancy (weight loss misleads clinicians)", 8),
bullet("3:1 female-to-male ratio", 8),
{ text: "\nMVT: ", options: { bold: true, fontSize: 12, color: C.teal, breakLine: false } },
{ text: "Subacute diffuse abdominal pain (days–weeks); less dramatic onset; may present with GI bleeding", options: { fontSize: 11.5, color: C.darkText, breakLine: true } },
], { x: 5.2, y: 1.98, w: 4.5, h: 3.42 });
}
// ─────────────────────────────────────────────
// 10. DIFFERENTIAL DIAGNOSIS TABLE
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 5 — Clinical Presentation");
slideTitle(sl, "Differential Diagnosis — Acute Severe Abdominal Pain");
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 1.6, w: 9.5, h: 0.32,
fill: { color: C.red }, line: { color: C.red } });
sl.addText("In any elderly patient with sudden severe abdominal pain + AF or vascular disease: AMI must be ACTIVELY EXCLUDED", {
x: 0.3, y: 1.62, w: 9.4, h: 0.28,
fontSize: 10.5, bold: true, color: C.white
});
const rows = [
[
{ text: "Surgical Emergencies", options: { bold: true, color: C.white, fill: { color: "1A3557" } } },
{ text: "GI / Medical Causes", options: { bold: true, color: C.white, fill: { color: "1A7A8A" } } },
{ text: "Vascular Emergencies", options: { bold: true, color: C.white, fill: { color: "922B21" } } },
],
["Perforated peptic ulcer", "Acute pancreatitis", "Ruptured AAA"],
["Bowel obstruction / volvulus", "Severe gastroenteritis", "Aortic dissection"],
["Acute appendicitis", "IBD exacerbation", "Ischaemic colitis"],
["Acute cholecystitis / cholangitis", "Renal colic / ureteral stone", "Spontaneous SMA dissection"],
["Sigmoid volvulus", "Inferior MI (referred pain)", "Median arcuate ligament syndrome"],
];
sl.addTable(rows, {
x: 0.25, y: 1.97, w: 9.5, h: 3.45,
colW: [3.16, 3.16, 3.18],
border: { type: "solid", color: C.border, pt: 0.5 },
fill: { color: C.tableAlt },
rowH: 0.55,
fontFace: "Calibri",
fontSize: 12,
color: C.darkText,
align: "center",
valign: "middle",
});
}
// ─────────────────────────────────────────────
// 11. LABORATORY INVESTIGATIONS TABLE
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 6 — Investigations");
slideTitle(sl, "Laboratory Investigations", "Adjuncts only — no single test confirms or excludes AMI");
const rows = [
[
{ text: "Investigation", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Finding in AMI", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Clinical Significance", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
],
["WBC count", "> 15,000 with neutrophilic left shift", "Suggests ischaemia/infarction; non-specific"],
["Serum Lactate", "Elevated (may be NORMAL early!)", "Normal lactate CANNOT exclude AMI — poor NPV"],
["Metabolic panel / ABG", "Metabolic acidosis, raised anion gap", "Late finding; suggests advanced ischaemia"],
["Amylase / Lipase", "Elevated (40–50% of cases)", "Non-specific; also raised in pancreatitis"],
["Serum phosphate", "Elevated > 1.5 mmol/L (inorganic phosphate)", "Raised with bowel necrosis; useful adjunct"],
["D-dimer", "Often elevated", "High sensitivity, very low specificity"],
["LDH / CK", "Elevated with muscle ischaemia", "Supports ischaemic necrosis; non-specific"],
["ABG", "pH < 7.35, base excess < -4", "Metabolic acidosis = advanced / widespread ischaemia"],
];
sl.addTable(rows, {
x: 0.2, y: 1.6, w: 9.6, h: 3.9,
colW: [2.0, 3.6, 4.0],
border: { type: "solid", color: C.border, pt: 0.5 },
fill: { color: C.tableAlt },
rowH: 0.42,
fontFace: "Calibri",
fontSize: 11,
color: C.darkText,
align: "left",
valign: "middle",
});
sl.addShape(pres.ShapeType.rect, { x: 0.2, y: 5.55, w: 9.6, h: 0.0 });
}
// ─────────────────────────────────────────────
// 12. IMAGING — CTA GOLD STANDARD
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 6 — Investigations");
slideTitle(sl, "Imaging — CT Angiography (Gold Standard)");
// CTA key info
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 1.62, w: 5.6, h: 0.35,
fill: { color: C.navy }, line: { color: C.navy } });
sl.addText("CTA — Sensitivity 93%, Specificity 96% | BIPHASIC protocol (arterial + venous phase)", {
x: 0.3, y: 1.63, w: 5.5, h: 0.32,
fontSize: 10, bold: true, color: C.white
});
sl.addText([
bullet("BIPHASIC CTA: arterial phase + delayed venous phase — evaluates both arteries & portal/mesenteric veins", 8),
{ text: "\nCT Findings with >97% Specificity:", options: { bold: true, fontSize: 12, color: C.red, breakLine: true, paraSpaceAfter: 2 } },
bullet("Pneumatosis intestinalis — intramural gas", 12),
bullet("Portal venous / SMV gas", 12),
bullet("SMA or celiac artery occlusion (filling defect)", 12),
bullet("Arterial embolism — intraluminal filling defect", 12),
{ text: "\nOther Findings:", options: { bold: true, fontSize: 12, color: C.teal, breakLine: true, paraSpaceAfter: 2 } },
bullet("Bowel wall thickening / thinning (paper-thin = transmural necrosis)", 12),
bullet("Mesenteric fat stranding", 12),
bullet("Absent bowel wall enhancement = full-thickness ischaemia", 12),
bullet("Ascites (peritoneal fluid) — late sign", 12),
], { x: 0.3, y: 2.0, w: 5.55, h: 3.4 });
// Right panel — other modalities
sl.addShape(pres.ShapeType.rect, { x: 6.1, y: 1.62, w: 3.65, h: 0.35,
fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("Other Imaging Modalities", {
x: 6.15, y: 1.63, w: 3.55, h: 0.32,
fontSize: 10, bold: true, color: C.white
});
const modalities = [
{ name: "Plain X-ray", note: "Initial screen; late: ileus, thumbprinting, pneumatosis, portal gas. NEVER to exclude AMI." },
{ name: "Duplex US", note: "Best for CMI: SMA PSV >275 cm/s = >70% stenosis. Sensitivity 92%, Specificity 96%." },
{ name: "Conventional Angiography", note: "Definitive diagnosis + simultaneous endovascular Rx (thrombolysis, vasodilators)." },
{ name: "MRA", note: "Non-radiation alternative for CMI work-up; limited in acute setting." },
];
let yy = 2.02;
modalities.forEach(m => {
sl.addText([
{ text: m.name + ": ", options: { bold: true, fontSize: 11, color: C.navy } },
{ text: m.note, options: { fontSize: 10.5, color: C.darkText } }
], { x: 6.1, y: yy, w: 3.65, h: 0.65, wrap: true });
yy += 0.82;
});
}
// ─────────────────────────────────────────────
// 13. DIAGNOSTIC FLOWCHART
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 6 — Investigations");
slideTitle(sl, "Diagnostic Algorithm — Suspected AMI");
// Flowchart using shapes
function box(sl, x, y, w, h, color, text, textColor, fs) {
sl.addShape(pres.ShapeType.rect, { x, y, w, h, fill: { color }, line: { color } });
sl.addText(text, { x, y, w, h, fontSize: fs || 11, bold: true, color: textColor || C.white, align: "center", valign: "middle", wrap: true });
}
function arw(sl, x, y, len, vert) {
if (vert) {
sl.addShape(pres.ShapeType.line, { x, y, w: 0, h: len, line: { color: C.midText, width: 1.5 } });
} else {
sl.addShape(pres.ShapeType.line, { x, y, w: len, h: 0, line: { color: C.midText, width: 1.5 } });
}
}
// Start
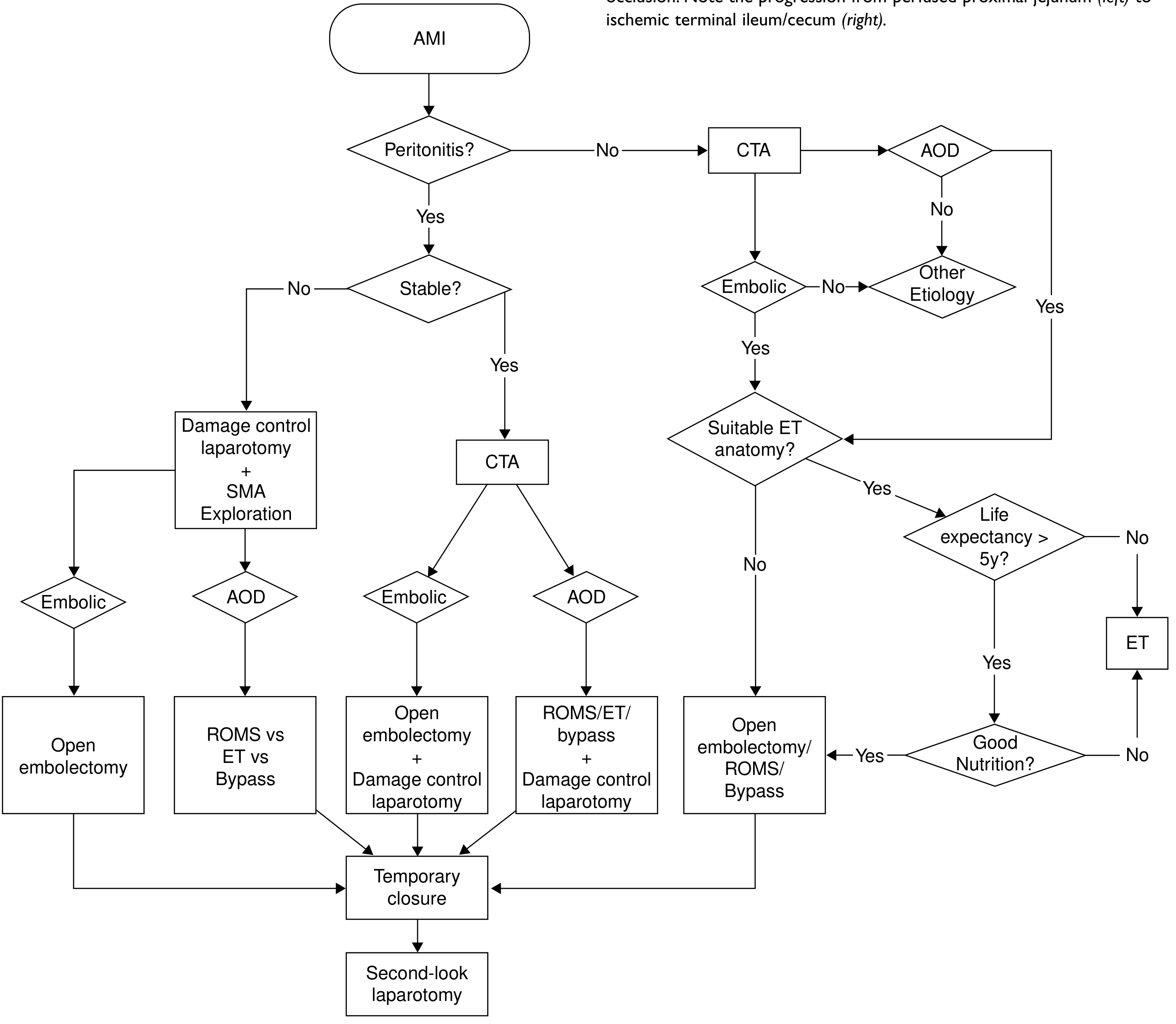
box(sl, 3.5, 1.55, 3.0, 0.44, C.red, "SUSPECTED AMI\nElderly + Abdo Pain", C.white, 10.5);
arw(sl, 5.0, 1.99, 0, 0.22, true);
// CTA
box(sl, 2.8, 2.21, 4.4, 0.44, C.navy, "CT ANGIOGRAPHY (Biphasic CTA)", C.white, 10.5);
arw(sl, 5.0, 2.65, 0, 0.22, true);
// Decision diamond (rectangle as proxy)
box(sl, 2.9, 2.87, 4.2, 0.5, C.orange, "PERITONITIS / Bowel Necrosis?", C.white, 11);
// YES → left
arw(sl, 2.9, 3.12, -1.8, 0, false);
sl.addText("YES", { x: 1.55, y: 3.01, w: 0.6, h: 0.22, fontSize: 10, color: C.red, bold: true });
box(sl, 0.25, 3.3, 2.65, 0.55, C.red, "EMERGENT\nLAPAROTOMY", C.white, 11);
arw(sl, 1.57, 3.85, 0, 0.22, true);
box(sl, 0.25, 4.07, 2.65, 0.55, C.red, "Revascularize FIRST\nResect necrotic bowel\nTemp closure", C.white, 9.5);
arw(sl, 1.57, 4.62, 0, 0.22, true);
box(sl, 0.25, 4.84, 2.65, 0.44, "922B21", "Second-look 24–48 hrs", C.white, 10.5);
// NO → right
arw(sl, 7.1, 3.12, 1.8, 0, false);
sl.addText("NO", { x: 7.2, y: 3.01, w: 0.5, h: 0.22, fontSize: 10, color: C.green, bold: true });
box(sl, 8.9, 3.3, 0.85, 0.55, C.teal, "Consider\nEndovascular", C.white, 8.5);
arw(sl, 9.32, 3.85, 0, 0.22, true);
box(sl, 8.6, 4.07, 1.15, 0.55, C.teal, "PTA/Stent\nThrombolysis\nEmbolectomy", C.white, 8.5);
// Centre - specific paths
arw(sl, 5.0, 3.37, 0, 0.22, true);
box(sl, 3.7, 3.59, 2.6, 0.44, C.teal, "Identify Subtype:\nEmbolism / Thrombosis / NOMI / MVT", C.white, 9);
arw(sl, 5.0, 4.03, 0, 0.22, true);
box(sl, 3.7, 4.25, 2.6, 0.55, C.navy, "Subtype-directed\nmanagement\n(see next slides)", C.white, 10);
}
// ─────────────────────────────────────────────
// 14. INITIAL MANAGEMENT — RESUSCITATION
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 7 — Management of AMI");
slideTitle(sl, "Initial Management — Resuscitation", "Start Immediately — Do NOT Delay Surgical Planning");
// Flowchart-style checklist
const steps = [
{ num: "1", head: "IV Access & Fluids", body: "Large-bore IV access · Crystalloid fluid resuscitation · Haemodynamic monitoring (A-line, CVP, urinary catheter)" },
{ num: "2", head: "Monitoring & Decompression", body: "NG tube decompression · Correct electrolyte abnormalities · Continuous ECG and pulse oximetry" },
{ num: "3", head: "Anticoagulation", body: "IV Unfractionated Heparin (UFH) — prevents further thrombus propagation · Continue throughout perioperative period" },
{ num: "4", head: "Vasopressors — Caution", body: "Avoid vasoconstrictors if possible — worsen mesenteric perfusion · If required for haemodynamic support, use cautiously" },
{ num: "5", head: "Antibiotics", body: "Broad-spectrum cover (gram-negative + anaerobic) — bacterial translocation is early and universal" },
{ num: "6", head: "ICU / Surgical Team", body: "Early surgical/vascular surgery consult · Interventional radiology team on standby for endovascular option" },
];
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 1.62, w: 9.5, h: 0.3,
fill: { color: C.red }, line: { color: C.red } });
sl.addText("⚠ PERITONITIS = EMERGENT LAPAROTOMY — Do NOT wait for imaging when peritonism is present", {
x: 0.3, y: 1.63, w: 9.4, h: 0.27,
fontSize: 10.5, bold: true, color: C.white
});
steps.forEach((s, i) => {
const x = (i % 3) * 3.2 + 0.25;
const y = Math.floor(i / 3) * 1.55 + 1.98;
sl.addShape(pres.ShapeType.rect, { x, y, w: 3.0, h: 1.42,
fill: { color: "F8FAFC" }, line: { color: C.border, width: 0.8 } });
sl.addShape(pres.ShapeType.ellipse, { x: x + 0.1, y: y + 0.08, w: 0.36, h: 0.36,
fill: { color: C.navy }, line: { color: C.navy } });
sl.addText(s.num, { x: x + 0.1, y: y + 0.08, w: 0.36, h: 0.36, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle" });
sl.addText(s.head, { x: x + 0.5, y: y + 0.1, w: 2.45, h: 0.3, fontSize: 11, bold: true, color: C.navy });
sl.addText(s.body, { x: x + 0.1, y: y + 0.44, w: 2.85, h: 0.94, fontSize: 10, color: C.darkText, wrap: true });
});
}
// ─────────────────────────────────────────────
// 15. SURGICAL MANAGEMENT FLOWCHART
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 7 — Management of AMI");
slideTitle(sl, "Surgical Management — Open Surgery");
// Two columns: Embolectomy and Bypass
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 1.6, w: 4.6, h: 0.36,
fill: { color: C.red }, line: { color: C.red } });
sl.addText("SMA EMBOLECTOMY (Embolic AMI — Gold Standard)", {
x: 0.3, y: 1.61, w: 4.5, h: 0.33,
fontSize: 10.5, bold: true, color: C.white
});
const embSteps = [
"Midline laparotomy",
"Colon reflected cephalad; small bowel to patient's right",
"Expose SMA at base of transverse colon mesentery",
"Intraoperative Doppler → localise loss of signal",
"Transverse arteriotomy at SMA (reduces risk of stenosis vs. longitudinal)",
"Fogarty balloon catheter embolectomy proximal + distal",
"Completion angioscopy or on-table angiography",
"Assess bowel viability (fluorescein + Doppler)",
"Resect ONLY frankly necrotic bowel",
"Temporary abdominal closure → Second-look 24–48 hrs"
];
sl.addText(embSteps.map((t, i) => ({
text: `${i + 1}. ${t}`,
options: { fontSize: 10.8, color: C.darkText, bullet: false, breakLine: true, paraSpaceAfter: 3 }
})), { x: 0.3, y: 2.0, w: 4.5, h: 3.35 });
sl.addShape(pres.ShapeType.line, { x: 4.97, y: 1.6, w: 0, h: 3.8, line: { color: C.border, width: 0.8 } });
sl.addShape(pres.ShapeType.rect, { x: 5.15, y: 1.6, w: 4.6, h: 0.36,
fill: { color: C.navy }, line: { color: C.navy } });
sl.addText("MESENTERIC BYPASS (Thrombotic AMI / CMI)", {
x: 5.2, y: 1.61, w: 4.5, h: 0.33,
fontSize: 10.5, bold: true, color: C.white
});
sl.addText([
{ text: "Antegrade Bypass (Supraceliac inflow):\n", options: { bold: true, fontSize: 11, color: C.teal, breakLine: true } },
bullet("Inflow: supraceliac / distal thoracic aorta", 8),
bullet("Bifurcated Dacron graft (12×6 or 14×7 cm) for celiac + SMA", 8),
bullet("Less kinking; preferred in younger/fitter patients", 8),
bullet("Transperitoneal: mobilise left liver lobe; divide left crus of diaphragm", 8),
{ text: "\nRetrograde Bypass (Infrarenal inflow):\n", options: { bold: true, fontSize: 11, color: C.orange, breakLine: true } },
bullet("Inflow: infrarenal aorta or iliac artery", 8),
bullet("PTFE or Dacron graft — C-loop or J-loop configuration to prevent kinking", 8),
bullet("Preferred in emergency or when heavy supraceliac disease", 8),
{ text: "\nEndarterectomy:\n", options: { bold: true, fontSize: 11, color: C.green, breakLine: true } },
bullet("Transaortic endarterectomy: trapdoor aortotomy; removes plaque", 8),
bullet("Best for ostial lesions; requires aortic cross-clamp", 8),
], { x: 5.2, y: 2.0, w: 4.5, h: 3.35 });
}
// ─────────────────────────────────────────────
// 16. SECOND LOOK + BOWEL VIABILITY
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 7 — Management of AMI");
slideTitle(sl, "Second-Look Laparotomy & Bowel Viability Assessment");
// Principle banner
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 1.62, w: 9.5, h: 0.32,
fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("PRINCIPLE: Revascularize First → Resect ONLY Dead Bowel → Temp Closure → Second-Look 24–48 hrs → Definitive Closure", {
x: 0.3, y: 1.63, w: 9.4, h: 0.29,
fontSize: 10, bold: true, color: C.white
});
// Viability table
const rows = [
[
{ text: "Assessment Method", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Viable Findings", options: { bold: true, color: C.white, fill: { color: "1E8449" } } },
{ text: "Non-Viable Findings", options: { bold: true, color: C.white, fill: { color: "C0392B" } } },
],
["Visual (colour)", "Pink / red, glistening serosa", "Black / green / grey, dull / mottled"],
["Peristalsis", "Present — good prognostic sign", "Absent"],
["Wall thickness & turgor", "Normal thickness, firm", "Thin (paper-thin) or oedematous"],
["Mesenteric pulse", "Palpable arterial pulsation", "Absent pulsation"],
["Intraop Doppler", "Audible Doppler signal at antimesenteric border", "Loss of signal = no flow"],
["IV Fluorescein + Wood's lamp", "Bright fluorescence under UV light", "No fluorescence = necrosis"],
["Subserosal haemorrhage", "Absent / minimal", "Extensive = concerning"],
];
sl.addTable(rows, {
x: 0.2, y: 2.0, w: 9.6, h: 3.35,
colW: [2.4, 3.6, 3.6],
border: { type: "solid", color: C.border, pt: 0.5 },
fill: { color: C.tableAlt },
rowH: 0.41,
fontFace: "Calibri",
fontSize: 11,
color: C.darkText,
align: "left",
valign: "middle",
});
sl.addShape(pres.ShapeType.rect, { x: 0.2, y: 5.4, w: 9.6, h: 0.37,
fill: { color: "FEF9E7" }, line: { color: C.orange, width: 1 } });
sl.addText("Preserve ALL questionable bowel at first operation. Second-look allows recovery of marginal segments. < 100–150 cm small bowel remaining = Short Bowel Syndrome.", {
x: 0.3, y: 5.43, w: 9.4, h: 0.32,
fontSize: 10, color: C.orange
});
}
// ─────────────────────────────────────────────
// 17. ENDOVASCULAR MANAGEMENT
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 7 — Management");
slideTitle(sl, "Endovascular Management — AMI & CMI");
const rows = [
[
{ text: "Technique", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Indication", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Key Points", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
],
[
{ text: "Percutaneous transluminal angioplasty (PTA)", options: {} },
"CMI — short segment stenosis",
"Balloon dilation; may need adjunct stent; restenosis ~30% without stent"
],
[
{ text: "Primary Stenting", options: {} },
"CMI first-line / AMI without peritonitis",
"Balloon-expandable COVERED stent preferred; traps plaque, prevents embolism"
],
[
{ text: "Intra-arterial thrombolysis", options: {} },
"Acute thrombosis / embolism (no peritonitis)",
"Papaverine or tPA; allows simultaneous diagnostic angiography; cannot assess bowel viability"
],
[
{ text: "Pharmaco-mechanical embolectomy", options: {} },
"Embolic AMI — early, no peritonitis",
"Aspiration + thrombolytics; hybrid with open if needed"
],
[
{ text: "Intraarterial vasodilators (NOMI)", options: {} },
"NOMI — no peritonitis",
"Papaverine infusion 30–60 mg/hr into SMA; most studied. Alternatively nitroglycerin / prostaglandins"
],
];
sl.addTable(rows, {
x: 0.2, y: 1.6, w: 9.6, h: 3.7,
colW: [2.6, 2.8, 4.2],
border: { type: "solid", color: C.border, pt: 0.5 },
fill: { color: C.tableAlt },
rowH: 0.6,
fontFace: "Calibri",
fontSize: 11,
color: C.darkText,
align: "left",
valign: "middle",
});
// Access technique note
sl.addShape(pres.ShapeType.rect, { x: 0.2, y: 5.37, w: 9.6, h: 0.42,
fill: { color: "EBF5FB" }, line: { color: C.teal, width: 1 } });
sl.addText("Access: Femoral or brachial approach · Selective angled catheters · Systemic heparin after access · Balloon diameter = reference vessel diameter · Post-procedure antiplatelet ≥ 6 months", {
x: 0.3, y: 5.4, w: 9.4, h: 0.36,
fontSize: 10, color: C.teal
});
}
// ─────────────────────────────────────────────
// 18. CMI — WORKUP & REVASCULARIZATION TABLE
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 8 — Chronic Mesenteric Ischemia");
slideTitle(sl, "Chronic Mesenteric Ischemia — Workup & Revascularization");
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 1.62, w: 9.5, h: 0.3,
fill: { color: "EBF5FB" }, line: { color: C.teal, width: 1 } });
sl.addText("Requires ≥ 2 of 3 vessels (Celiac, SMA, IMA) with significant stenosis/occlusion for symptoms. Atherosclerosis is the most common aetiology.", {
x: 0.3, y: 1.64, w: 9.4, h: 0.26,
fontSize: 10.5, color: C.navy, italic: true
});
const rows = [
[
{ text: "CMI Assessment Step", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Details", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
],
[{ text: "Clinical criteria", options: { bold: true } }, "Classic triad: postprandial pain + food fear + weight loss; r/o malignancy first"],
[{ text: "Duplex US", options: { bold: true } }, "SMA PSV >275 cm/s; EDV >45 cm/s = >70% stenosis. Sensitivity 92%, Specificity 96%"],
[{ text: "CT/MR Angiography", options: { bold: true } }, "Defines anatomy, collaterals, degree of stenosis; plan revascularisation"],
[{ text: "Endovascular (1st line)", options: { bold: true } }, "Balloon-expandable COVERED stent; 70–80% of CMI procedures; primary patency 75–80% at 3 yrs"],
[{ text: "Open bypass — Antegrade", options: { bold: true } }, "Supraceliac inflow; bifurcated Dacron; preferred in younger/fitter; superior long-term patency"],
[{ text: "Open bypass — Retrograde", options: { bold: true } }, "Infrarenal/iliac inflow; C or J-loop graft; preferred in elderly/high risk"],
[{ text: "Transaortic endarterectomy", options: { bold: true } }, "Best for ostial/flush lesions; trapdoor aortotomy; multi-vessel simultaneous treatment"],
[{ text: "Post-procedure care", options: { bold: true } }, "Oral feed when symptoms allow; nutrition rehab; duplex surveillance at 1, 6, 12 months then annually"],
];
sl.addTable(rows, {
x: 0.2, y: 1.97, w: 9.6, h: 3.7,
colW: [2.8, 6.8],
border: { type: "solid", color: C.border, pt: 0.5 },
fill: { color: C.tableAlt },
rowH: 0.41,
fontFace: "Calibri",
fontSize: 11,
color: C.darkText,
align: "left",
valign: "middle",
});
}
// ─────────────────────────────────────────────
// 19. OUTCOMES & SPECIAL SCENARIOS
// ─────────────────────────────────────────────
{
const sl = addSlide();
sectionBanner(sl, "Section 9 — Outcomes & Special Scenarios");
slideTitle(sl, "Outcomes Summary & Special Scenarios");
// Outcomes grid
const outcomes = [
{ label: "Overall AMI Mortality", val: "17–21%", color: C.red },
{ label: "Thrombotic (untreated)", val: "77%", color: "7B241C" },
{ label: "Embolic (untreated)", val: "54%", color: C.red },
{ label: "Open Repair (2010)", val: "33%", color: C.orange },
{ label: "Endovascular (2010)", val: "15%", color: C.green },
{ label: "ICU-admitted AMI", val: "> 70%", color: "7B241C" },
];
outcomes.forEach((o, i) => {
const x = (i % 3) * 3.18 + 0.25;
const y = Math.floor(i / 3) * 0.95 + 1.62;
sl.addShape(pres.ShapeType.rect, { x, y, w: 3.0, h: 0.82, fill: { color: o.color }, line: { color: o.color } });
sl.addText(o.val, { x, y: y + 0.02, w: 3.0, h: 0.46, fontSize: 22, bold: true, color: C.white, align: "center", valign: "middle" });
sl.addText(o.label, { x, y: y + 0.48, w: 3.0, h: 0.32, fontSize: 9.5, color: C.white, align: "center" });
});
// Special scenarios
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 3.6, w: 9.5, h: 0.3,
fill: { color: C.navy }, line: { color: C.navy } });
sl.addText("Special Clinical Scenarios", {
x: 0.3, y: 3.61, w: 9.4, h: 0.27,
fontSize: 11, bold: true, color: C.white
});
const rows = [
[
{ text: "Scenario", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
{ text: "Key Management Points", options: { bold: true, color: C.white, fill: { color: C.tableHdr } } },
],
["Spontaneous SMA Dissection (SISMAD)", "Rare; males, East Asian. Asymptomatic → antiplatelet. Mild → anticoagulation. Persistent pain/aneurysm → endovascular stenting."],
["Post-aortic surgery ischaemic colitis", "Ligation of IMA during aortic repair; sigmoid most at risk. Monitor postop. Flexible sigmoidoscopy if suspected."],
["Short Bowel Syndrome", "< 100–150 cm small bowel = lifelong TPN dependency. Prevention: revascularise first, preserve marginal segments, second-look."],
["Median Arcuate Ligament Syndrome", "Extrinsic celiac compression by diaphragmatic crus. Treatment: ligament division ± celiac reconstruction."],
];
sl.addTable(rows, {
x: 0.2, y: 3.95, w: 9.6, h: 1.65,
colW: [2.8, 6.8],
border: { type: "solid", color: C.border, pt: 0.5 },
fill: { color: C.tableAlt },
rowH: 0.38,
fontFace: "Calibri",
fontSize: 10.5,
color: C.darkText,
align: "left",
valign: "middle",
});
}
// ─────────────────────────────────────────────
// 20. KEY TAKE-AWAYS / CLOSING SLIDE
// ─────────────────────────────────────────────
{
const sl = addSlide(C.navy);
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.18, fill: { color: C.teal }, line: { color: C.teal } });
sl.addText("SURGICAL TAKE-AWAYS", {
x: 0.4, y: 0.25, w: 9.2, h: 0.55,
fontSize: 24, bold: true, color: C.white, align: "center", charSpacing: 2
});
const msgs = [
{ num: "01", text: "Pain OUT OF PROPORTION to examination = AMI until proven otherwise. High index of suspicion is the first life-saving step." },
{ num: "02", text: "No laboratory test can exclude AMI. CT angiography (biphasic) is the gold standard — specificity > 97% for key findings." },
{ num: "03", text: "PERITONITIS = Emergent laparotomy. Do NOT delay for imaging when peritonism is present." },
{ num: "04", text: "Revascularise FIRST — resect only clearly dead bowel. Preserve questionable segments for second-look at 24–48 hours." },
{ num: "05", text: "NOMI: treat the underlying cause + intraarterial vasodilators. MVT: anticoagulate. Tailor treatment to subtype." },
{ num: "06", text: "CMI: Endovascular (covered stent) is first-line for most; open bypass for younger/fitter patients with superior long-term durability." },
];
msgs.forEach((m, i) => {
const x = (i % 2) * 4.9 + 0.25;
const y = Math.floor(i / 2) * 1.38 + 0.88;
sl.addShape(pres.ShapeType.rect, { x, y, w: 4.65, h: 1.28, fill: { color: "122540" }, line: { color: C.teal, width: 0.8 } });
sl.addShape(pres.ShapeType.ellipse, { x: x + 0.12, y: y + 0.1, w: 0.42, h: 0.42, fill: { color: C.teal }, line: { color: C.teal } });
sl.addText(m.num, { x: x + 0.12, y: y + 0.1, w: 0.42, h: 0.42, fontSize: 11, bold: true, color: C.white, align: "center", valign: "middle" });
sl.addText(m.text, { x: x + 0.6, y: y + 0.12, w: 3.95, h: 1.04, fontSize: 10.5, color: "C8D8E8", wrap: true });
});
sl.addShape(pres.ShapeType.rect, { x: 0, y: 5.2, w: 10, h: 0.42, fill: { color: "0A1929" }, line: { color: "0A1929" } });
sl.addText("Based on: Schwartz's Principles of Surgery 11e · Sabiston Textbook of Surgery · Current Surgical Therapy 14e · 2026", {
x: 0.4, y: 5.24, w: 9.2, h: 0.34,
fontSize: 9, color: "5A7A9A", align: "center"
});
}
// ─────────────────────────────────────────────
// WRITE FILE
// ─────────────────────────────────────────────
const outPath = "/home/daytona/workspace/mesenteric-ischemia/Mesenteric_Ischemia_Merged.pptx";
pres.writeFile({ fileName: outPath })
.then(() => console.log("SUCCESS: " + outPath))
.catch(e => { console.error("ERROR:", e); process.exit(1); });
cd /home/daytona/workspace/mesenteric-ischemia && npm install pptxgenjs --save 2>&1 | tail -3 && echo "NPM_DONE"
Make it
ls /home/daytona/workspace/mesenteric-ischemia/ && node -e "require('pptxgenjs'); console.log('pptxgenjs OK')" 2>&1
cd /home/daytona/workspace/mesenteric-ischemia && node build.js 2>&1
ls -lh /home/daytona/workspace/mesenteric-ischemia/Mesenteric_Ischemia_Merged.pptx
Mesenteric Ischemia Merged
Presentation · PPTX
| # | Slide | Format |
|---|---|---|
| 1 | Title Slide | Visual layout — dark navy bg |
| 2 | Lecture Outline | Two-column list |
| 3 | Historical Perspective + Epidemiology | Table + callout box |
| 4 | Classification of Mesenteric Ischemia | 5-type comparison table |
| 5 | Vascular Anatomy & Collaterals | Diagram (shapes) + bullet points |
| 6 | Pathophysiology — Ischemia Timeline | Colour-coded flowchart (0–3h → 3–6h → >6h → Death) |
| 7 | Embolic vs. Thrombotic AMI | Side-by-side comparison table |
| 8 | NOMI & Mesenteric Venous Thrombosis | Two-column layout |
| 9 | Clinical Presentation | AMI vs CMI two-column layout |
| 10 | Differential Diagnosis | 3-column table (surgical / GI / vascular) |
| 11 | Laboratory Investigations | 8-row table with significance column |
| 12 | CT Angiography — Gold Standard | Findings list + other modalities panel |
| 13 | Diagnostic Algorithm | Decision flowchart (peritonitis? YES/NO branches) |
| 14 | Initial Resuscitation | 6-step numbered grid |
| 15 | Open Surgery (Embolectomy + Bypass) | Step-by-step two-column layout |
| 16 | Second-Look Laparotomy + Bowel Viability | Viability assessment table |
| 17 | Endovascular Management | Techniques table (PTA, stent, thrombolysis, NOMI) |
| 18 | Chronic Mesenteric Ischemia | Workup + revascularization table |
| 19 | Outcomes + Special Scenarios | Mortality stat grid + scenarios table |
| 20 | Key Take-Aways | 6 message cards on dark background |
Kindly add epidemiology & risk factor part from one of these ppt that i uploaded to this new ppt that you made
timeout 30 python3 -c " import zipfile, re def get_slide(path, nums): with zipfile.ZipFile(path, 'r') as z: for n in nums: sname = f'ppt/slides/slide{n}.xml' try: content = z.read(sname).decode('utf-8', errors='ignore') texts = re.findall(r'<a:t[^>]*>(.*?)</a:t>', content, re.DOTALL) print(f'--- {path} slide{n} ---') print(' | '.join([t.strip() for t in texts if t.strip()])) except: pass # PPT2 slides 5 (epidemiology) and 6 (risk factors) get_slide('/home/daytona/workspace/mesenteric-ischemia/ppt2.pptx', [5, 6]) " 2>&1
~/mesenteric-ischemia/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/mesenteric-ischemia/build.js'
cd /home/daytona/workspace/mesenteric-ischemia && node build.js 2>&1
ls -lh /home/daytona/workspace/mesenteric-ischemia/Mesenteric_Ischemia_Merged.pptx
Mesenteric Ischemia Merged
Presentation · PPTX
- Left column: 6 stat boxes (incidence, demographics) with teal value tiles
- Right column: Mortality table by scenario (overall AMI, ICU, thrombotic, embolic, NOMI)
- Bottom: Trends 1999–2010 table (open vs. endovascular mortality, diagnosis delay impact)
- Source cited: Sabiston · Current Surgical Therapy 14e · Schwartz 11e
- Full 4-column table covering all four subtypes side-by-side:
- Embolic AMI (AF, LV thrombus, valvular disease...)
- Thrombotic AMI (atherosclerosis/PVD, hypercoagulable states...)
- NOMI (critical illness, vasopressors, post-cardiac surgery...)
- Mesenteric Venous Thrombosis (Factor V Leiden, APS, JAK2, malignancy...)
- Bottom callout: "68% of embolic AMI have simultaneous emboli elsewhere"
Suggest me some figure to add in the abode presentation taken from standard textbooks
Search multiple medical textbooks for figures (images) related to mesenteric ischemia. Use query_library_db and read_file tools to find image URLs embedded in the textbook markdown files. Specifically search these files for any lines containing "![" (markdown image syntax) within the mesenteric ischemia sections: 1. Schwartz's Principles of Surgery: /textbooks/9781259835346/9781259835346_block14.md — read from offset 316 to around 380 (the mesenteric ischemia section ends around line 380) 2. Current Surgical Therapy 14e: /textbooks/9780323796835/9780323796835_block12.md — read around lines 3160–3400 (mesenteric ischemia sections) 3. Sleisenger & Fordtran's GI: /textbooks/9780323609623/9780323609623_block2.md — read around lines 2723–2900 4. Sleisenger & Fordtran's GI block31: /textbooks/9780323609623/9780323609623_block31.md — read around lines 2932–3100 For each file, read in chunks of 100 lines. Look for lines that contain "![" (markdown image syntax) and extract: - The image alt text (description inside ![...]) - The image URL (inside the parentheses) - The figure caption (the line immediately after the image, usually starting with *Figure...) - Which textbook it came from - The line number Return a complete list of ALL figure URLs found, with their captions and which textbook/slide context they belong to. This is for a surgical presentation on mesenteric ischemia.
Recommended Textbook Figures for Your Presentation
🫀 SLIDE 5 — Vascular Anatomy
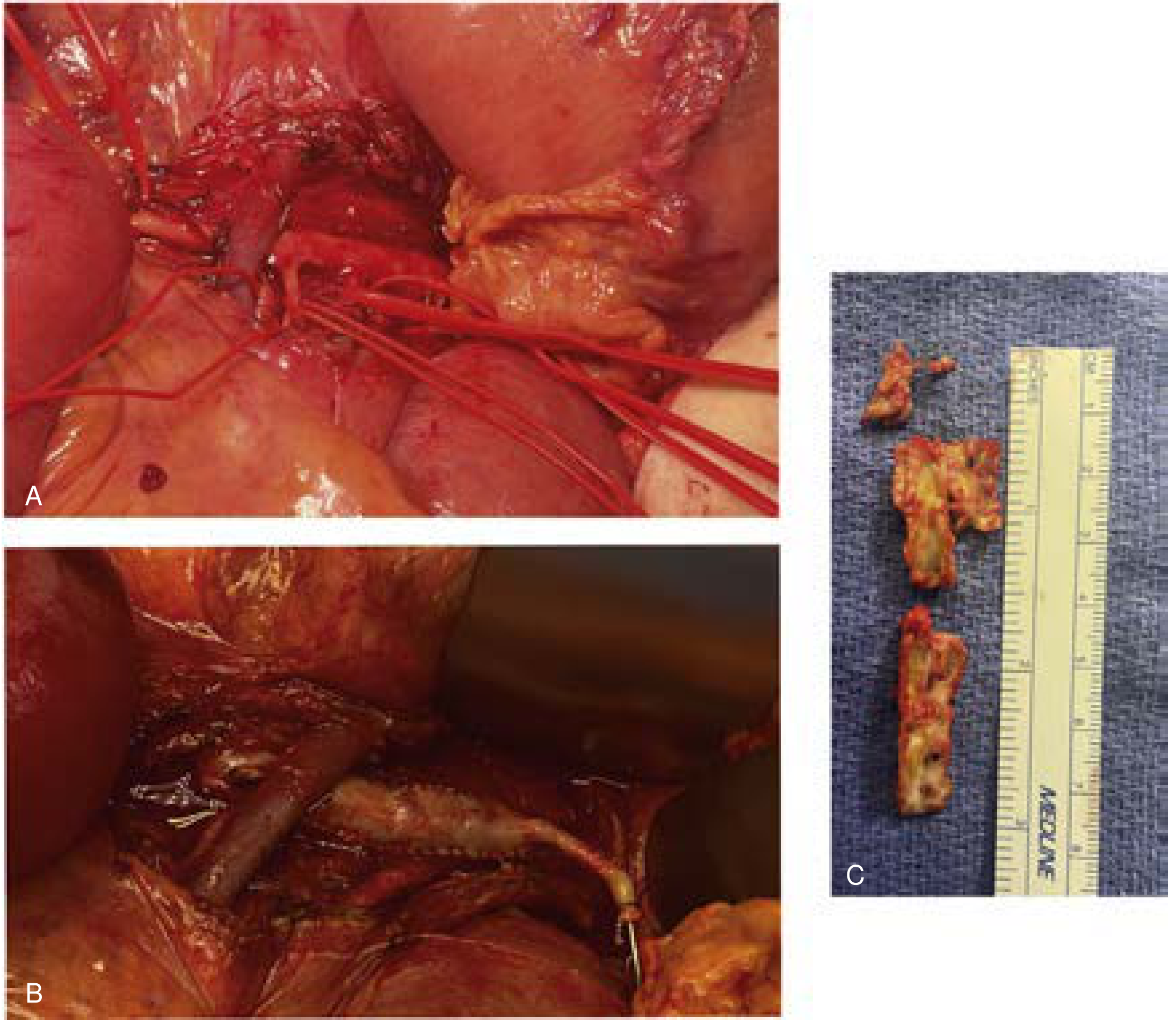
🔴 SLIDE 7 — Classification / Pathophysiology (Gross Surgical Photo)

🔀 SLIDE 13 — Diagnostic Algorithm
🔪 SLIDE 15 — Open Surgical Technique
🩻 SLIDE 12 — Imaging (Angiography)
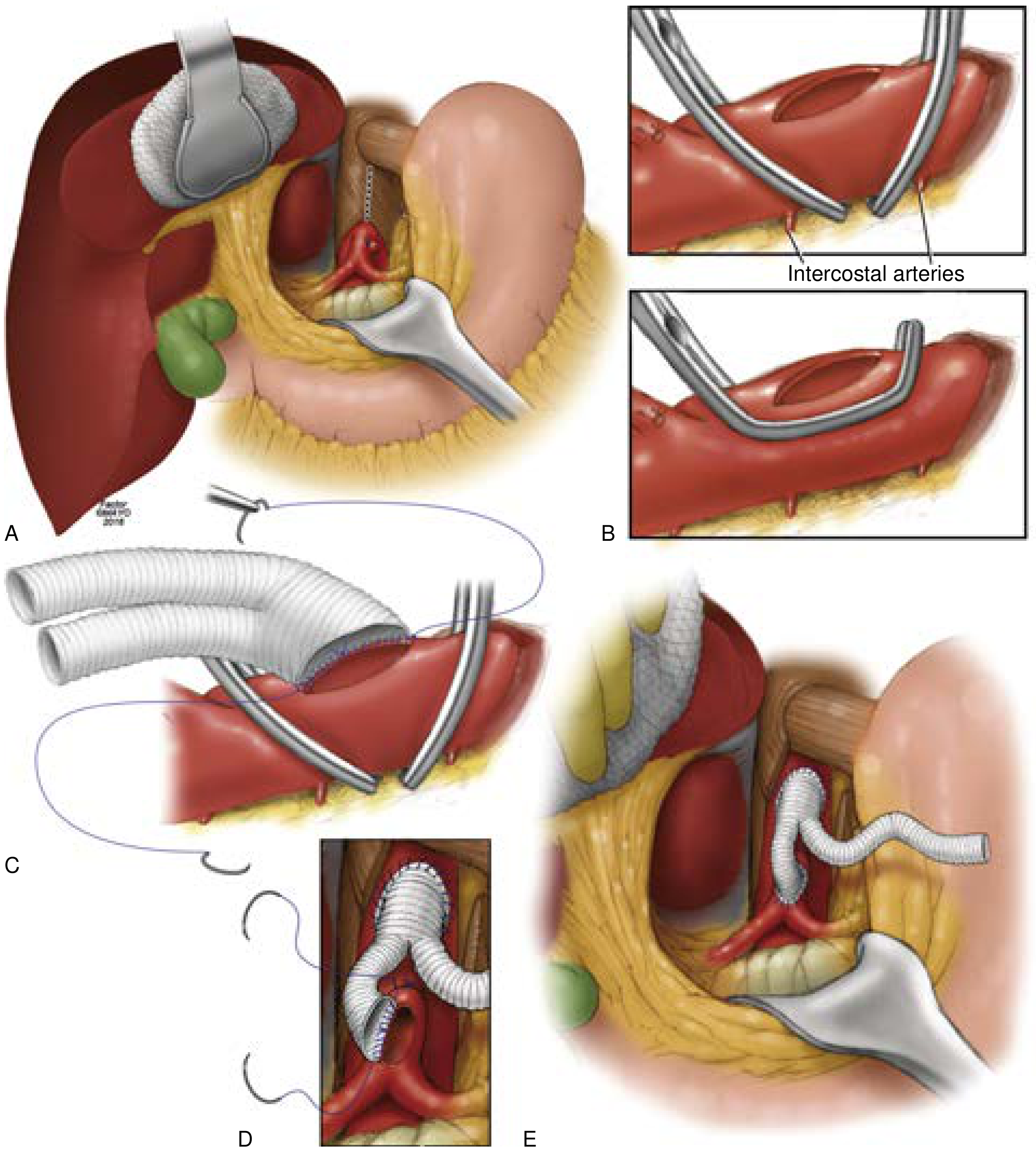
🏥 SLIDE 15 — Antegrade Bypass
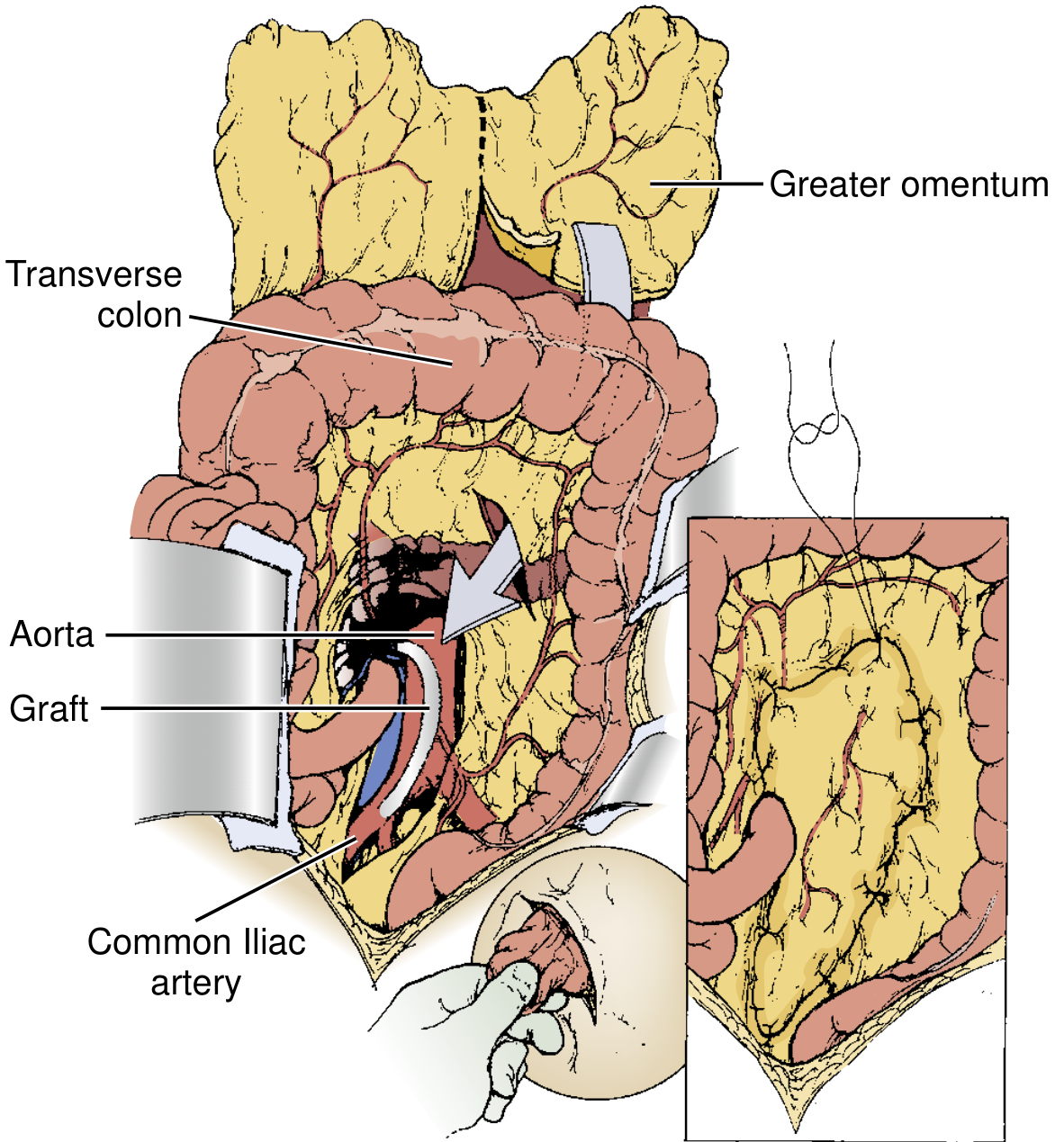
🩹 SLIDE 15 — Retrograde Bypass / Omental Coverage
🔬 SLIDE 16 — Second Look / Endarterectomy
Summary Table — Where to Add Each Figure
| Figure | Source | Best Slide |
|---|---|---|
| FIG. 1 — Mesenteric arterial tree + collaterals | Current Surgical Therapy 14e | Slide 5 — Vascular Anatomy |
| FIG. 2 — Ischemic bowel intraop photo | Current Surgical Therapy 14e | Slide 6/7 — Pathophysiology |
| FIG. 3 — Open vs. endovascular algorithm | Current Surgical Therapy 14e | Slide 13 — Diagnostic Algorithm |
| FIG. 4 — SMA operative exposure diagram | Current Surgical Therapy 14e | Slide 15 — Open Surgery |
| FIG. 6 — Omental graft coverage | Current Surgical Therapy 14e | Slide 15 — Bypass technique |
| FIG. 7 — Antegrade bypass (A–E panels) | Current Surgical Therapy 14e | Slide 15 — Bypass technique |
| FIG. 11 — Endarterectomy intraop | Current Surgical Therapy 14e | Slide 16 — Second look |
| Fig. 118.8 — SMA angiogram (embolus + papaverine) | Sleisenger & Fordtran | Slide 12 — Imaging |
Create a new diagnostic imaging slide with CT/plain film/angiography images from Sleisenger